
The Big Reveal ~ Motives hidden beneath the unfounded claims that more obstetrical interventions make childbirth safer for healthy childbearing women
This bring us back to the question I first started asking when I saw the drastic contrast between the non-interventive practices associated with childbirth of black mothers on 1 South, compared to “business as usual” obstetrical interventions used on white mothers admitted to 5 North.
Link to “Time Traveler’s Perspective on Normal Childbirth” published in journal BIRTH, September 2011
I was thunderstruck by their unwillingness or refusal to see what was right before their eyes — black mothers having perfectly normal births and healthy babies with virtually no medical or surgical interventions of any kind, while white mothers labored in semi-conscious drug fog and had births that included the routine use of episiotomy, dangerous fundal pressure, and forceps and babies born so respiratrially depressed the a significant number were never able to breathe. Why could these smart, well-educated men not see that the obstetrical protocols they impressed on white mothers were both unnecessary and harmful and just stop doing these things?
I have devoted decades of my time and talent to searching for these answers – more than 30 years of studying the motivations of the American obstetrical profession, both historically and in contemporary times, and making what I discovered publicly available on my various websites.
In addition to all the historical documents available on the Web, l am fortunate to live just a few miles from Stanford University, and its medical school library, which provide me with access to all variety of historical books and other publications. Many years of this in-depth research leaves me with the dubious distinction of having become an idiot savant in two areas. The first is a solid understanding of safe childbirth practices for healthy childbearing women and the second area is the harm caused by the dysfunctional obstetrical system in the US. Unlike the Western Europe,Obstetrics in America, long ago institutionalized the “wrong use” of obstetrical interventions as the legally-binding “standard of care” for obstetricians practicing in the United States.
Unfortunately, the information I uncovered was more disturbing that i could ever have imagined and included many issues — particularly the economics of hospitals and decades-long isolation and institutionalized abuse of laboring women — that shocked me speechless. The negative effects of our deeply dysfunctional obstetrical system is was even greater than the original issue I was trying to understand – why the American obstetrical profession treated two biologically-identical groups of healthy childbearing women in such a starkly different manner?
Early 1900s ~ peeling the onion, one layer at a time . . .
How the routine use of obstetrical interventions in the births of middle- and upper-class women in the early 1900s radical changed and redefined obstetrically-managed childbirth for the rest of the 20th and continues to dominate obstetrical practices in the 21st century
The disturbing and disheartening “answers” trace back to early 1900s. It was a “one-two punch” delivered by small number of extremely influential obstetricians over the decades from 1910 (the year Flexner Report was published) to the early 1930s. This elite guard of obstetricians was looking for ways to simultaneously eliminate the legal practice of midwifery the US, while also setting the policies and practice of obstetrics on a very specific trajectory — a hospital-based surgical specialty that ‘delivered’ healthy women who were unconscious under general anesthesia.
This “grand plan” directly eliminated decision-making by childbearing women in regard to what was done to them – in other words, they had absolutely no “say” about where and how they labored and gave birth.
The political version of this “grand plan” was to actively engage state legislatures to pass laws making the practice of midwifery. In many states, they succeeded in outlawing the care of professionally trained midwives who immigrated from the UK and Scandinavian countries, making it a crime for them to provide care during the normal biological event of labor and spontaneous birth.
The gender gap writ large, with women as mothers and midwives the historic losers!
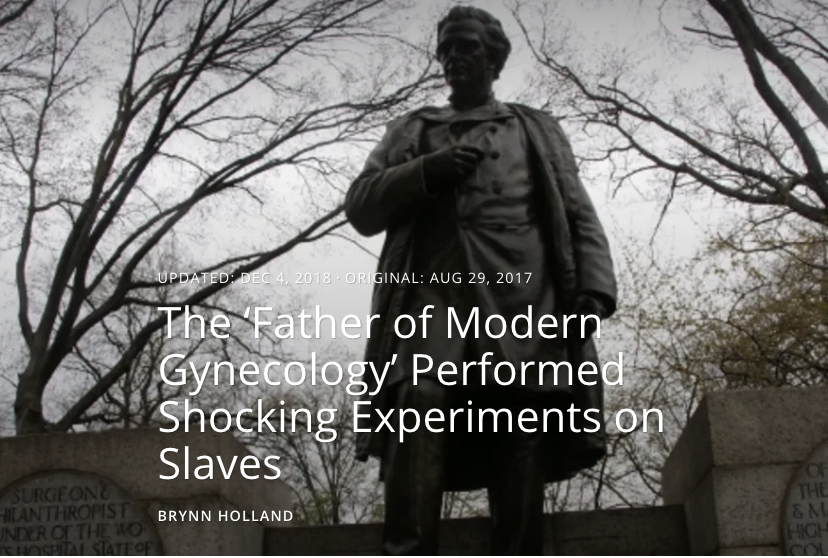
Statue of Dr. Marion Sims, the famous 19th century gynecological surgeon. Also owner of a Southern plantation & slave-holder, he perfected his surgical techniques by “practicing” his operations w/o anesthesia on 3 of his female slaves. The statute of this misogynist doctor was recently removed from Central Park in NYC
The gender gap writ large, with women as mothers and midwives the historic losers!
Unfortunately, this part of the story begins with the male of the species assuming that men naturally do everything better than members of the female gender.
For obstetricians in leadership roles in the early 20th century, the specific gender-related target was midwives.
What they characterized as the “midwife problem”, was the problem that doctors were having in eliminating midwives. Typical opinions about midwives remind me of the disparaging comments that upper-class whites have always made about the poor, uneducated, immigrants, and people of color.
In 1906 an obstetrician by the name of Dr. Gerwin described midwives as:
“ the typical … midwife, her mouth full of snuff, her fingers full of dirt and her brain full of arrogance and superstition”
A paper published 1907 by Drs. Emmons and Huntington criticized midwives for:
“the overconfidence of half-knowledge, …unprincipled and callous for the welfare of her patients”
Dr J. Whitridge Williams, 1912:
“The question in my mind is not “what shall we do with the midwife?” We are totally indifferent as to what will becomes of her…[1912-B, p.225]. No attempt should be made to establish school for midwives, since, in my opinion, they are to be endured in ever-decreasing numbers while substitutes are being created to displace them.” [1912-B; p.227]
Dr. Joseph DeLee’s 1915 publication “The Teaching of Obstetrics“; American Association of Obstetrics and Gynecologists
“The midwife has long been a drag on the progress of the science and art of obstetrics. Her existence stunts the one and degrades the other. For many centuries she perverted obstetrics from obtaining any standing at all among the science of medicine.
The midwife is a relic of barbarism. In civilized countries the midwife is wrong, has always been wrong. The greatest bar to human progress has been compromise, and the midwife demands a compromise between right and wrong. All admit that the midwife is wrong.
If the profession would realize that parturition [childbirth], viewed with modern eyes, is no longer a normal function, but that it has imposing pathologic dignity, the midwife would be impossible of mention.” [TASPIM, 1915 p.117]
[Transaction of the American Society for the Prevention of Infant mortality (TASPIM) 1915, p. 114]
The gender-loaded title of “Medical Men”
Most people don’t know that in the early 1900s, medical doctors in the US didn’t like being called “doctors”, which was more strongly associated with college professors and the ministerial title “Doctor of Divinity”, and they hated being referred to as a “man-midwife”. Instead they preferred being the descriptive title of “medical men”. A comment by no less an icon of obstetrical wisdom than Dr. J. Whitridge Williams demonstrates the nature of this gender issue:
“Have you ever considered,” he said, “the economical significance of the fact that three out of every five women are more or less incapacitated for several days each month, and that one of them is quite unable to attend to her duties?
Granting that the two sexes are possessed of equal intelligence, it means that women cannot expect to compete successfully with men. For until they are able to work under pressure for 30 days each month, they cannot expect the same compensation as the men who do so.” {Twilight Sleep: Simple Discoveries in Painless Childbirth; 1914}
During this formative period of American obstetric as distinct from its practice in other developed countries, the profession never doubted that Mother Nature, having blessed male MDs with the superior intellectual powers conferred by their “y” genes, meant it was their divine destiny to rescue the millions of white middle- and upper-class women who gave birth each year from a malicious Mother Nature.
American obstetricians believed it was both their right and their duty to be in charge of female reproduction, which meant that they controlled all aspects of pregnancy and childbirth in the United States.
“A Review of the Midwife Situation” ~ Boston Medical and Surgical Journal, 02-23-1911, page 261 {*} Arthur Brewster Emmons, 2d, M.D., Boston and James Lincoln Huntington, M.D., Boston.
“… we believe it to be the duty and privilege of the obstetricians of our country to safeguard the mother and child in the dangers of childbirth.
The obstetricians are the final authority to set the standard and lead the way to safety. They alone can properly educate the medical profession, the legislators and the public.”
While thes outspoken and politically-active obstetricians continued to assert that childbirth in the white well-off demographic of childbearing women was a dangerous abnormal state, they likewise insisted that reproductive biology of childbirth in women of color, immigrants and the working poor was relatively a normal.The sheer size of the average poor or immigrant families – as 15 or even 20 children – attested to that.
However, these same influential obstetricians insisted that normal labor and spontaneous childbirth in the upper classes of (white) women had somehow become a “patho-physiology”, that is, a dangerously dysfunctional aspect of female biology.
Very specifically, this was the opinion propagated by Dr. J. Whitridge Williams, former Chief of Obstetrics at the highly-guarded Johns Hopkins University Hospital and at the time, the Dean of it famous School of Medicine.
Having concluded that the lower classes of working poor did not particularly need, nor were able to pay for obstetrical services, the profession turned its attention to middle- and upper-class white women, whose families could afford an obstetrically-managed hospital birth. This serendipitously coincided with the more advent-guard ideas about making childbirth more “modern” by identifying obstetricians (i.e. not midwives) as the preferred birth attendant for the wealthier and whiter classes of women.
Articles by obstetricians published in newspapers and women’s magazines and broadcast on the radio, all described pregnancy and childbirth in the “modern” American (i.e. white) woman to as a “nine-month disease” that required a “surgical cure”. As spokesmen for the obstetrical profession, they were outspoken and relentless in promoting the idea of “always a doctor, never a midwife”.
Having defined normal childbirth to be pathology, professional services associated with the ‘disease’ of childbirth was, without question, the legal “property” of the obstetrical profession. Since ‘new’ obstetrics was defined as a surgical specialty, the proper way to refer to childbirth as attended by “medical men” was now referred to as “the delivery”, a term that defined childbirth to be a sterile surgical procedure conducted by an MD trained in obstetrical surgery.
This process began by putting labor patients to sleep with chloroform or ether and having the nurses cover the laboring woman with sterile drapes. Then the doctor stepped in to cut an episiotomy, instruct the nurse to provide “fundal pressure” (i.e. tp push very hard on the top of the mother’s uterus in order to press the baby’s head deeper in the pelvic) and then for the doctor to extract the baby with the use of obstetrical forceps.
After handing the newborn over to the L&D nurse, the doctor turned his attention to retrieving the placenta
By defining childbirth as a pathological process to be conducted under general anesthesia, the doctor removed the placenta manually (i.e. to use his hand) instead of waiting for it to be spontaneously expelled. In order to detach the placenta from the uterine wall and bring it out in his hand, the doctor he had to put on a special sterile glove with a long cuff that went up to his elbow. Then he inserted his hand and forearm into the mother’s vagina in order to reach inside her uterus and peel the placenta off the inner surface of the uterine wall, grab the separated placenta with his fingers, and draw it out of the uterus and the mother’s vagina.
The last of this series of surgical procedures was suturing the episiotomy incision.
Note that unconscious childbearing women could no longer described as “giving birth”; instead they were seen as passive entities from the doctor uses forceps to extract a baby from their unconscious bodies, thus establishing that it was the doctor, and not the mother, who “delivered” the baby.
For healthy childbearing women, this was the most profound change in childbirth practices in the history of the human species.
Continue to Chapter 3 ~ The Historical Role of Dr. J. Whitridge Williams, most famous obstetrician of the 20th century and author of “Williams’ Obstetrics”
