Aside ~ ‘The story I hate to tell’: 3 decades of slow progress followed by the slow death of a dream
Link back to part 2
1950s to 1990s
During the decades from the early 1900s to the 1950s, it was ‘business-as-usual’ for the surgical specialty of obstetrics. As many as half the births in the US were still attended by regular doctors — general practitioners or family practice physician — but all the standards for childbirth services were written by each hospital’s chief of Ob-Gyn and inevitably imposed a strict obstetrical model.
While I am not actually the nurse in the photo below, its spitting image of our OR-type delivery room, the white scrub dress we all word and me as an incredibly young and naive L&D nurse.
This woman is the same age and looks like me during the years I first worked in L&D. She is wearing the same kind of white scrub dress, cotton cap, and mask, white stocking and oxford shoes, with scissors and a pen in her pocket.
The architecture of the delivery room is identical, with the same model of delivery table, stirrups, anesthesia machine, OR light and stainless steel buckets on wheels. The nurse could even double for me as I instructed first-year nursing students in the art and science of sterile technique while of setting up equipment on the instrument table.
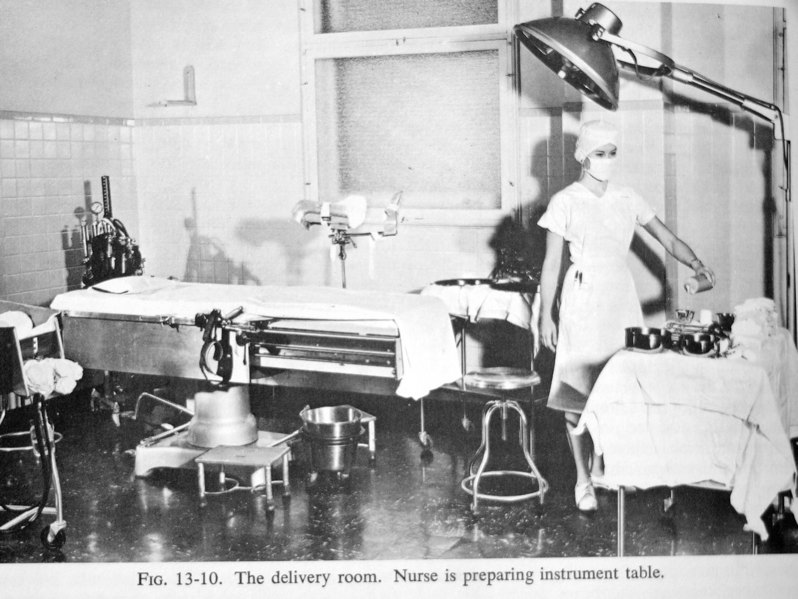
Fifty years is a long time — so long that everyone begins to think of such ‘customs’ as as handed down by Moses along with the Ten Commandments. It was reasonable to assume that childbirth in American would always take place in OR-type delivery rooms as pictured above.
After all, it seems so clean, so well-appointed with modern equipment, mysterious yet reassuringly — surely this was the best and the safest place in the whole world to have a baby. What mother wouldn’t want to be the leading lady in a drama as important and exciting as the birth of her child, as skilled professionals bustled about the room to care for her and her newborn? This type of scene is still made for good drama, as we see weekly on television’s current blockbuster hospital show, Gray’s Anatomy.
But in 1958 something happened that briefly called this medical-surgical model into question. A letter written by a ‘whistle-blower’ Labor & Delivery nurse was published in the Ladies Home Journal, which was a popular woman’s magazine. She spoke out about the routine use of dangerous obstetrical practices and the despicable way women laboring under the influence of Twilight Sleep drugs or unconscious from general anesthesia were mistreated by rude or uncaring nurses and doctors.
This was followed by a lengthy article called “Cruelty in the Maternity Wards“, which caused quite a protracted publicity buzz. Other L&D nurses confirmed the account published in the original nurse’s published letter. Childbearing women who vividly remembered being harmed or humiliated also spoke up.
It’s important to understand that for the previous fifty years, the entire intrapartum period of hospital care (labor, birth & recovery from anesthesia) occurred behind closed doors that said in big black letters: “NO ADMITTANCE — Authorized Personnel Only“. This was a specialized area of the hospital built as a closed surgical department that was restricted to hospital personnel and patients that were admitted to the unit– patients were not allowed to leave (or even get out of bed) and the family was not permitted to come in.
Labor under Twilight Sleep protocols meant that mothers-to-be were drugged and semi-conscious. The word ‘sleep’ is misleading, as women were in a profound stupor between contraction and became delirious during them. They frequently moaned, cried, screamed, occasionally hit or would bite nurses, refused to stay modestly under their covers, often tried to climb out of bed and sometimes broke an arm or chipped a tooth as the fell to the floor.
The functional effects of the drug scopolamine are the temporary equivalent of a frontal lobotomy — all executive function and all personal inhibitions are inaccessible while under its influence for as long as 48 hours.
Historically women under the influence of scopolamine were dressed in special hospital gowns with long sleeves that were sown together in the middle to make one continuous loop from each arm. This is a very low-tech yet highly efficient way to achieve the goal of a straight jacket. In many hospitals also wrapped the mother’s head in a towel to keep her from getting hurt when she banged her head on the bars of her cribbed.
 Other also placed a black hood over the laboring woman’s head to reduce visual distractions. A photo of this practice is reminiscent of those that came out of the Abu Garab torture scandal during the Afghanistan War.
Other also placed a black hood over the laboring woman’s head to reduce visual distractions. A photo of this practice is reminiscent of those that came out of the Abu Garab torture scandal during the Afghanistan War.
 Then the new mother-to-be was put in a special adult-sized crib with 4-ft high bars. After being put in this bed, a removable canvas cover was fastened to the top of the bed to keep drugged women inside like caged animals.
Then the new mother-to-be was put in a special adult-sized crib with 4-ft high bars. After being put in this bed, a removable canvas cover was fastened to the top of the bed to keep drugged women inside like caged animals.
By the time I worked in the L&D, some of these egregious practices had been discontinued. But when our labor ward was busy (which was often), we still put drugged women in four-point restraint to keep them from falling out of bed. Using the same kind of leather restraints as the hospital psyche unit, L&D nurses (including me) fastened both the patient’s wrists and both ankles to the four corners of the bed.

This meant they could not move or turn over but instead were forced to labor for hours and hours while lying flat on their back. As their contractions stretched open the cervix, these mothers still felt the full physical effects of pain and pressure. However, the pharmaceutical effect of scopolamine blocks and therefore prevents the formation of memories.
Women given the drug scopolamine during labor cannot recall anything afterward, including the birth of their baby, because the memory was never formed in the first
place.
{Note on pharmacology of scopolamine and memory: Memory formation occurs in 3 stages: encoding (when a new memory is initially made), storage (the creation of memories) and recall (when memories are retrieved). N
eurotransmitters are bio-chemicals involved in the transfer of nerve signals.
Acetylcholine (ACh)
is a
cholinergic neurotransmitter that
transfers the electrical signals that encode our memories
. Scopolamine has an anti-cholinergic effect, which means the memory encoding effect of the acetylcholine is neutralized and no memory formation can occur.
Ref –
}
Quite obviously, this was no place for husbands. Not only would they be upset to see their own wife under these conditions but they might see things that violated the privacy of other men’s laboring wives.
During the surgical procedures of ‘delivery’, women were in OR-type delivery rooms, unconscious and in stirrups. Hospital rules for strict surgical sterility allowed only hospital personnel who were in hospital scrubs with a scrub hat and mask be permitted to enter the restricted environment of the delivery room, so husbands could never be present at the birth of their baby.
With mothers drugged or unconscious, fathers and other family members expressly excluded, there simply were NO witnesses to the practices (good, bad or indifferent) that went on in the sanctum sacrarium of the L&D unit, either from a policy standpoint or how individual patients were treated by individual staff members.
Women sometimes told disturbing stories of being mistreated, but since mothers-to-be had been given narcotics and hallucinogenic drugs, these accounts were dismissed as the product of a drugged imagination. Total lack of first-hand witnesses and the automatic discounting of those who did have the first-hand experience is similar to situations found in maximum security prisons.
According to historical reports, many other L&D nurses confirmed the account published in the original nurse’s published letter. Childbearing women who vividly remembered being harmed or humiliated also spoke up. This caused quite a protracted publicity buzz. An increasing number of people questioned the necessity and wisdom of routinely isolating women from their families during labor.
Why couldn’t they be there to be sure their wife or daughter was being properly treated by the staff? These early birth activists were also concerned about the effects of repeated injections of narcotics and the hallucinogenic-amnesic drug scopolamine during labor, routine use of general anesthesia, episiotomy and outlet forceps.
Public interest during the late 1950s and 60s was accompanied by a trickle of books that were critical of the 50-year old status quo. Most of these authors promoted unmedicated labor and ‘natural’ or spontaneous births (i.e, no forceps). The popular and influential books were “Childbirth Without Fear” by Grantly Dick Read, MD, “Husband-coached Childbirth” by Dr. Bradley and “Thank You, Dr. Lamaze”.
Slowly the idea of participatory childbirth — conscious mothers giving birth under their own power instead of having their doctors cut an episiotomy on anesthetized women and pull their babies out with forceps — gave rise to various types of childbirth education. From this came a brand new player in the maternity care field — the childbirth educator. This role is part teacher, part activist role, part friendly guide for childbearing families who wished to avoid the infamous “knock’em out, drag’em out” obstetrics.
Dashed Hopes for a Quick Fix:
I wish I could say that all this ‘consumer’ agitation brought about liberalized policies that quickly and dramatically changed ‘business-as-usual’ for the obstetrical profession. But my experience as a student nurse, and after graduation when I worked in the L&D (1962 to 1976), mirrored the reports of the nurses writing those revelatory letters in the 1950s.
Nonetheless, there were tiny increments of progress. The most avant-guard hospitals in New York City started pilot programs the late 1950s that allowed a few hand-picked dads to be present during labor and the surgically-conducted birth in the OR-type delivery room, even though the mother was often unconscious under anesthesia.

There is a famous photograph of the birth of a well-known contemporary photographer (David Miller) taken at the moment of his birth by his MD-dad, who was allowed to be in the delivery room.
Functionally speaking his mother was not present, as she had been put to sleep with anesthetic gas.
The baby and the umbilical cord shows the effects of the inhaled anesthesia as his body is limp, with arms falling over his head. The cord is not its natural plumb and purple (due to circulating blood) but instead looks like a cord after the blood stops circulating and is about to be clamped and cut. The usual reason for this is extremely slow fetal/newborn heart rate due to the depressive effect of the anesthesia his mother had received just prior to his birth.
But slowly over the next 30 years, an unambitious set of changes worked their way across the country, bigger or faster changes in big cities and smaller and slower (or none at all) in very conservative, very small, and very rural towns. The liberalization of policies was so slow that in many instances it was the obstetricians rather than the policies that change. The older OBs held their ground and just said “no”. Finally, they retired and the younger OBs took over as chief and changed the rules because the younger generation is always itching to shake things up.
There was however one very major change during the late 1960s and 1970s when the field of obstetrics gradually began to end its routine use of inhalation anesthesia during normal childbirth in most hospitals. When hospitals switch to spinal and epidural anesthesia it dramatically reduced the risks to women and babies by eliminating the use of anesthetic gases.
I wish I could say that the obstetrical profession simply decided to do this on its own obvious merit, or in response to women who wanted to actively participate in their own labors. But what actually turned the tide was the work of Dr. Virginia Apgar and the Apgar scoring system for neonates she developed in 1953.
Dr. Apgar was able to scientifically establish the detrimental effect of anesthetics gases on about-to-be-born babies when inhaled by their about-to-give-birth mothers. She did this by using the metrics of the 1, 5, and 10 minutes Apgar scores that she invented. There was an obviously depressed bodily function at the time of the birth (first ten minutes of life) for babies born to mothers who had been narcotized during labor and were unconscious from anesthesia.
These newborns were either cyanotic (blue or purple skin color) or very pale and more often than not, suffered from respiratory depression. They had low Apgar scores and frequently needed to be resuscitated. This was in contrast to mothers who did not have narcotics or general anesthesia, who typically gave birth to babies that were nice and pink at birth, cried and breathed right away and usually had Apgar scores of 9 & 10.
Faced with a growing demand by childbearing families for newborns that did not arrive limp, pale and not breathing, the obstetrical profession and hospital maternity departments saw this as an opportunity to exchange the old Twilight Sleep drug regime and general anesthesia for the new types of regional analgesia — locals, spinals and epidurals. This coincided with a natural desire by members of the obstetrical profession to brag about the good Apgar scores of the babies they delivered. It also provided what birth educators described as “awake and aware” childbirth.
What was not to like?
While these changes in the type of anesthesia used and liberalized policies that allowed husbands to be present were supposed to promote “natural birth”, there were surprisingly few substantial changes. The ignoble and long-overdue end of the infamous “knock’em out, drag’em out” obstetrics created a new subspecialty for anesthesiologists — obstetrical anesthesia — but otherwise did not unwind the Gordian Knot by even one turn. Over the last 29 years, things have gone in the opposite direction, as hospital L&D units continue to be highly medicalized environments.
Hospitals did add a lot of cosmetic changes and convenience — nicer waiting rooms for the family and they prettied up the labor rooms with attractive drapes and colored bedspreads. Linoleum floors were exchanged for classic wood flooring, while stainless steel cabinets turned into ones with blonde woodgrain. Husbands for sure, and sometimes even younger children were allowed to be present at the ‘delivery’, which was and is still conducted as a surgical procedure.
The Cesarean section rate has risen from less than 5% in 1970 to a high water mark of 32.9% in 2001. Maternal mortality in the state of California has increased from 8 per 100,000 live births in 1999 to 14 per 100K in 2007 (last year stats were available). Prematurity rate for newborns has increased from 8% in 1984 to a high of 13%. Only pressure from public health officials, and many maternity care professionals, the March of Dimes, and consumer advocates was able to slow down the epidemic of non-urgent inductions and scheduled Cesareans, both of which fuels our high prematurity rate.
More attractive and comfortable furniture is all very nice, but its not at what we hoped for or needed most. What didn’t happen was a fundamental reexamination of the basic error of 1910 – a policy that promoted high levels of obstetrical interventions applied to healthy childbearing women, even when they explicitly asked (often begged) not to be medicalized. We continued to wait for physiologically-based maternity care to once more be accepted as part of mainstream healthcare but so far, the obstetrical profession has failed us.
Continue to part 3 ~ Three strikes and you’re out!
