Chapter ? 3-b ? ~ The Historical Role of Dr. J. Whitridge Williams, most famous obstetrician of the 20th century and author of “Williams’ Obstetrics”
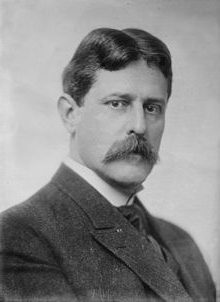
b. 1866 to d. 1931
Dr. J. Whitridge Williams was the most famous and highly-lauded American obstetrician of the 20th century. In addition to being highly influential within his profession peers and original author of “William’s Obstetrics (1904), he was also revered by other obstetricians and the general public.
He was by far the most outspoken, influential and prolific proponent of the “the new obstetrics” as a hospital-based surgical discipline.
It’s not surprising that historians also identify Dr. Williams as the founder of academic obstetrics in the United States and recognized him as the leader of obstetrics in America during the first 3 decades of the 20th century.
Personally, I would go much further; I would identify Dr. Williams as having almost single-handedly defined the discipline of obstetrics as a surgical specialty and promoted its “modern” practice as a highly interventive hospital-based process.
Dr. Williams also was acutely aware that the desperately needed a nationwide system of general hospitals like the famous large regional hospitals in Western Europe that were able to provide comprehensive and round-the-clock services to patients of ages and both genders. They were equipped with operating rooms and newer technologies such as x-ray machines that enable them to provide emergency care and medical, surgical, obstetrical, pediatric services to its hospitalized patients.
While the US had a very large number of hospitals — best historical estimate is 8,000 — they were overwhelmingly private, doctor-owned very small 2 to-10 bed hospitals that were more like convalescent home. They were neither staffed or equipped to provide emergency services or any but the very simplest of surgeries. Dr. J. Whitridge Williams believed that desperate need for a nationwide system of comprehensive general hospitals could be achieved over the next few decades via his a two-step “plan”.
@?move to stand-along post?@ {Click here to read the disturbing story}
His Plan is described in great detail in a 1914 book titled ~ “Twilight Sleep: Simple Discoveries in Painless Childbirth” written in collaboration with a famous science writer of the early 20th century by the name of Dr. Henry Smith Williams, MD, JD (no relation as far as we know). His goal was to invent a self-funding plan that would allow these hospitals to eventually transform themselves over a few decades into large general hospitals without having to borrow money from banks or take federal money that would expose them to long-term interference by the federal government.
Dr JWW’s Plan began by convincing the MD-owners of many of these small and middle-sized basically 19th-century hospitals to embark on a modernization plan for with the goal of bringing their facilities into the 20th century. This would include the physical remodeling and up of the hospital building and eventually purchasing technologically-sophisticated purchasing capital intensive equipment such x-ray machine, institutional autoclaves, microscopes, and other medical equipment, and putting in a new ceramic tiled operating rooms with state-of-the-art OR spot lights)
by using his very specific plan that would created a steady and dependable revenue stream that would provide the money for upgrading the physical hospital building and embark on a to fund of these
As a result of these often conflicting goals, his motives were a mixed bag.
As a professor of obstetrics at the prestigious Johns Hopkins University Hospital, he was very interest in increasing the number of “teaching cases” available for the clinical training of medical students. He believed that childbirth in the very lowest classes — new immigrants and black women — generally occurred naturally and without need of kind of obstetrical interventions. As a result, using this demographic of indigent labor patients was the perfect solution for providing medical students with clinical (or “hands-on”) experience. using the labors and birth among this poor and immigrant women as an endless source of “obstetrical material” (i.e. teaching cases).
he saw the in middle and upper-class whiteshould
that included giving repeated doses of Twilight Sleep drugs during labor, with or without patient’s consent. When the mother was ready to give birth, she was mover to an obstetrical operating room and rendered unconscious under general anesthesia (chloroform or ether). Then the OB or obstetrical resident cut a “generous” episiotomy and delivered the baby with forceps after asking the assisted by the nurse providing a forceful and dangerous form of “fundal pressure” (having the nurse push hard on the top of the mother’s uterus to force it farther down in the pelvis).
After extracing the baby with forceps, the doctor manually removed the placenta and sewing the mother’s vagina back together.
But before focusing on Dr JWW’s critical role in defining the “new obstetrics“, an overview of Dr. JWW’s professional background and positive contributions, which began with a vision for a nationwide system of large general hospitals like the system used in Western Europe for the previous two centuries.

The famous and grandiose Johns Hopkins Hospital, built in ?? 1890 ?? with an multi-million dollar endowment from (Google name)
Dr. Williams was employed by the famous and highly respected Johns Hopkins University Hospital for his entire professional life, from 1893 to his untimely and very painful death in 1931 after an operation to repair a diaphragmatic hernia was unsuccessful.
During professional career, he was a gynecological surgeon, a practicing obstetrician, a professor of obstetrics, and in 1899, appointed Chief of Obstetrics. His famous obstetrical textbook “Williams’ Obstetrics” was published in 1904 and is currently in its 27th printing. He was appointed Dean of Johns Hopkins University School of Medicine in 1911 and served in that role until 1923. After that he resumed his role as a professor of obstetrics for the medical school and personally editing the next 5 editions of his obstetrical textbook.
Without a doubt, Dr. Williams was committed to modernizing obstetrical education, elevating obstetrical practice, eliminating midwifery care, which he believed was dangerous, and improving the status of obstetrical medicine in the United States. As a member of the American Association for the Study and the Prevention of Infant Mortality” (AASPIM) a new national organization founded in 1909 [1] — Dr JWW was also committed to reducing the embarrassingly high rate of infant deaths in the US compared to other wealthy industrialized countries.
How allopathic medicine changed from a low-tech “healing art” to a modernized and technologically enhanced medical science early in the 20th century and resulting financial problem for small and medium-sized private hospitals
{A} As a medical doctor and Dean of a very prestigious medical school, Dr. JWW found himself living and working in one of the most extraordinary times in the history of medicine. Dr JWW and his contemporaries all played an important part in the most profound change in the practice of medicine in human history. For a variety of reasons, very few Americans know about this important period of history – the death of the pre-scientific “healing arts” and the ‘birth’ of modern medicine as a science-based, drug and technology enhanced, very expensive enterprise.
From Hippocrates to Heart Transplants ~ the birth of medical science
Medical science was preceded by 2,000 years during which the practice of medicine in Western cultures was known as “the healing arts”. These traditional healing methods started with the famous Greek physician, Hippocrates, (460 — 375 BCE) and his theory of “four humors”. The standard treatment for disease was based on “balancing” the four humors, which consisted of repeatedly bleeding patients until they lost consciousness and purging them with strong laxatives.
Over many centuries, more accurate knowledge of human anatomy and biology greatly improved the ability of doctors to diagnose and treat their patients. But without our modern diagnostics testing and effective drug therapies, the practice of medicine continued to primarily be an intuitive “art”. These thousands of years old practices defined medical care until the mid 19th century, when a rapid series of world-changing scientific discoveries in Europe and America gave us “modern medical science” and slowly displaced the “healing arts” over the course of the next century.
Medical science jumped into high-gear in 1850 with the use of ether by Dr. Morton, a Boston dentist, as the first relatively safe anesthesia. This was followed in the 1860s by Pasteur’s many important discoveries that resulted in the new science of bacteriology. Pasteur showed that microbes were omnipresent – in water, in air, on objects, and on the skin, and that a type of microbe called “bacteria” is what causes infectious diseases. Pasteur first published the finding of his study in 1861 and a 2nd paper on contagion and infectious diseases titled “The Germ Theory” in 1879.
In 1881 Pasteur delivered an address to a group of physicians at the Paris’ Institute of Medicine. Standing at a blackboard, he picked up a piece of chalk and drew a picture of what looked like railroad tanker cars lined up in a row. Then he turned to his audience and pointing to his rendition of the pathogenic bacteria streptococcus pyogenes said:
“This gentlemen is what causes puerperal sepsis and the death of newly-delivered mothers”.
Understanding that certain bacteria caused fermentation and disease allowed Pasteur to develop vaccines against anthrax and rabies. Prevention of disease though public sanitation systems and aseptic principles of personal cleanness, in combination with vaccinations and immunizations, continues to be a cornerstone of our science-based healthcare system.
{ref a ~ https://www.pasteur.fr/en/institut-pasteur/history}.
In 1865, Sir Joseph Lister, royal surgeon to Queen Victoria and “Father of modern surgery”, used the principles set out in Pasteur’s bacteriological science to develop antiseptic medicine and sterile surgical technique. The principles asepsis and sterility continue to be one of the pillars of modern medical practice.
In 1895, the discovery of radiation led to the manufacture of the first x-rays machines. This was quickly followed by blood-typing in 1901 and the first pharmaceutical drug in 1909. At this point, the practice of medicine had become a modern science, one that would change the lives of millions of people for the better.
However, the scientific advances in late 19th and early 20th century were not restricted to diseases and their treatments. This particularly fertile period included the invention of electric lights, telephones, the x-ray machine (1895), aspirin and understanding blood types (1901), first manned plane flight (1903), Model T Ford (1908), the Hoover vacuum cleaner, an early version of an automatic dishwasher, and in 1909, the first pharmaceutical drug to treat African sleeping sickness.
The great “leap forward” even more important than landing on the moon
For the very first time in human history, the combining of scientific knowledge with technical abilities and human ingenuity allowed medical doctors to consistently cure formerly fatal diseases and successfully treat injuries that used to be deadly. All of this stands on the shoulders of the dedicated physician-scientists who brought the “miracles of modern science” into being in the late 19th and early 20th century.
Over the next century, medical science expanded exponentially to included antibiotic drugs, chemotherapy, organ transplants, reattachment of limps, laser surgery to restore sight, DNA-designed drugs and genetic engineering.
This change also dramatically impacted hospitals who suddenly had to figure out how to bring the scientific practice of medicine to their hospital without breaking the bank. The best guess by historians is that US had about 8,000 small, doctor-owned 2 to 10 bed hospitals in the early 1900s. Relative to the modern practice of medical science, these small private hospitals they were still on 19th century time.
The last gasps of 19th century hospitals as they were dragged into the 20th century
Prior to the scientific era, the basic function of hospitals was providing “hospitality”, that is, a medicalized version of a well-staffed hotel that provided clean dry linens, three meals a day, and help to the bathroom or a bedside commode.
Basic nursing function were done by non-professionals (often members of a religious order) who provided nursing care to bed-ridden patients, bathing them, changing bandages, emptying bedpans, and feeding patients too ill to feed themselves.
This category of “palliative care” was typically provided to patients with chronic or terminal diseases or recovering from a debilitating injury. No matter how sick these patients were, scientific medical treatments such as IVs, blood transfusions or chemotherapy drugs were not a possibility.
But as the healing “arts” morphed into a very modern medical science during the first three decades of the 20th century, the nature of hospitals in America changed dramatically. Among the many “gifts” produced by medical science was a tsunami of must-have medical equipment, specialized supplies and eventually various medical technologies.
Hospitals of any size that wanted to be “modern” had to figure out how to afford the purchase of capital-intensive equipment like x-ray machines and other new and usually expensive medical equipment.
Over the course of a few decades, many these small 2-to-10 bed hospitals that provided palliative and “end of life” care morphed into vibrant institutions in which the idea of “medical science” had become an active verb. This gave rise to many different forms of effective medical and surgical treatments, which meant the majority of its seriously ill or injured patients not only lived, but they walk out of the hospital on their own two feet!
But who is going to pay the big bill that medical science runs up? If one were to ask the American Medical Association, the answer would certainly been “the patient” and not under any circumstances (i.e over our dead bodies!) would it be the state or federal governement!
Note-2-self ~Economics from the hospital’s perspective (i.e. NOT pts as paying customers) Further more, I think the following rendition is redundant and should be melded together into a single topic
For all of their lifesaving and world-changing properties, these scientific discoveries and new technologies had a substantial economics downside for hospitals. As already noted, modern medical miracles don’t come cheap. This was particularly a problem for the 8,000 small, private, doctor-owned hospitals that suddenly found themselves in a time warp that relegated them to the Dark Ages! It was like they’d been were doing a brisk business in horse-and buggy transportation, only to wake up one day and see the streets filled with cars! What to do?
This brings us back to Dr. JWW and his vision. As mention to earlier, he saw two different but intertwined problems. The first had to do with those 8,000 small privately-owned hospitals that were now out-of-step with the times and desperately needed to be modernized and brought up to 20th century standards. This of course meant the purchase of capital-intensive medical equipment and upgrading or remodeling their physical facilities.
Keep in mind that these hospitals were all “for-profit” businesses that depended on sick patients as paying customers to keep the door open and pay the of the staff, with enough profit left over for the doctors that owned it believe the effort worthwhile to keep it open.
But unless they found a way to increase their revenue – more patients, longer hospitalizations, maybe a generous endowment from grateful philanthropist — these small hospitals would forever remain stuck in 19th century “healing arts” as providers of palliative treatments to the chronically and terminally ill.
Continue to Ch 3 ~ Two problems, one solution, a big win for society at the expense of healthy childbearing women
