word count 3715 Jan 17, 2025
Chapter Eight ~ 2001 – 2004: The Surgical Fix
 At the beginning of the 21st millennium, a small but influential group of obstetricians began to openly question the biology of vaginal birth. This wasn’t the first time that an obstetrician had questioned the basic character of the female reproductive capacity. In the early 1900s Dr DeLee insisted that childbirth, from the standpoint mother’s perineum, was “about as “natural” as falling on a pitchfork“.
At the beginning of the 21st millennium, a small but influential group of obstetricians began to openly question the biology of vaginal birth. This wasn’t the first time that an obstetrician had questioned the basic character of the female reproductive capacity. In the early 1900s Dr DeLee insisted that childbirth, from the standpoint mother’s perineum, was “about as “natural” as falling on a pitchfork“.
He likewise insisted that every baby’s head was subjected to pathological forces during even the most normal labor by being repeated bashed into what he described as “the mother’s iron i.e. intact perineum. He thought that only the generous use of episiotomy could save mother and baby from the defects of female biology. He also believed that the birth canal was so intrinsically dangerous that the routine use of forceps were necessary to save the baby from being battered and brain damaged as it was pushed along by unpredictable and malevolent forces of nature.
Prophylactic Cesarean Section at Term
The theme begun by Dr DeLee early in the 20th century reoccurred again in the last decades of the century. In a peer-reviewed paper published in the New England Journal of Medicine in 1985, a case was made for the mother’s right to have a Cesarean “on demand” (the precursor to ‘patient-choice’ CS), as well as a move to “prophylactic” Cesarean as a preemptive strike to protect the baby from the “dangers” normal labor and birth.
The authors, Doctors Feldman and Friedman, were suggesting that from the standpoint of fetal wellbeing, the obstetrical standard of care should become a 100% scheduled Cesarean. This drastic idea would redirect the professional focus of obstetricians from the management of labor and birth to the prenatal determination of fetal lung maturity so that the CS could be scheduled before the mother went into spontaneous labor and (Gasp!) ‘”accidently” gave birth naturally!
This recommendation was based on the idea that routine use of cesarean surgeries would entailed only a minor amount of “excess” or “extra maternal mortality”, which was trivial when compared to the loss fetal and newborn life associated with normal birth. The Doctors Feldman and Friedman opined that the “low cost of excess maternal mortality” may be a price worth paying.
Here is a short excerpt:
“….the number of extra women dying as a result of a complete shift to prophylactic cesarean section at term would be 5.3 per 100,000…. This may be the proper moment to recall that the number of fetuses expected to suffer a disaster after reaching lung maturity is between 1 in 50 to 1 in 500. … if it could save even a fraction of the babies at risk, these calculations would seem to raise the possibility that a shift toward prophylactic cesarean section at term might save a substantial number of potentially healthy infants at a relatively low cost of excess maternal mortality.” p. 1266
“We probably would not vary our procedures if the cost of saving the baby’s life were the loss of the mother’s. But what if it were a question of 2 babies saved per mother lost, or 5 or 10 or (as our calculations roughly suggest) as many as 36 or 360? …. Is there some ratio of fetal gain to maternal loss that would unequivocally justify a wider application of this procedure?
….is it tenable for us to continue to fail to inform patients explicitly of the very real risks associated with the passive anticipation of vaginal delivery after fetal lung maturity has been reached? If a patient considers the procedure and decides against it, must she then be required to sign a consent form for the attempted vaginal delivery?” p. 1267 [Prophylactic Cesarean Section at Term? Feldman & Feldman; NEJM, May 1985]
As at the beginning of the 20th century, so at the end of the 20th century, the conclusion of the obstetrical profession was that normal vaginal birth is risky and damages both mothers and babies .
From 1910 to 1980, the obstetricaltione solution – only now the fix is ‘elective’ Cesarean instead of routine use of episiotomy and forceps. Since the late 1970s, the list of reasons for doing Cesarean deliveries had steadily lengthened and the number of surgeries increased from an average of 5% in 1975 to approximately 27% in 2003.
Cesarean Surgery as a Replacement for Normal Birth, claimed by obstetricians to be as safe as vaginal birth for childbearing women and safer for babies.
The question about the safety of vaginal birth, the strong sentiment within the obstetrical community lead many in the obstetrical community reiterate the idea of Drs. Feldmen and Friedman about ‘Cesarean on demand’, that is, women electing to have a Cesarean even if there were no immediate medical reasons for surgery.
In 2000 Dr Ben Harer, former president of the American College of Obstetricians and Gynecologists (ACOG), was interviewed by Diane Sawyer on Good Morning America. Dr Ben Harer supports the idea that Cesarean surgery is safer and better than vaginal birth. Here are excerpts from the transcript of the show:
Diane Sawyer: “Each year, one in every five babies in America comes into the world through a cesarean section, the country’s most common surgery. “
Diane: “Some obstetricians are now calling the cesarean section preferable to vaginal births.”
Diane Sawyer: “ . . . (doctors) believe that women should at the very least have the option to choose between the two . . . . and that insurance companies should basically pay … equally and treat them equally.”
Dr. Harer: “…Yes …. women should be given the facts and then given the choice.”
Diane: “…and (you say) there’s a higher rate of problems with vaginal birth, than with cesarean section. . .”
Dr. Harer: Yes, for the baby, the risks are far higher for vaginal delivery . . .
than for an elective cesarean section at term. For the mother, the immediate risks for a cesarean section are a little higher ….
Dr. Harer: but the longer term, risks of pelvic dysfunction, incontinence . . . . . . those risks are higher for vaginal birth. Over the long term I think that the risks balance out, that there really is no big difference” (between surgery & normal birth).
Questions, Questions, Always More Questions…
The unanswered question at this point is simple – could he and the other be right? How could a century of obstetrical opinion be wrong? Is it normal childbirth or medical management that is the origin of these problems? Is Cesarean surgery basically benign, at least as compared to the ‘dangers’ of normal vaginal birth? How enthusiastically should we embrace this wave of the future – elective Cesarean as the 21st century standard of care?
The background question is whether or not modern day obstetrical management of healthy women with normal pregnancies is a science-based system, a value-added service with a “superior” tract-record that rightly displaces physiological management. The pinnacle of this system, the final solution recommended by Dr Harer and others in the obstetrical profession, is the most surgical of all ‘surgical’ procedures.
It is offered as a permanent replacement for vaginal birth predicated on the idea that normal birth is defective beyond repair and needlessly damages birth mothers and babies. The obstetrical ‘proof’ for this opinion is the failure of the profession’s best efforts for the last 100 years to make birth safe, a state of affairs that leads obstetricians to conclude that its got to be the physical body of childbearing women that is at fault.
That century of “best effort” was focused on the idea of obstetric surveillance of pregnancy and then using specially trained hospital staff and specialized equipment of the maternity wards to evaluate, diagnose, prevent and treat problems. In the last 30 years that has meant the use of EFM, which is now the standard of care.
The medical profession and the lay public have both assumed that this general process in combination with this specific equipment and the skills of obstetricians to recognize abnormal EFM strips and perform and appropriate and “timely” Cesarean surgery, could and would vouch safe the baby from brain damage and cerebral palsy.
This sincere belief lead to the conclusion that it was worth the loss of all other aspects of normal birth — physiological, psychological, social and developmental — as well as the huge expense of total medicalization, so as to permanently eliminate this ancient scourge.
And when not even the best of obstetrical management could buy the much sought after safety and reliably guarantee a perfect baby, the official recommendation by obstetricians was to scrap normal birth all together and identify elective Cesarean as the safest way for a baby to “delivered”.
But what if this was based on a faulty premise, what if the data was wrong? Wouldn’t that call the conclusion into question also?
To address that question, ’m going to focus first on the hot-button issue of EFM. Then we’ll return to:
- the general questions of obstetrical surveillance of pregnancy
- management of labor by a specially trained staff and specialized equipment of the hospital
- the experience of the laboring women in the year 2005,
- the issue of vaginal by-pass surgery — Cesarean section — valid reasons to recommend or perform a CS and the immediate, delayed and downstream consequences of its use.
The EFM – CP Connection ~ Cure? Cause? Or Inconsequential?
 In July 2003 a well-respected report by none other than the American College of Obstetrics and Gynecologists quietly revealed that the most sacred dogma of obstetrical practice incorrect. ACOG’s Task Force on Neonatal Encephalopathy & Cerebral Palsy concluded that the obstetrical profession was mistaken about the ability of continuous electronic monitoring and liberal use of cesarean section to reduce the rate of cerebral palsy and other neurological disabilities.
In July 2003 a well-respected report by none other than the American College of Obstetrics and Gynecologists quietly revealed that the most sacred dogma of obstetrical practice incorrect. ACOG’s Task Force on Neonatal Encephalopathy & Cerebral Palsy concluded that the obstetrical profession was mistaken about the ability of continuous electronic monitoring and liberal use of cesarean section to reduce the rate of cerebral palsy and other neurological disabilities.
Editor’s Note –> * “neonatal encephalopathy” is med-speak for birth-related brain damage]
The ACOG Task Force went on to identify the failure of EFM and cesareans to prevent these complications, stating that:
“Since the advent of fetal heart rate monitoring, there has been no change in the incidence of cerebral palsy.
…. The majority of newborn brain injury does not occur during labor and delivery. Instead, most instances of neonatal encephalopathy and cerebral palsy are attributed to events that occur prior to the onset of labor.”
This ACOG task force report had the endorsement and support of six major federal agencies and professional organizations, including the Center for Disease Control & Prevention (CDC), the March of Dimes and the obstetrical professions in Australia, New Zealand and Canada. It is described as the “most extensive peer-reviewed document on the subject published to date.”
An August 15, 2002 report in Ob.Gyn.News stated that:
…performing cesarean section for abnormal fetal heart rate pattern in an effort to prevent cerebral palsy is likely to cause as least as many bad outcomes as it prevents.”
…. A physician would have to perform 500 C-sections* for multiple late decelerations or reduced beat-to-beat variability to prevent a single case of cerebral palsy. [** ‘numbers needed to treat’] emphasis added
The September 15, 2003 edition of Ob.Gyn.News stated that:
The increasing cesarean delivery rate that occurred in conjunction with fetal monitoring has not been shown to be associated with any reduction in the CP rate…
… Only 0.19% of all those in the study had a non-reassuring fetal heart rate pattern…. If used for identifying CP risk, a non-reassuring heart rate pattern would have had a 99.8% false positive rate….” [emphasis added]
 Most people incorrectly assume that EFM is the equivalent of an electrocardiogram (EKG) for the unborn baby but this is a serious misunderstanding of the technology as used for the last 30 year. Electronic monitoring equipment simply provides an elaborate mechanism to count the unborn baby’s pulse.
Most people incorrectly assume that EFM is the equivalent of an electrocardiogram (EKG) for the unborn baby but this is a serious misunderstanding of the technology as used for the last 30 year. Electronic monitoring equipment simply provides an elaborate mechanism to count the unborn baby’s pulse.
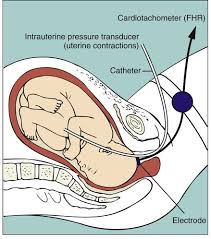 The machine transposes the acoustic signal of the baby’s heart rate into a printed paper graph and video display.
The machine transposes the acoustic signal of the baby’s heart rate into a printed paper graph and video display.
This permits the educated observer to evaluate a graphic representation of the four auditory markers of fetal well-being – baseline heart rate (110 to 160), variability (should be present 90% of time), accelerations (should be intermittently present) and decelerations (brief decels can sometimes be OK but generally should not be present).
Over the course of the 20th century medical science had developed a more sophisticated understanding of FHT patterns, especially in regard to variations and deviations from the normal baseline and their relationship to uterine contractions. It is interesting to note that this method of beat-by-beat auscultation in relationship to uterine activity was the theoretical underpinnings that eventually lead to the development of electronic fetal monitoring.
 But the original theory and method of fetal surveillance comes from the work of Dr. Joseph DeLee. In his 1924 obstetrical textbook, he described counting fetal heart tones during a uterine contraction in twelve, 5-second sampling and then transposing these numbers on to a graphic representation of the uterine contraction. [Principles and Practice of Obstetrics; DeLee, 4th edition, ch. 8, p. 144].
But the original theory and method of fetal surveillance comes from the work of Dr. Joseph DeLee. In his 1924 obstetrical textbook, he described counting fetal heart tones during a uterine contraction in twelve, 5-second sampling and then transposing these numbers on to a graphic representation of the uterine contraction. [Principles and Practice of Obstetrics; DeLee, 4th edition, ch. 8, p. 144].

Midwives, physicians and labor room nurses have been listening to fetal heart tone for most of the 20th century, so obviously continuous EFM is not the only way to track the wellbeing of the fetus in labor. However, the way this information was collected in decades past did not usually integrate all four markers of fetal wellbeing, making this an inadequate tool for protecting fetal wellbeing. During the last 20 years a method has emerged to collect the same type of information electronically gathered by EFM, but without the expense or restrictions of this equipment. This equally effective alternative method is called “intermittent auscultation” or (IA) and it is able to detect the baseline rate, heart rate variability, accelerations (if present) and pathological decelerations (if present).
Intermittent auscultation describes a process to gather that same information by listening regularly to fetal heart tones with a fetoscope or an electronic Doppler for one full minute immediately following a uterine contraction and counting in twelve (or more) 5-second samplings to determine the baseline rate.
IA also detects the presence of a normal heart rate, normal variability, presence of normal accelerations and absence of pathological decelerations. In the presence of a reassuring pattern such as described above, the likelihood of hypoxic states (i.e., fetal distress) occurring within the next 120 minutes of normal labor is statistically insignificant. [“Fetal Monitoring In Practice” by Dr David Gibbs & S. Arulkumaran, MD; published in the UK]
While IA is more time-intensive (requiring a professional at the bedside), it is equally as effective as continuous EFM for low and moderate-risk labors, with the added benefit of a greatly reduced cesarean rate (4% vs. 26%). This is, in part, because it unhooks healthy mothers from machines and permits laboring women to move around freely.
No longer tethered to the bed by electronic wires, the mother is able to change positions frequently, walk, use hot showers or deep water for pain relief and make “right use of gravity” IA is harmonious with physiological process, which reduces fetal distress and failure to progress and the need for Pitocin-augmentation of labor, pain medication, anesthesia and instrumental and operative delivery.
In spite of the significant benefits of intermittent auscultation, the obstetrical profession generally dismisses the use of IA for what they claim is the “unacceptably great expense involved in providing the one-on-one nursing that is almost mandatory to perform intermittent fetal heart rate auscultation.” [Obstetrics: normal and problem pregnancies, Gabbe et al; 1992, p. 457]. This is a strange objection, since many hospitals bill, and insurance companies reimburse, $400 an hour for the use of continuous EFM, far less than the average L&D nurse’s hourly salary.
The Bible of Science Based Birth Care
The next question on our list is the efficacy (safety + cost-effectiveness) of the system of obstetrical management for a healthy population of childbearing women. If obstetrical management is to replace physiological forms of maternity care, we should be certain the replacement system is scientifically sound one that uses evidence-based practices.
For an objective determination on this issue There are two excellent, well-respected sources that we may turn to. The first is a scientifically researched publication known as ‘A Guide to Effective Care in Pregnancy and Childbirth’ and the second is a survey of contemporary maternity care practices entitled “Listening To Mothers”, commissioned by the Maternity care Association of New York City and conducted by Harris Poll Interactive in 2002.
To determine the scientific aspect of current obstetrical practices we’ll first look to the published work of Drs Ian Chalmers and Murray Enkins and their life-long work — the bible of evidenced-based maternity care — entitled ‘A Guide to Effective Care in Pregnancy and Childbirth’ (GEC). It is a compilation of all pregnancy and childbirth related studies published in the English language in the last 30 years.
The Guide to Effective Care identifies six levels effectiveness/efficacy, ranging from the positive end of ‘clearly beneficial’ (category 1) to the negative end (category 6) of ‘likely to be ineffective or harmful’. Using the preponderance of available evidence, Drs Chalmers and Enkins rated each ‘standard’ maternity-care practice and regularly used medical/ surgical interventions for safety and efficacy. Based on these categories, the G E C cautions that:
“Practices that limit a woman’s autonomy, freedom of choice and access to her baby should be used only if there is clear evidence that they do more good than harm”
“Practices that interfere with the natural process of pregnancy and childbirth should only be used if there is clear evidence that they do more good that harm”
As measured by the six categories identified in the Guide to Effective Care, the “standard of care” presently as provided by obstetricians is extremely discordant when measured by scientific principles (both in practice and in interpretation of scientific studies) and evidence-based practice parameters.
Contemporary obstetrics reverses the recommended safe practices, with those identified as most beneficial and least likely to cause harm (List #1) being the last or least used and those identified as most likely to be ineffective or harmful (List #6) being the primary or routinely used methods. This vastly increases the number of medical and surgical interventions used and the complications occurring, both immediately and downstream.
Maternity Center Association Report “Listening to Mothers
Information on the childbearing woman’s experience of childbirth and the care she received is strangely missing from most obstetrical sources. For that information we turn to the October 2002 report by the Maternity Center Association “Listening to Mothers: Report of the First National US Survey of Women’s Childbearing Experiences” conducted by the Harris Interactive Polling Service.
The Maternity Center Association (MCA) of New York City, is a non-profit organization established in 1918. It promotes safer maternity care and develops educational materials for expectant parents on ‘evidenced-based’ maternity practices — that is, policies that are based on a scientific assessment of the safety and effectiveness of commonly-used methods and procedures.
The MCA commissioned a survey of healthy mothers with normal pregnancies (no premature babies, multiple gestations, breech or sick mothers) who gave birth in the last 24 months to track contemporary obstetrical trends and the quality of care received by healthy childbearing women. The full report (some 60 pages long) is available on the Internet at www.maternitywise.com.
MCA Study Concludes ~ There is no ‘normal’ birth in American Hospitals
According to the “Listening to Mothers” survey, 99% of healthy pregnant women do not receive science-based maternity care from their obstetrical providers. The average healthy mom was exposed to 7 or more significant medical interventions and/or surgical procedures during a ‘normal’ labor and birth.
The document notes that in the previous 24 months (Oct 2000 to Oct 2002) there were virtually NO ‘natural’ births occurring in hospitals. The entire hospitalized population of healthy mothers-to-be were subjected to one or more major interventions. The only women who had a normal birth without medical or surgical interventions were those who had their babies at home or an independent birth center.
It also documented a significant gap between scientific evidence and standard obstetrical practice. Healthy, low-risk women in the United States often receive maternity care that is not consistent with the best research and in fact, is often directly in opposition to scientific recommendations. According the MCA, many people are not aware of the following major areas of concern:
- The under-use of certain practices that are safe and effective
- The widespread use of certain practices that are ineffective or harmful
- The widespread use of certain practices that have both benefits and risks without enough awareness and consideration of the risks
- The widespread use of certain practices that have not been adequately evaluated for safety and effectiveness
According the ‘Listening to Mothers’ survey, the majority of childbearing women did not receive the safer and more satisfactory type of care delineated in the top 3 categories (those established as beneficial) and instead were exposed to a plethora of practices in the bottom 3 categories which were rated as of unknown or unproven effectiveness, unlikely to be effective or known to be harmful. The survey documented the following statistics are for healthy women at term with normal pregnancies. Intervention rates would be higher for women medical complications.
93% Continuous electronic fetal monitoring;
86% IV fluids and denial of oral food and water
74% Immobilized or confined to bed due to physician preference,
hospital protocols or the limitations imposed by multiple medical devices
(EFM, IVs, epidural catheter, Foley bladder catheter, etc)
71% Push and deliver with mother lying flat on her back
67% Artificial rupture of membranes
63% Epidural anesthesia
63% Pitocin induced or accelerated uterine contractions
58% Gloved hand inserted up into the uterus after the delivery
to check for placenta or remove blood clots
52% Bladder catheter
35% Episiotomy
24% Cesarean delivery (12.6% planned/12.4% in labor
11% Operative – one-half forceps, half vacuum extraction
In a population that was essentially healthy (95% +/-), an astounding 55% of women had some form of surgery performed – episiotomy, forceps, vacuum extraction or Cesarean section. Using the classical definition of operative delivery (CS+ forceps/vacuum extraction) the rate for 2002 would be 38% or 2 out of 5. This is twice the operative deliveries reported by physicians in the early 1900s who merely performed operative procedures on 1 out of 5. Intervention rates would be much higher for women with premature labor, multiple pregnancies or frank medical complications.
The Listening to Mothers survey is consistent with data from the CDC’s (Center for Disease Control) National Center for Health Statistics Vol. 47, No 27, on The Use of Obstetric Interventions 1989-97. It documents a steady annual increase since 1989 in each of these interventions.
A press release dated June 6, 2002 based on the NCHS report “Births: Preliminary Data for 2001” [NVSR Vol. 50, No. 10. 20 pp] for the year 2001 documents a 24.4% CS rate (the same rate as identified by the Listening to Mothers survey). Statistics for the year 2003 show an even higher Cesarean rate – 26.1 in the US and 26.8 in California. http://www.cdc.gov/nchs/releases/02news/birthlow.htm)
As a result of the Listening to Mothers survey, the Maternity Center Association’s recommended:
“ ..more physiological and less procedure-intensive care during labor and normal birth”.
****************************************
Link to Chapter Nine
