Brave New World Chapter 7 ~ re# subsequent chapters, rename URL to match
Originally published in 2013, updated in 2021
Chapter 7: What the (heck) does this have to do with contemporary obstetrical practices?
 This same scientifically-mandated “burden of proof” and tort laws apply to the entire premise of obstetrical care for healthy women with essentially healthy pregnancies. But unfortunately, obstetrics in America is not scientifically-based when the mother-to-be is healthy and has a normal term pregnancy (70-85% of the childbearing population in the United States).
This same scientifically-mandated “burden of proof” and tort laws apply to the entire premise of obstetrical care for healthy women with essentially healthy pregnancies. But unfortunately, obstetrics in America is not scientifically-based when the mother-to-be is healthy and has a normal term pregnancy (70-85% of the childbearing population in the United States).
The routine use of obstetrical interventions is a “wrong” use of obstetrical medicine. No scientific studies have identified the routine use of obstetrical interventions to be better (safer for mothers and babies) than simple non-interventive support for the normally progressive biology of labor and birth.
This is a shame, as obstetrics was historically developed to give doctors the ability to intervention when something went wrong and there was a complication that threatened the life or well-being of mother and/or unborn baby.
Obstetrical interventions should only be used by those who need them — women with very high-risk pregnancies, those who developed complications or suffered an obstetrical emergency. In that case, obstetrical medicine does a splendid job, for which we all (myself included as a former L&D nurse) would be enormously grateful.
The Wrong Use of Obstetrics ~ Protocols typically associated with the obstetrical model are NOT currently “evidence-based”
 Hospital admission of an obstetrical patient typically begins by immobilizing the mother-to-be in bed and immediately hooking her up to the electronic fetal monitor (EFM 89%). As a result, the vast majority of healthy labor patients spend more than 90% of their labors lying in bed. According to the University of Minnesota’s “Taking Charge” website:
Hospital admission of an obstetrical patient typically begins by immobilizing the mother-to-be in bed and immediately hooking her up to the electronic fetal monitor (EFM 89%). As a result, the vast majority of healthy labor patients spend more than 90% of their labors lying in bed. According to the University of Minnesota’s “Taking Charge” website:
 After the mother is wired up the EFM, the labor protocols for most hospitals include routinely starting an IV (66%) and restricting oral fluids (60%) and food (79%). Depending on the situation, Pitocin is 0ften started to either induce (20-to-40%) or “aumentent” (speed up) the labor (31%, or total of over 60% of all labors. An article in the Wall Street Journal (Landro, July 12, 2006) had this to say about the drugs used to induce labor and the way it is used and thought of by the obstetrical profession:
After the mother is wired up the EFM, the labor protocols for most hospitals include routinely starting an IV (66%) and restricting oral fluids (60%) and food (79%). Depending on the situation, Pitocin is 0ften started to either induce (20-to-40%) or “aumentent” (speed up) the labor (31%, or total of over 60% of all labors. An article in the Wall Street Journal (Landro, July 12, 2006) had this to say about the drugs used to induce labor and the way it is used and thought of by the obstetrical profession:
“The most common brand name is Pitocin, which is a synthetic version. It’s often used to speed or jump-start labor, but if the contractions become too strong and frequent, the uterus becomes “hyperstimulated,” which may cause tearing and slow the supply of blood and oxygen to the fetus.
Though there are no precise statistics on its use, IHI says reviews of medical-malpractice claims show oxytocin is involved in more than 50 percent of situations leading to birth trauma.
“Pitocin is used like candy in the OB world, and that’s one of the reasons for medical and legal risk,” says Carla Provost, assistant vice president at Baystate, who notes that in many hospitals it is common practice to “pit to distress” [i.e. to give progressively larger doses of Pitocin until the mother either delivers or the baby goes into fetal distress].
Among women who labor in a hospital obstetrical unit, 67% will have Epidural anesthesia. The standard “delivery” position still has the mother lying on her back, most often with her legs and feet in obstetrical stirrups. The Cesarean surgery rate in the US is currently 31%,
 According to the Listening to Mothers Survey (childbirthconnection.org) more than 90% of hospitalized women receive 7 (or more) obstetrical interventions. This includes pharmaceutical products such as narcotic drugs, labor accelerating hormones (Cytotec and prostaglandins), and obstetrical instruments such as forceps and vacuum extractors.
According to the Listening to Mothers Survey (childbirthconnection.org) more than 90% of hospitalized women receive 7 (or more) obstetrical interventions. This includes pharmaceutical products such as narcotic drugs, labor accelerating hormones (Cytotec and prostaglandins), and obstetrical instruments such as forceps and vacuum extractors.
How do we know that this is still true? Will here are the numbers from the “horse’s mouth” so to speak — peer-reviewed professional journals that publish scientific studies by obstetricians and other researchers:
According to a statement by the American College of Obstetricians (ACOG) Jun 11, 2015
Thirty percent of women in the United States have their spontaneous labors stimulated with exogenous oxytocin (Pitocin; Declercq et al., 2013) and 20 percent to 40 percent of labors are now induced.

According to the Mayo Clinic, the disadvantages of inducing labor a significant number of serious risks including:
- Failed induction 25 percent in first-time mother
- Low fetal heart rate. …
- Infection. …
- Uterine rupture. …
- Increased bleeding {hemorrhage} after delivery.
Inducing labor: When to wait, when to induce – Mayo Clinic
https://www.mayoclinic.org › in-depth › art-20047557
As published in the Journal Of Perinatal Education, a research paper titled “Healthy birth practice #4: avoid interventions unless they are medically necessary” …
link to a free PDF @ https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6503899/
“Maternity care in the United States continues to be intervention-intensive, despite substantive evidence that the routine use of intervention without medical indication increases risk for mothers and babies.“
-
-
- 89% of women experienced electronic fetal monitoring (EFM)
- 79% experienced restrictions on eating
- 67% of women who gave birth vaginally had an epidural in labor
- 66% have continuously IV infusion
- 62% received intravenous fluids at some time during labor
- 60% experienced restrictions on drinking in labor
- 31% were given Pitocin to speed up their labors
- 31% had a cesarean
- 20% had their membranes artificially ruptured
- 17 % of women had an episiotomy
-
{emphasis added by web editor}
Synopsis of scientific method as a legal standard that identifies physiological management as the evidence-based choice for healthy women
Historically the “burden of proof” as applied to medicine was known as “positivism” and is one of the foundational principles of the Scientific Age {ref: Cry and the Covenant by Morton Thompson, 1949; Emails from Professor Walters, 1991}. Individuals holding or wishing to promote a particular theory were required to prove the validity of their theories on objective grounds.
In the “big picture” of maternity care for a healthy population, it would be necessary to evaluate the overall necessity and safety of obstetrician management versus physiological management.
 |
 |
 |
| Typical labor scene – IV Pitocin, EFM, mom immobilized in bed | Normal vaginal delivery while med students in the corner watch | Preparing the mother for Cesarean surgery |
Assessing everything in light of physiologically-based care as the evidence-based standard
In the small picture we need to look at each and every procedure, drug and devise (EFM) to determine its direct safety and its potential for triggering or leading to a cascade of complications. The routine medicalization of normal labor and birth cannot be meet the burden of scientific proof any more than anyone could make a case for the use of catheters as a replacement for normal bladder function. Each of obstetrical intervention introduces unnecessary and unnatural risk when they are applied to healthy women with normal pregnancies that are not having any kind of emergency. {See references at bottom of this page}
EFM and Epidurals ~ Especially pernicious interventions
EFM and epidural are both a disproportionate part the intervention cascade — that negative category of a “gift that keeps on giving”.
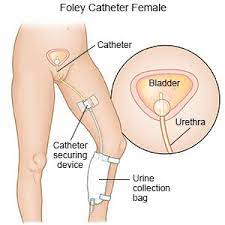
 One small example of an apparently ‘minor’ interventions associated epidural anesthesia is bladder infections. Most women with an epidural are not able to spontaneously empty their bladder because they have lost feeling in their lower body. They are also receiving large quantities of IV fluids to counteract the blood pressure lowering effects of the epidural anesthesia. So the majority of anesthetized women require urinary bladder catheterization one or more times during their labor.
One small example of an apparently ‘minor’ interventions associated epidural anesthesia is bladder infections. Most women with an epidural are not able to spontaneously empty their bladder because they have lost feeling in their lower body. They are also receiving large quantities of IV fluids to counteract the blood pressure lowering effects of the epidural anesthesia. So the majority of anesthetized women require urinary bladder catheterization one or more times during their labor.
 |
 |
 |
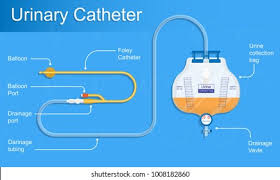
 Often an indwelling or “Foley” catheter is placed in their bladder and left in place during the many hours of labor. In some places, this Foley catheter is even left in the mother’s bladder while she pushes. However, many nurses and birth attendants see this as a dubious practice, since pushing a 30cc (one oz) Foley balloon against the inside of the urethra with every push risks damaging to it and other soft tissues. At a minimum, at least 1% of these new mothers will develop a bladder infection during the postpartum; a few will wind up with a kidney infection and the potential for all the other complications that are associated with pyelonephritis.
Often an indwelling or “Foley” catheter is placed in their bladder and left in place during the many hours of labor. In some places, this Foley catheter is even left in the mother’s bladder while she pushes. However, many nurses and birth attendants see this as a dubious practice, since pushing a 30cc (one oz) Foley balloon against the inside of the urethra with every push risks damaging to it and other soft tissues. At a minimum, at least 1% of these new mothers will develop a bladder infection during the postpartum; a few will wind up with a kidney infection and the potential for all the other complications that are associated with pyelonephritis.
EDIT line @@@@@@@@@@@@@@@
However Foley catheterization is not the only danger the mother will be exposed to, as each increment of intervention has the potential to trigger a cascade of complications. In addition to the rubber urinary catheter, she usually will have two intravenous lines, one for hydration and one for Pitocin, which is a ubiquitous accompaniment of epidural anesthesia.
The epidural requires taping a small plastic epidural catheter taped to the mother’s back, and having an automatic blood pressure cuff that goes off automatically every 15 minutes on her arm. In many hospitals, she will also have a pulse oximetry device on one of her fingers.
The electronic fetal monitor requires that two external EFM belts encircle the mother’s abdomen. Sometimes one of these belts is replaced by an internal fetal monitor leads and/or a uterine pressure catheter that goes up into her uterus. Of course, there is a Foley catheter in her bladder, with its plastic bag clamped to the lower side of the bed. Entanglement in this massive quantity of equipment (minimum of 8 wire leads and plastic tubes) effectively chains the mother to her bed and frequently requires that she remain prone and immobilized for most of the hours she is in labor.
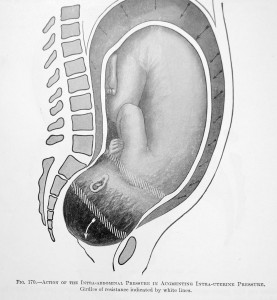
Obstetrical management of normal birth as a gravity-defying feat!
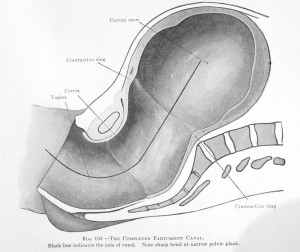
NOTE: The trajectory of the birth canal makes a 60-degree turn upward as the baby is being pushed out. A woman trying to give birth while laying on her back it trying to push a 7, 8 or 9# baby uphill, in defiance of all the laws of gravity!
Amazingly enough, the obstetrical profession — with a few well appreciated exceptions — believes that none of this in any way interferes with the natural function of the pregnant uterus or ‘spontaneous’ nature of childbearing – at least not in their minds.
The opinion of childbearing women might well be different, especially for those who finds themselves in the unlucky 30% of healthy women who wind up with operative deliveries – forceps, VE or Cesarean surgery.
Pharmaceutical and mechanical interventions do provide a number of ways for physicians to effectively control the interaction between themselves and the mother, as well as the timing, manner and circumstance of childbirth under obstetrical management.
Total control as the obstetrical goal for management of childbirth
Our 20th century technological society has long sought to control the biology of childbirth, as part of a natural desire to reduce the unexpected and inconvenient. Many Americans believes that their own superior intellect and the technological superiority of the US makes it possible to control everyone and everything including normal biology. Over the course of the last 100 years, that propensity to control bodily functions has included the use of various drugs on a routine or casual basis to manipulate bodily functions.
In the early 1900s the idea of controlling normal bowel function through the use of laxative was very popular. Eventually a public education campaign was undertaken to disabuse the public of the notion that laxatives were an “improvement” and teach that an appropriate diet and drinking water was safer and better than drug dependency.
I remember a period of time when the casual use of prescribed sleeping pills was very “in”. Eventually the down-side of their use became apparent. Barbiturates disturb the normal sleep patterns and interfere with the deep dreaming phase of sleep, which is responsible for feeling refreshed the next morning. Even more troubling was the large number of people who became dependent or addicted to sleeping bills. eventually this problems spawned a public re-education campaign that exposed the dangers of routine barbiturate use.
For a very long time, women were instructed that a “proper lady” must douche after her menstrual period and more often if she wished to be fastidious or welcomed into polite company. This notion also turned out to be without merit and to caused many unintended and even dangerous side effects requiring surgery (women who put cornstarch in the water, which with migrated up into their abdomen and caused a large tumor).
Many Americans have sought out aphrodisiacs of various kinds and now we have the dubious benefits of Viagra available to the male populations. And of course, the control of appetite and eating is our biggest favorite with various prescription and OTC diet pills abounding. With the possible exception of Viagra, virtually all these medicinal interventions designed to manipulation of normal bodily function has been debunked, at least among the more well informed public.
Historically speaking, the obstetrical profession has been having a romance with control that is now more than a hundred years long. Through the use of labor stimulating drugs, the amnesic and hallucinogenic drug scopolamine, frequently repeated injections of narcotics, anesthesia, and forceps, labor patients underwent surgical interventions such as episiotomies, instrumental deliveries and routine manual removal of the placenta. they have long desired to have total control over the physical act of childbirth.
The obstetrical profession has always seen itself as revolutionary and responsible for defining all aspects of pregnancy and birth care, including the politics of childbearing and our national maternity care policy. A historical example of this is a quote from the February 23, 1911 edition of the Boston Medical and Surgical Journal, page 261]
We believe it to be the duty and privilege of the medical profession of American to safeguard the health of the people; we believe it to be the duty and privilege of the obstetricians of our country to safeguard the mother and child in the dangers of childbirth. The obstetricians are the final authority to set the standard and lead the way to safety. They alone can properly educate the medical profession, the legislators and the public”
What we must first do is arouse public sentiment and first of all we must have the enthusiastic support and united action of the medical fraternity…. We feel that the most important change should be in the laws governing the registration of births. The word “midwife” as it occurs, should be at once erased from the statute books. … [Boston Medical and Surgical Journal, Feb. 23, 1911, page 261]
@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@
Links to scientifically-proven benefits of physiologically-based childbirth services and the risks of routine interventions, a list that begins by identifying the use of continuous EFM, Pitocin and epidural to all be medically unnecessary interventions that lead to preventable complication and substantial increase in operative delivery and Cesarean surgery.
University of Minnesota website; Center for Spirituality and Healing
What Factors Influence the Progression of Childbirth?
https://www.takingcharge.csh.umn.edu/what-factors-influence-progression-childbirth
Healthy Birth Practice #4: Avoid Interventions Unless They Are Medically Necessary
https://www.ncbi.nlm.nih.gov/pubmed/31118546
