 Conservative, Responsible, Humane, Woman-centered and Cost-effective Maternity Care in 21st-Century America
Conservative, Responsible, Humane, Woman-centered and Cost-effective Maternity Care in 21st-Century America
Part One ~ The $64,000 dollar questions are:
“Where did it go?”
&
“How can we get it back?”
I am not old enough to remember what it was like when physiological care for a normal childbirth was the norm and was typically provided all over the country by experienced midwives.
However, I am old enough to have been a very young student nurse in the mid-1960s, when normal labor and birth in our hospital was primarily provided by general practice doctors.
The management style of these GPs was conservative, as defined by the classical principles of conservation of well-being. In regard to childbirth, the ability of these practitioners to successfully manage a vaginal birth was also valued by the other doctors in the community. Cesarean section was still widely (and rightly) seen as a potentially dangerous procedure, thus something to be used sparingly and then only when all else had failed.
Even complications such as a marginal placenta previa were managed “conservatively”, with the professional skill of the practitioner informally judged by his ability to avoid a Cesarean.
 Except for emergency C-sections, all intrapartum Cesareans required the physician to get a second opinion. The doctor providing that 2nd opinion as to whether or not a Cesarean surgery was warranted also could not belong the same group practice as the physician who thought a surgical delivery Cesarean was necessary.
Except for emergency C-sections, all intrapartum Cesareans required the physician to get a second opinion. The doctor providing that 2nd opinion as to whether or not a Cesarean surgery was warranted also could not belong the same group practice as the physician who thought a surgical delivery Cesarean was necessary.
In addition to the “second opinion” rule, each Cesarean was reviewed by the obstetrical department’s morbidity and mortality (M&M) committee, which met monthly. Any physician whose C-section rate was substantially above average was interviewed to find out why surgical rate was so much higher than average.
If there was no apparent medical reason for the higher rate, he was warned that he would be put on probation for as long as his C-section rate remained disproportionately high. If probation became necessary, a proctor physician would be assigned to help him bring his C-section rate into line with the overall norms for the hospital. In 1961, our teaching hospital had a 3% Cesarean section rate.
The Good ‘ole days when midwives and general practice physicians had a pretty good “working relationship”

General practice physician performing a newborn exam on hour-old baby“
Most of these general practice physicians were older, having graduated from medical school in the late 1930s and early 1940s, when half of all births still occurred at in the parents’ home under the watchful eyes of one or more experienced midwives.
Doctors from that generation often agreed to provide “back-up” for midwives. This meant they could call on him if a mother or baby developed complications that required his medical services or hospital transfer.
GPs also hired midwives to monitor a labor patient at home and then assist him during the birth. During the immediate postpartum period the midwife stayed for several hours after the baby was birth. This included caring for newly-delivered mother, helping her breastfeed for the first time. and making sure her newborn was warm and doing well. Then the midwife arranged to do daily home visits for the next 10 days to check on the nursing mother and baby.

Midwife Ina May Gaskin (The Farm in Tennessee) listing to the fetal heart rate with an acoustic fetoscope called as “Pinard Horn”
Unfortunately, the era of childbirth services by midwives and general practitioner MDs began to ebb away early in the 1940s, first very slowly and then faster and faster.
By the end of the 1960s, childbirth services by midwives and general practice physicians were nothing more than a nostalgic memory, as newly minted obstetricians greedily dream of the day when all childbirth-related care would be in the hands of obstetricians and they alone would have the legal authority to “deliver babies”.
*************************************
Yet another $64,000 question — Planned obsolescence by the obstetrical profession for the all aspects of conservative and responsible maternity care, and why no one asked questions or tried to stop it?
After I graduated from nursing school and got hired to work nights in the L&D unit, GPs were still attending the majority of births. The smaller number of obstetricians on staff only attended about a quarter of all births, and these were often doctors’ wives, socialites, and very wealthy and/or politically influential patients.
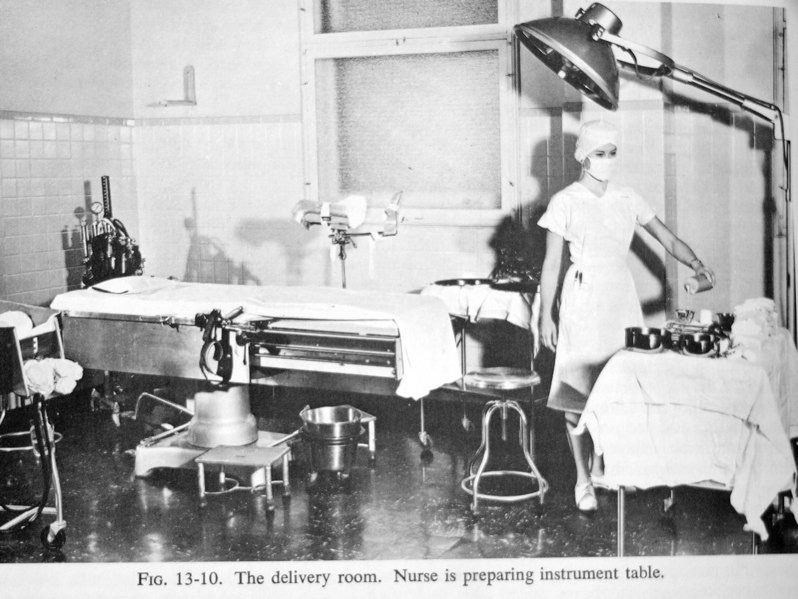
Exact replica of the OR-style “delivery rooms” and the white scrub dresses that the nurses wore our our hospital (OMH) in the 1960s
But during the first ten years of my L&D nursing career, I noted the incremental elimination of GPs from the roster of physicians that had obstetrical privileges.
During the 1960s, the scale was tipping slowly toward obstetricians, as the number of older GPs who were well-known and well-liked finally dwindled to zero.
The reason was the dominating influence of obstetrician members of ACOG who exerted near total control over the hospital policies for the obstetrics department.
By the 1980s all our GPs had disappeared off the face of the earth, but there still were a few newly minted “family practice” physicians were attending births. However, our obstetricians saw this as a challenge to “go for broke” and get rid of all the “competiton” once and for all!
After eliminating the obstetrical privileges of GPs, the next target for their obstetrical wrath was to reduce the scope of practice of family practice doctors, which resulted in increasingly restrictive policies for non-obstetrician physicians. Even though these family practice MDs were fully licensed as ‘physicians and surgeons’, they were no longer permitted to attend breech or twin births or perform Cesareans.

The hospital’s chief of obstetrics, who was responsible for all OB department policies, was elected by physicians with obstetrical privileges at our hospital.
As ACOG members, obstetricians dominated the staff and pretty much got what they wanted. This included dirty dealing by a few head-strong obstetricians who “did not play well with others” and instead spent all their energy defending their obstetrical “turf”.
Having strategically eliminated all other categories of physician-providers of childbirth-related services, all the obstetricians on staff insisted that only board-certified obstetricians had the appropriate training and skill to deliver a baby, which would mean that only obstetricians should be allowed to deliver babies in our hospital, and successfully arm-twisted the hospital administrator to agree.
For all their years of medical school and years of residency in obstetrics, our obstetricians and their medical students didn’t understand anything about the biology of spontaneous and other such niceties. Quite obviously the obstetrical profession didn’t believe in the “right use of gravity“, and were convinced that God surely wouldn’t have given us forceps if Mother Nature was not such a bitch!
How the American obstetrician profession was able in 1910 to convinced a majority of American women (and husbands who paid the bill) that white middle and upper-class homo-sapiens females were only able to give birth safely when they were “delivered” by a doctor in a hospital
The facts speak quite eloquently for themselves and the obstetrical profession in the United States was listening carefully. Obviously, there was no money to be made by obstetricians when all the young healthy women in the neighborhood just “popped” their babies out, no fuss, no muss. These were identified by obstetricians as the really “bad old days”, when childbearing women were being helped by midwives and GPs.

5,000 year-old Egyptian hieroglyphics of normal childbirth
In the early 20th century (1910 to be exact), after many thousands of years in which the biology of normal childbirth was generally successful, influential leaders of the American obstetrical profession decided to “nip such such foolishness in the bud” — up with that we cannot put!
Not only were the “normal births” fast and straight forwards (described in Genesis as “they were lively upon the birth stool”) but also extremely bad for obstetrical profession, and also deprived hospitals of the steady revenue stream from its maternity ward that was much appreciated.
Hospital administrators were able to use income generated by maternity patients to make up for deficits in other departments. It also allowed them to make “capital-intensive” purchases, such as x-ray machines and putting in surgical suite that sported a big electric spotlight in the new operating room. Being able to upgrade and modernize their facilities was a proven way for the hospital to attract more paying customers, and the economic benefits that the hospital’s higher daily “patient census” generated.
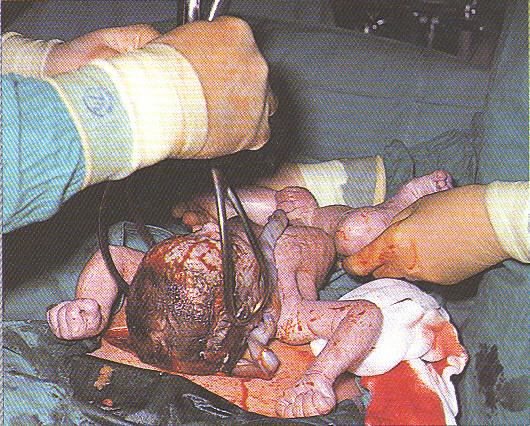
The obvious result ii this hospital-centric obstetrical system that it was so successful in turning normal childbirth in a perfectly healthy women into patients of a surgical speciality, and reconfiguring spontaneous childbirth into a series of surgical procedures performed under general anesthesia and described as “the delivery”.
“Delivery”
something now done by the doctor
and not by unconscious childbearing women
Compared to fooling around with women whose babies just “popped” out (often before the doctor arrived), the new ideas generated by the obstetrical profession for monetizing maternity care made childbirth into a money-making bonanza beyond their wildest dreams!
You could charge a lot of money for services that began with a “painless childbirth” easily achieved by administrating Twilight Sleep drugs to all labor patients. Then there were all the billable procedures associated with “delivery” as a surgical procedure — a charge for general anesthesia, another for “performing” an episiotomy, a charge for the surgical procedure of “forceps delivery, another for removing the placenta from the mother’s uterus and last but not least, the charge for suturing the OB’s patient perineal incision.
This was of particular to the future of the woman’s sex life after having a baby. In particular, the issue was the level of satisfaction experienced by her husband. Obstetrician never want to have yet another husband come to you and complain that “ever since my wife had the baby, having sex with her is just like walking into a warm room” and expecting you to “make it right again” (i.e. turn her back into a virgin).
But good news, the gravy train didn’t stop there! When it came to hospital profits as generated by the “baby business” during the first several decades of the 20th century, hospital-based childbirth also included the traditional 14-day lying-in period in the hospital maternity ward. Hospital room rates for new mothers were was low as $2.45 and high as $11 and hospital’s newborn nursery charged from $3 to $8 for her infant.
How historical era of American obstetrics from 1910 to the 1960s first defined and ultimately changed my life forever
My personal story begins when I was a student nurse rotating through our hospital’s racially segregated all-black ward in the basement. It was my good luck, and a true privilege for which i am eternal grateful, to find out personally and up-close just how the spontaneous biology of normal childbirth actually worked (very well, thank you!).
Without realizing it, our black labor patients on 1South were directly benefited by the hospital’s policy of “benign neglect” generated by its racial segregation. Black patients in labor were lift to their own devices during first stage labor — undrugged, uninterfered with, able to walk around, drink, and sit on the toilet when they began to feel “pushy”.
All together, this was a perfect form non-interventive labor “management” in which the mother who managed herself just fine! When birth of the baby began approaching, hospital policy called for one of the nurses to move the laboring woman by stretcher to the elevator in the rear of the hospitsl (only a few feet from the door to 1South, the hospital’s industrial kitchen and laundry and morgue) to the white delivery room on 5-North. As i have already described, it was my great pleasure to see a lot of nice healthy babies born to very happy new mothers in that elevator, long before got it got to the 5th floor.
This experience was both educationally important and emotionally rewarding on its own merits. But far more important, it made me very smart in regard to spontaneous childbirth, and what I describe as “rough, and tough, and very very (impossible!) to bluff when came to clearly dysfunctional profession of obstetrics as practice in American hospitals.
This became such a deep aspect of my personally that it also (unfortunatley) lead to my being arrested and jailed in 1991 for the sin/crime of attending the normal births of healthy women in their own home. I was living in and attending home births in the state of California before our Legislature finally passed the Licensed Midwifery Practice Act of 1993. But that is a digression so let me return to the ……
what childbirth at as worked as L&D nurse on the night shift at Organge Memorial Hospital in Orlando Florida from 1961 to 1963. I learned a great deal about many aspect of life, not only the biology of normal childbearing, but also the centruies-old mysoginy on steriods and the political machinations of “organized medicine” (documented as far back as 1820!) fo the obstetrical profession who has been adding more and more intervertion (interruptiions and interference of the delicate phycioloty of childbearing)
Later its historic name of OMH on Orange Avenue for more than a century recently changed to Orlando Regional Hospital.
The newly-naned ORH is just four shot block from the Pulse Night Club. On that tragic night — June 12th, 2016 — the over 60 critically wounded and dead inundated ORH’s ER. As a former ER nurse myself, i was so glad not to have been working there that night.
does not need and actually is harmed by virtually all of the “business as usual” obstetrical interventions and routinely conducting a so-called “normal” vaginal childbirth as surgical procedure to be “perfomed” the doctor.
You read that right! In my world of circa 1961 to 1964 childbearing women did NOT “give birth” as a spontaneous biological event.
Instead our about-to-be new mothers lay unconscious under general anesthesia, laying flat on their back, both legs in obstetrical stirrups, both feet in the air, as one of our obstetricians, interns, resident or medical students cut a “generous” episiotomy in preparation for a routin forceps delivery, which was believed to save the baby’s head from becoming “a battering ram thurst repeately against its mother’s “iron perineum” and damage equated by the obstetrical profess to be equal to having “fallen on a pitchfork”.
inserted each blade of the forces separately into the mother’s uterus at each side of the unborn baby’s head, locked the handle together and pulled on the baby while, as circulating L&D nurse, stood on a foot stool at the mid-side of the laboring woman, placed my right forare tight againd ghe very top of her uterus as i grabbed my hand grabed the far side of the delivery tatel and thing balled up by lest hand and pushed it against my right are in “T” configuration and leaninforward so the whoel weight of my own body was balanced over the unconscious mother’s body, was instructed to push down (“give it all you’ve got”) as he (all our doctors and medical students were male) as he pull on the handles of the stainelss-steel obstetrical forceps with all his might.
Sometimes these babies, who already the narcotis given to it mother running aourn in its own veins,
Nothing about the 20th and 21st-century obstetrical systems had anything to do with helping healthy women to have a normal spontaneous birth with no unnecessary medicalization.
That is when I ask to be transferred to the ER, where i personally was every so much happier but it did nothing to fix oue extremely dysfunctional obstetrical system. More about that later!
 Business-as-usual obstetrics was much petter for doctors than for healthy childbearing women
Business-as-usual obstetrics was much petter for doctors than for healthy childbearing women
For more than a century, “business-as-usual” for the American obstetrical profession has always been organized around putting the laboring woman in bed and medicating her with various kinds of drugs to speed up the labor and potent narcotics to kill the pain.
For over a hundred years, normal childbirth has been conducted as a surgical procedure that was literally and legally “performed” by the doctor on an anesthetized labor patient. Obstetrical “delivery” began by cutting a “generous” episiotomy, extracting the baby from its mother’s inert body with forceps, reaching a gloved hand up into the mother’s uterus and peeling the placenta off the uterine wall and pulling it out and suturing the episiotomy incision.
This was the most profound change in childbirth services in the history of the human species. Whether this was done by one of our very nice GPs, a family-practice physician, or an obstetrician, I knew full well that it was not only medically unnecessary but it made normal childbirth unnaturally dangerous and painful.
Childbirth in Black and White prior to the passage of the 1965 Civil Right Act

This is the story of my time as a student nurse in the “Deep South” in the 1960s, and the following four years. During that time our racially-segregated hospital had two very different systems for providing maternity care that all depended on whether the labor patient was white or black,
The historical story of the two very different systems for providing maternity care in our racially segregated hospital in the Deep South of the 1960s. Which place you wound up depended on whether the labor patient was white or black, during my time a student nurse and following four years
I first learned about normal childbirth as a student nurse during my rotations in the segregated black ward (One South) in the basement of our hospital. Since there was no “labor ward”, black mothers in labor were admitted to their postpartum bed.
Unlike white mothers, black labor patients were never given anything “for pain”. However, they were sternly instructed to immediately notify the nurse when they “needed to push”. Then a floor nurse, and me as a student nurse, would get the labor patient on a stretcher and head for the elevator in a usually unsuccessful attempt to get the patient up the hospital’s one of the hospital’s two “delivery rooms” on 5North.
Alas, most of these mothers had already given birth several times. More than half the time, their babies made a sudden and unscheduled appearance in the elevator before we reached 5North. What was so striking to me was that something so extraordinary as giving birth could happen so easily, quickly and with with no discernible no fuss.
Laying on the stretcher and covered with a hospital sheet as the elevator rose slowly, the mother ever-so-slightly held her breath and made a tiny little grunting noise. The RN instantly flip the elevator switch off so the doors wouldn’t open to gaggle of strangers. Then the nurse turned around and pulled the sheet back, revealing the very top of the baby’s head as it begin to peak out of its mother’s vagina.
In the next 60 seconds, the baby’s head slowly spun out of the mother’s body, and the rest of its body slipped out, landing between its mother’s legs. Then the new mom, cool as you please, reached down between and picked up her newly born baby, and cuddled him or her tight in her arms as God’s newest member of the homo-sapiens species took its first breath and began cooing.
Wow, did I really see what I just saw, or was I dreaming?
 One a dozen thoughts this triggered was the obvious biological fact of spontaneous childbirth that is hiding in plain sight — giving birth as Mother Nature configured female reproductive biology is something that the childbearing woman herself does!
One a dozen thoughts this triggered was the obvious biological fact of spontaneous childbirth that is hiding in plain sight — giving birth as Mother Nature configured female reproductive biology is something that the childbearing woman herself does!
But the obstetrical system that keeps new mothers from realizing that they themselves did the hard work of giving birth! Somehow our new mothers always thought they should be grateful to the doctor for having “delivered” the baby. Over and over again I saw new mothers thanking their doctor profusely and squeezing his hand in gratitude for “delivering her baby”.
I also remembered those thousands of medical interventions that kept the nursing staff, nurse-anesthetists, and all the doctors, busy but also allowed them to take credit for having “delivered” the baby as an obstetrical procedure, and then would send the parents a substantial bill for his “delivery” services.
From an honest and accurate economic perspective, it was duplicitous for the obstetrical profession to bill for hundreds or thousands of dollars for attending a spontaneous birth, when the real work was being done by the about-to-be new mother!
 But what was so amazing to me as a student nurse was the contrast between the white labor patients upstairs that I saw obstetrically “delivered” on 5North. These women were under the influence of Twilight Sleep drug scopolamine.
But what was so amazing to me as a student nurse was the contrast between the white labor patients upstairs that I saw obstetrically “delivered” on 5North. These women were under the influence of Twilight Sleep drug scopolamine.
This psychotropic drug often caused our labor patients to try to climb over the bed rails and try to escape! Surely this was not a pleasant experience for our white labor patients.
When their babies were about to be born they were taken by stretcher to the delivery room, moved to the operating room “delivery table”, strap their arms to the side of the delivery table so they touch (and contaminate) any of the sterile instruments, strap their legs into metal obstetrical stirrups to make the forceps deliver easier, and then “knock’em out” under general anesthesia. Now the stage was all set for the doctor to step between the stirrups that held her legs in the air and cut an episiotomy, and use of forceps to pull the unborn baby out of its unconscious mother’s body.
There is a very old-fashioned term about people “covering their eyes with wool” and its opposite — “removing the wool from their eyes”.
I finally “removed the wool from and eyes” in 1976 and immediately quit my job as a hospital L&D nurse, never to return, and eventually to cross-train in traditional (out-of-hospital) midwifery. I became a professionally licensed midwife in 1997 (number 041) and have never regretted any of those decisions. As I write this in 2025, I am now retired, which gives me lots of time to write and reminisce.
However, the story of those bad old days still needs to be told, so we better understand how and why normal childbirth in the United States got hijacked by the obstetrical profession in 1910 and has held childbearing women and midwives hostage every since.
Obstetrics before “malpractice madness” made everyone crazy
As a labor room nurse in the early 1960s, both GPs and obstetricians delivered breeches and twins vaginally, with little or no ‘special’ attention or preparation. Both of these situations were considered a variation of normal vaginal birth and the outcomes for these mothers and babies were consistent with those of other normal vaginal births.
 However, this was before the “one-two punch” that changed the practice of medicine in America forever!
However, this was before the “one-two punch” that changed the practice of medicine in America forever!
The ‘punch’ was a fateful decision by the United States Supreme Court (1964?) who ruled that all MDs, irrespective of what part of the country they practiced in, were legally held to the same basic and universal “medical standard of care” (more later).
Then in 1976, the medical profession was again turned upside down by the infamous “malpractice crisis of 1976“. The problem was the audacity of the medical malpractice insurance industry to raise its rates (a lot!) and in particular, the rates for doctors in Southern California. One cannot help but assume that wealthy movie stars and their expensive ‘no-holds-barred’ attorneys sued their doctors each and every time their newest face-life was not to their liking.
Of course, these same doctor were not going to take this laying down. Theoretically under a blood-red banner that read:
“Up With This We Will Not Put!”

… all the doctors in Southern California banded together and staged a real-life “doctors’ strike” that lasted almost a month or so. Sometime later, when state mortality statistics for that period became available, newspapers and nightly TV news reported a precipitous FALL in the mortality rate while doctors were refusing to doctor and surgeons were refusing to put up a scalpel and incise!
As expected, older (and usually wiser) doctors of that era insisted that the practice of medicine would never be the same again and apparently they were right!
Deconstructing Conservative and Responsible Maternity Care for fun and profit!
After I graduated from nursing school and got hired to work nights in the L&D unit, GPs were still attending the majority of births. The smaller number of obstetricians on staff only attended about a quarter of all births, and these were often doctors’ wives, socialites, and very wealthy and/or politically influential patients.
But during the first ten years of my L&D nursing career, I noted the incremental elimination of GPs from the roster of physicians who had obstetrical privileges. During the 1960s, the scale was tipping slowly toward obstetricians, as the number of older GPs who were well-known and well-liked finally dwindled to zero. The reason was the dominating influence of obstetrician members of ACOG to exert control over the hospital policies for the obstetrics department. By the 1980s the GPs were all long gone, but a few newly minted “family practice” physicians were still attending births.
Having already eliminated the obstetrical privileges of GPs, the next target for the obstetrician wrath was restricting the scope of practice of family practice doctors. This resulted in increasingly restrictive policies for these non-obstetrician physicians. Even though these family practice MDs were fully licensed as ‘physicians and surgeons’, they were no longer permitted to attend breech or twin births or perform Cesareans.
The hospital’s chief of OB, who was responsible for all the OB department policies, was elected by a vote of physicians with obstetrical privileges. As ACOG members, obstetricians dominated the staff and pretty much got what they wanted. This included dirty dealing by a few head-strong obstetricians who “did not play well with others” and instead spent all their energy defending their obstetrical “turf”.
Having strategically eliminated all other categories of physician-providers of childbirth-related services, all the obstetricians on staff insisted that only board-certified obstetricians had the appropriate training and skill to deliver a baby, which would mean that only obstetricians should be allowed to deliver babies in our hospital.
All the obstetricians on staff got together and arm-twisted the Administrator into only allowing board-certified obstetricians to provide obstetrical services. This was when the use of forceps suddenly became much more frequent.
Even more important, it was when I consciously realized that I could no longer be an “accomplice” to what were some versions of an “organized crime family” — well-meaning, but still dysfunctional and fundamentally wrong. Nothing about the 20th and 21st-century obstetrical systems had anything to do with helping healthy women have a normal spontaneous birth with no unnecessary medicalization.
“Business-as-usual obstetrics” was good for obstetricians but bad for childbearing women
 For more than a century, “business-as-usual” for the American obstetrical profession has been organized around putting the laboring woman in a hospital bed, medicating her with various kinds of drugs to speed up the labor, and injected with potent narcotics to kill the pain. When they started to push, they’d be moved to an obstetrical operating room where the “delivery” or “baby-ectomy” would be performed. When the general anesthesia wore off, these new mothers, according to the obstetrical professions, were supposed to be eternally grateful to the doctor for “delivering their baby” and then being paid a goodly fee for the inadequate and harmful care they received.
For more than a century, “business-as-usual” for the American obstetrical profession has been organized around putting the laboring woman in a hospital bed, medicating her with various kinds of drugs to speed up the labor, and injected with potent narcotics to kill the pain. When they started to push, they’d be moved to an obstetrical operating room where the “delivery” or “baby-ectomy” would be performed. When the general anesthesia wore off, these new mothers, according to the obstetrical professions, were supposed to be eternally grateful to the doctor for “delivering their baby” and then being paid a goodly fee for the inadequate and harmful care they received.
For over a hundred years, normal childbirth has been conducted as a surgical procedure that was literally and legally “performed” by the doctor on an anesthetized (thus unconscious) labor patient. Obstetrical “delivery” began by cutting a “generous” episiotomy, extracting the baby from its mother’s inert body with forceps, reaching a gloved hand up into the mother’s uterus and peeling the placenta off the uterine wall and pulling it out and suturing the episiotomy incision.
This was the most profound change in childbirth services in the history of the human species, bar none!
Whether this was done by one of our very nice GPs, a family-practice physician, or an obstetrician, I knew full well that it was not only medically unnecessary but it made normal childbirth unnaturally dangerous and painful.
Childbirth in Black and White 1960s prior to passage of the 1965 Civil Right Act
The historical story of the two very different systems for providing maternity care in our racially segregated hospital in the Deep South of the 1960s, all depending on whether the labor patient was white or black, during my time a student nurse and following four years
I first learned about normal childbirth as a student nurse during my rotations in the segregated black ward (One South) in the basement of our hospital. Since there was no “labor ward”, black mothers in labor were admitted to their postpartum bed.
Unlike white mothers, black labor patients were never given anything “for pain”. However, they were sternly instructed to immediately notify the nurse when they “needed to push”. Then a floor nurse, and me as a student nurse, would get the labor patient on a stretcher and head for the elevator in a usually unsuccessful attempt to get the patient up the hospital’s one of the hospital’s two “delivery rooms” on 5North.
 Alas, most of these mothers had already given birth more than once so their babies made a sudden and unscheduled appearance in the elevator before it ever reached 5North. But what was so striking to me was that something so extraordinary as giving birth could happen easily and quickly with no discernable fuss!
Alas, most of these mothers had already given birth more than once so their babies made a sudden and unscheduled appearance in the elevator before it ever reached 5North. But what was so striking to me was that something so extraordinary as giving birth could happen easily and quickly with no discernable fuss!
Laying on the stretcher and covered with a hospital sheet, the mother ever-so-slightly held her breath and made a tiny little grunting noise. The RN instantly responded by flipping off the elevator switch so it wouldn’t open to gaggle of on-lookers. Then the nurse turned around and pulled back the sheet and we could see the very top of the baby’s head beginning to peak out of the mother’s vagina.
In the next 60 seconds, the baby’s head spun out of the mother’s body, and the rest of its body slipped out and landed between its mother’s legs. Then the new mom, cool as you please, reached down between her legs and picked up her newly born baby, and cuddled him or her tight in her arms, as God’s newest creation took its first breath and began to coo.
Wow, did I really see what I just saw, or was I dreaming?
With a dozen thoughts racing around in my head, this experience made the biological fact of spontaneous childbirth very plain, even though it was hiding in plain sight — giving birth as Mother Nature configured our female reproductive biology is something that the childbearing woman herself does!
But we have a strange system in which the new mother doesn’t realize that she was the one who did the hard work of giving birth and instead believes she should be grateful to the doctor for having “delivered” her baby! Is this nuts or what? But it was the norm for new mothers to thank their doctors profusely, over and over again, for “delivering” (i.e. catching) the baby as the mother pushed it out.
I also remembered those thousands of medical interventions that were critical activities for the nursing staff, the nurse-anesthetists, and all the doctors, who would take credit for having “delivered” the baby as an obstetrical procedure but would send the parents a substantial bill for his “delivery” services.

Note the presence of midwife Donna Driscoll on right side of the photo
From an economic perspective, it would be hard for the obstetrical profession to justify a bill for hundreds or thousands of dollars for attending an actual “natural” birth in which the real work is that which is done by the about-to-be new mother.
But what was so amazing to me as a student nurse was the contrast between the white labor patients upstairs that I saw obstetrically “delivered” on 5North. These women were under the influence of Twilight Sleep drug scopolamine. T his psychotropic drug often caused our labor patients to try to climb over the bed rails and try to escape! Surely this was not a pleasant experience for our white labor patients.
When their babies were about to be born they were taken by stretcher to the delivery room, moved to the operating room “delivery table”, strap their arms to the side of the delivery table so they touch (and contaminate) any of the sterile instruments, strap their legs into metal obstetrical stirrups to make the forceps deliver easier, and then “knock’em out” under general anesthesia. Now the stage was all set for the doctor to step between the stirrups that held her legs in the air and cut an episiotomy, and use of forceps to pull the unborn baby out of its unconscious mother’s body.
There is a very old-fashioned term about people “covering their eyes with wool” and its opposite — “removing the wool from their eyes”.
I finally “removed the wool from and eyes” in 1976 and immediately quit my job as a hospital L&D nurse, never to return, and eventually to cross-train in traditional (out-of-hospital) midwifery. I became a professionally licensed midwife in 1997 (number 041) and have never regretted any of those decisions. As I write this in 2025, I am now retired, which gives me lots of time to write and reminisce.
However, the story of those bad old days still needs to be told, so we better understand how and why normal childbirth in the United States got hijacked by the obstetrical profession in 1910 and has held childbearing women and midwives hostage ever since.
@@@@@@@ ??? end here, ???? begin new essay below?
1910 to 1993 ~ Behind-the-scenes “dirty politics” by influential obstetricians with the goal of totally eliminating the practice of midwifery in the United States & erase all public memory of the non-interventive care provided by midwives as guardians of normal childbirth
There has been an aggressive, century-long sustained agenda by influential members of the obstetrical profession to reduce the number of non-obstetrician providers of childbirth services to zero if they possibly could.
Midwives were their very first target, and I must admit, they succeeded beyond their wildest dreams. With considerable political and financial help of the AMA (see ref below) a small but very committed cotillion of politically-aggressive obstetricians with a lot of resources launched a public-relations campaign to permanently abolish midwifery in the United States.
{Transactions of the American Association for the Study and Prevention of Infant Mortality (national conferences met annually from 1910 to 1923-?-25),
They used the political resources provided by the AMA to help eliminate the practice of midwives all across the country. Their strategy was simple — pass to types of laws that by themselves and together defined its practice to be an illegal practice of medicine. Some of these laws defined attending a birth by anyone who was not an MD to be an illegal act. Other lawys unless restrice made attending a birth by into a crimiinal act for which the midwives could be arrested and jailed.
but just jailing midwives was not enough. The also had to demean, denigrate, ridicule, insutlt (see posted list of references with links to original publications, esp this link –>
{ https://ca-lm.org/hx-and-contmpry-comments-physicians-abt-midwives-mar2016/ }
and specifically erase the memory of midwifery care from the American public. and put out even the tiniest shred of respect for the care provided by midwives, virtually erasing everything about midwifery or the care provided by midwives from the brains of virtually every American between 191o, and at least in the state of California, the passage of the Licensed Midwifery Practice Act of 1913. As a California Licensed MIdwifery (licence 041) I’m am pboth proud and happy. But really wish the price of our victory in the California Legislature had not been so personal.
The return of Conservative and Responsible Maternity Care
Aside from the ethical principle of autonomy of healthy and mentally competent adults is the disturbing issue of an obstetrical profession that is apparently being held hostage to a radical form of maternity care for healthy women, which seeks to make surgical birth a ‘standard of care’ for the obstetrical profession. Due to policies set by hospital obstetrical and anesthesia departments, obstetricians are being restricted to a level of obstetrical care well below that of first-year obstetrical residents.
Obstetricians now need a permission slip from the hospital administration or chief of the anesthesiology department in order to provide care for a planned VBAC. In many case, obstetricians are forbidden, through formal or informal OB department policies, to provide vaginal birth services to mothers with twin or breech pregnancy. (This also applies to providing backup services to midwives or accepting hospital transfer of home birth clients.)
The result of a disenfranchised obstetrical profession is a sky-rocketing C-section rate, which in my professional life (1961 to the present) has gone from 3 to 27 percent. Identified risks of cesarean includes 33 well-known complications (including a 13-fold increase in emergency hysterectomies) compared to only 4 specific risks for normal vaginal birth –> see MCA’s systemic review at www.maternityWise,org].
“What every pregnant woman needs to know about Cesarean Section”
Childbearing women who are delivered by Cesarean section are two to four times more likely to die from the intra-operative, post-operative or downstream complications of Cesarean surgery than from normal vaginal birth.
More than a dozen operative and post-op complications for the mother are associated with Cesarean including maternal death, maternal brain damage, anesthetic accidents, drug reactions, infection, accidental surgical injury, hemorrhage, emergency hysterectomy, blood clots in the lungs, need to be admitted to ICU, need to be on life support, inability to breastfeed.
Potentially-lethal complications and protracted difficulties extend into the postpartum period, post-cesarean reproduction, post-cesarean pregnancies and post-cesarean labors. Reproduction complications include secondary infertility, miscarriage and tubal pregnancy.
Delayed or downstream complications in future pregnancies include placental abruption, placenta previa, placenta percreta, uterine rupture, and maternal death or permanent neurologically impairment.
Risks to babies include accidental premature delivery, surgical injury during the C-section, respiratory distress, increased rates of admission to NICU. Risks to babies in subsequent pregnancies include placenta abruption/stillbirth, death or permanent neurological disability (do to uterine rupture), lung disease and increased rates of both childhood and adult asthma.
For this reason, the reduction in operative deliveries associated with physiological management is an important tool in the reduction of maternal mortality and perinatal loss in future pregnancies.
A large number of women with identified pregnancy risks such as VBAC or breech baby at present are totally unable to get appropriate obstetrical care. Some of these women are choosing instead to be cared for by midwives and other are choosing unattended home births.
These parental choices may address the family’s own personal dilemma, but it doesn’t address the underlying problem. The major social problem here is a disenfranchised obstetrical profession – doctors forbidden to do doctoring — and the run-away costs, both personal and economic that are occurring subsequently.
This prevents the United Staes from having a truly conservative and responsible maternity care system, which is also a handicap in a global economy, preventing the US from being competitive around the world.
The solution lies in three specific areas of reform. One is the need for tort law reform in combination with ACOG policy statements and position papers that recognize physiological management as an appropriate category of care provided by obstetricians to healthy women with normal pregnancies, in which the mother neither desires or requires interventionist obstetrical care.
The second is for medical educators to acknowledge that physiological management is the foremost standard for healthy women worldwide. This would permit them to learn the principles of physiology themselves and subsequently to teach physiological management to medical students and in obstetrical residency programs, with the expectation that physiological principles would be routinely utilized for healthy women.
And last but not least is the staffing of labor and delivery units of hospitals by professional midwives as practitioners who are authorized to provide the full spectrum of physiological care to healthy women.
On the continuum of physiological management, the ‘birth’ or ‘delivery’ is not a separate activity requiring the services of a surgical specialist, but rather a normal part of normal maternity care as provided by the hospital-based midwife. At the request of either the mother or the obstetrician, the physician may be called to ‘catch’ the baby, but it would not be required by hospital policy.
Part and parcel to this changed relationship with hospital-based midwifery is also the ‘normalizing’ or rehabilitating of relationships with community-based midwifery, so that complementary professional relationships can develop between community midwives and hospital obstetricians. This would lead to the integration of community midwives into the health care system and result in “relocated home births” for that category of women with significant risk factors that can be reduced by early and easy access to medical services.
