https://tinyurl.com/y8udohl6
 Since the 1914 publication of Dr. J. Whitridge Williams’ little 128-page book {click here for original source material: “Twilight Sleep: Simple Discoveries in Painless Childbirth”}, the “behind the scenes” information it reveals about the history and impact of obstetrics in the United States is, politically and ethically-speaking, the equivalent of the Pentagon Papers, in that it shows us what was hidden and why.
Since the 1914 publication of Dr. J. Whitridge Williams’ little 128-page book {click here for original source material: “Twilight Sleep: Simple Discoveries in Painless Childbirth”}, the “behind the scenes” information it reveals about the history and impact of obstetrics in the United States is, politically and ethically-speaking, the equivalent of the Pentagon Papers, in that it shows us what was hidden and why.
Like the Pentagon Papers, this little book is also the story of powerful people in ‘high places’ who wanted us to believe a set of alternative facts that were never true.
A hundred years later, this book clearly identifies — in excruciating detail — the undeclared motives and hidden agenda of the obstetrical profession. It finally answers, also in great detail, questions of great importance to healthy childbearing women.
- How and why were healthy childbearing women turned into the patients of a hospital-based surgical specialty?
- How and why did normal birth become a surgical procedure performed on an anesthetized mother-to-be by an obstetrically-trained surgeon?

I recently saw the movie “The Post” and remember a remarkably shocking quote from the Pentagon Papers. To paraphrase, it was an admission that our use of military force in Vietnam was only 10% necessary, 20% prophylactic (to prevent future attacks) while being 70% CYA: To keep government officials under five different presidents from having to publicly admit that they were wrong.

Vietnam War ~ 4 soldiers carrying a fallen comrade
They knew their strategy was a failure, and that the war was unwinnable, that it was killing young American soldiers by the boatload (50,000 over 11 years), but they just couldn’t stop pretending they were doing the right thing for the right reasons: It would be too embarrassing to admit (a) they were wrong and (b) that they’d lied about it for decades.
Vietnam War & the American obstetrical profession’s Hundred Years War on normal childbirth — the exact same legacy of duplicity
Seen from the perspective of Dr. JWW’s little book, the surgical specialty of obstetrics as the official “standard of care” for healthy childbearing women is the same sort of story. Like the Pentagon Papers, Twilight Sleep: Simple Discoveries in Painless Childbirth also shows why influential obstetricians, who had multiple private agendas and professional goals, needed the American public to believe a set of alternative facts that were never true.
As with America’s involvement in Vietnam, Dr. Williams “Plan” also seemed like a really good idea in 1914 for the apparently compelling reasons he identified in his little book.
Dr. JWW’s ‘plan’ was adopted and widely implemented without ever having been “vetted”, that is, subjected to scientific studies that matched cohorts of healthy childbearing women whose normal births were managed in two dramatically different ways — the time-tested model of supportive physiologic management in homes and small private ‘lying-in’ hospitals vs. the brand new idea of hospital-based obstetrics as a surgical speciality — and then compared outcome statistics (number of deaths and serious complications) for both mothers and their babies in each of the two groups.
Under Dr. JWW’s watch as chief of obstetrics and Dean of the School of Medicine at Johns Hopkins during the first two decades of the 20th century, hospital-based obstetrics for healthy women with normal pregnancies and no complications routinely included protocols that drastically interfered with the normally progressive biology of childbirth (ex. semi-conscious women laying flat in bed after repeated doses of narcotics). After that, a long list of obstetrical interventions including general anesthesia and surgical procedures were substituted for what otherwise would have been a normal spontaneous process in these healthy women.
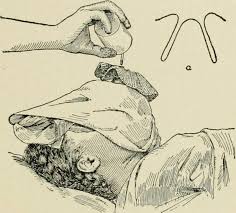
Administration of ‘drip’ ether to an obstetrical patient
During the 21 years, Dr. JWW was directly involved in the surgical specialties of obstetrics and gynecology (1893-1914), hospital-based obstetrics developed a universal model that considered laboring women to actually be surgical patients. That was the origin of shaving off the mother’s pubic hair (the OB ‘prep’) on admission to the labor ward and administering a large soapsuds enema. These are same protocols normally used to prep patients for abdominal surgery.
This obstetrical model routinely included the use powerful narcotics and the amnesic and hallucinogenic drug scopolamine during labor, as well as other medical interventions and invasive procedures. When the baby was about to be born, the mother was moved to a sterile operating room and rendered unconscious under general anesthesia. Then the new surgical procedure of ‘delivery’ was performed by a doctor trained in obstetrical surgery. This ‘baby-ectomy’ included the use of obstetrical stirrups, episiotomy, forceps, manual removal of the placenta and stitching up the perineal incision.
The good news for Dr. Williams and other obstetrical doctors of his day is that they DIDN’T do any comparison studies, as the morbidity (serious complications) mortality rate for both mothers and babies was over the moon when compared to watch monitoring of normal labor and birth by trained midwives and country doctors.

Early 1900s photo of a labor patient in obstetrical stirrups
But since Dr. Williams had no data to prove otherwise, his “plan” to normalize the obstetrically interventive as the model of care for normal childbirth took off like a rocket. Like a snowball rolling downhill that left a path of thousand dollar bills in its wake, the money, the professional and social prestige, the personal control, — everything about the obstetrical system as a monopoly on normal childbirth services was just too darned good to give up!
To admit that a model of a massive intervention in normal childbirth was intensely harmful (even fatal) as well as painful, humiliating, expensive was also unnecessary, would be to shoot oneself in the foot. One’s professional life and income as an obstetrician in America would never be the same again.
What is so different for American obstetrics, as compared to most other developed countries, is that routine maternity care to essentially healthy childbearing women is provided by professional midwives and general practitioners MDs (now known as ‘family practice’ physicians). This represents 70-80% of “the baby business”.
Women with pre-existing medical conditions (heart or kidney disease, etc), high-risk pregnancies (placenta previa, multiple gestations, pre-term labor, etc) or develop complications (toxemia, HHELP syndrome, etc) are referred to obstetricians. Obviously, this is only 20-30% of the baby business. American obstetricians did the math and concluded that 100% sound a lot better than a mere 25-30%.
Unfortunately, what this means is that the American obstetrical profession stubbornly refuses to look at the numbers — the excess mortality that historically resulted from Dr. JWW’s plan — and that fact that obstetrically managing healthy childbearing women as ‘surgical patients’ is still to unnecessarily introduce potentially-deadly, always harmful and expensive iatrogenic and nosocomial complications that are detrimental to the individual laboring woman, her baby, her family and society as a whole.
Just like in the 20th-century, 21st-century American obstetrics is never having to admit that you were wrong, never saying your sorry, and never ever agreeing to change your behavior so these things don’t happen in the future.
Part 2-B of this post will be devoted to the vital but missing 20th-century statistics (they existed, but Dr. Williams et al either didn’t know, didn’t care or didn’t believe them) and the compelling story they tell.
But first let me return to the life and time of Dr. J. Whitridge Williams, the critical historical role he played in this story and how I ‘history’ should judge him, which is to say, with an even hand that sees both sides of his remarkable (sometime remarkably good and other times remarkably bad) contribution to society in general and obstetrical medicine in particular.
Honoring Dr. J. Whitridge Williams for his Positive Contributions
In my previous essays about Dr. JWW, both as a person and in regard to his little book, I have repeatedly stressed that I do not believe these revelations are proof of any conspiracy or a nefarious attempt by him or the obstetrical profession to purposefully harm childbearing women.
Dr. J. Whitridge Williams, pioneering obstetrician at Johns Hopkins Hospital, Baltimore, Maryland; b. January 26, 1866 – d. October 21, 1931. Dr. Williams was a man of his time (b. 1866 to d. 1931) and of his station in life. The Williams were a wealthy, upper-class family who could brag about four generations of lawyers and doctors among their many male offspring. Dr. JWW’s father and brother were both physicians and his great-great-grandfather was a respected lawyer in London before immigrating to New England.
Prior to his 1914 book, Dr. Williams J. Whitridge Williams was already famous for writing the first five editions of the Williams Obstetrics textbook (original edition 1904). He was a good man trying to accomplish a big and historically important goal — financing a much needed nationwide system of modern full-service general hospitals to replace the 8,000 or so 19th century 2-10 bed privately owned hospitals that were not technologically equipped to provide 20th-century medical care nor afford to upgrade their facilities.
Acknowledging Dr. JWW’s faults in the context of early 20th century obstetrical medicine in the U.S.
Understanding how and where his good intentions went off the rails gives us the vitally important information we need to authoritatively question the status quo of American obstetrics (which is a surgical specialty) as the standard of care for normal childbirth in healthy women. Given the revelations in his book, we now can reject many self-serving or disingenuous explanations and expose claims are nothing more than self-serving smoke and mirrors.
This book reveals and promotes dark notions about eugenics and a basic prejudice against the poor working women, immigrants, and non-white populations that played out as a sub rosa campaign to increase the birth rate in the white ‘race’ (his word). Dr. JWW’s strategy was to normalize the use of the amnesic drug scopolamine and chloroform anesthesia in order to erase all memory of labor and birth in white mothers, naively believing that not remember the experience of laboring and giving birth would make these middle and upper-class white women have as many or more children than poor, black, brown and immigrant women.
Misdirection, misinformation, disinformation, and a bait-and-switch plan that sold elective hospital birth services to a specific demographic of childbearing women not because it was personally advantageous to the women themselves, but as an undeclared financial plan make private hospitals into profitable businesses and, oh, by the way, increase the birth rate in those “cultured women” that are “precisely the individuals who should propagate the species and thus promote the interests of the race“..
This included deception in their public relations campaigns and hidden motives to professionalize childbirth services as a proprietary business. Their PR machine viciously trashed the reputation of midwives, saying bluntly in women’s magazine that “midwives kill babies”. By associating midwifery care with dead babies, they successfully criminalized the practice of midwifery in the United States. As a result of these “Plans” (both Dr. JWW’s and other agendas of the AMA), childbirth services in healthy women were legally restricted obstetrically-trained MDs and the only acceptable place of birth became an acute-care hospital setting. This functionally granted the obstetrical profession and private hospitals a hundred-year (and still counting!) monopoly over the “baby business”.
The 1973 publication of the Pentagon Papers told the previously untold 20th-century story of America’s secrets about our involvement in the Vietnam War, so I can confidently describe the obstetrical profession’s Hundred Years War on normal childbirth as “the last and most important UNTOLD story of the 20th century“.
Future generations will see this abuse of trust by the obstetrical profession as having the same characteristics as the medical profession’s decades-long rejection of the Germ Theory in the 19th century. In the mid-1840, Dr. Semmelweis, a professor of obstetrics at Vienna’ huge charity hospital, was the first person to scientifically document the direct link between the unwashed hand of doctors and the deaths of the new mothers they delivered.
At that time, latex exam gloves had not yet been invented, the idea of germs was unknown, and hand-washing was not a standard part of medical practice. In Dr. Semmelweis’s busy hospital, there was an average of two maternal deaths a day, (average MMR of 5 to 50%), almost always from the fatal infection known as ‘childbed fever’ (puerperal sepsis). The professor on duty and his medical students performed autopsies on each one in order to advance their medical education and the science of obstetrics.
After these doctors and medical students finished autopsies on the most recently deceased new mothers, they walked across the hall to the maternity ward to check on all their laboring patients. This included vaginal exams, done one after another on all laboring patients, and often repeated by the medical students (for teaching purposes), without any of them ever having scrubbed and disinfected their hands — not after performing autopsies, not before vaginally examining a woman in labor, not between the exams on successive laboring patients, not before attending the next birth, and not after they were all done for the day. Within a few days, other new mothers who had been delivered by these same doctors and medical students would die from same puerperal sepsis, the disease that kept the hospital morgue filled with the lifeless bodies of newly delivered mothers and their also infected babies.
There was a 40-year period between Dr. Semmelweis’s 1840 discovery of the link between dirty hands and dead mothers and the 1881 publication of French microbiologist Louis Pasteur’s paper scientifically proving what he called “The Germ Theory of Contagion”. But no matter how much evidence was provided by Dr. Semmelweis, Dr. Joseph Lister in England, Dr. White in Scotland, Dr Oliver Wendal Holms in the US, and other doctors of his day, the obstetrical profession flatly refused to take him seriously, claiming that a “gentlemen’s hands could never to be the source of harm“.
Link to a 1952 movie about Dr. Semmelweis’s life-changing discoveries and the tragic personal consequences of his efforts.
The obvious take-home message, whether it’s decades of covert involvement by the US in distant wars or obstetrical plans to monopolize childbirth services masquerading as a public safety issue, is simply this: Once something is monetized, systemized and institutionalized, all the King’s horses and all the King’s men, all the facts and all the common sense in the world can’t stop an economic engine that is like a Sherman tank on steroids — it just rolls over anything that gets in its way, and keeps plowing forward!
And that list does not include our current, profoundly dysfunctional medical services delivery system (a deal made with the Devil between medical doctors, hospitals, medical service and supply providers and the health insurance industry).
When we get to bottom of Dr. Williams’ story, we see an undeclared Hundred Years War on healthy childbearing women and normal childbirth. The Pentagon Papers served the same revelatory function in regard to the Vietnam War.
Continued Part2-B: Insight from the recent movie about the Pentagon Papers (“The Post”) and the real story of preventable maternal deaths in the US between the 1900s and 1945 (when the antibiotic Penicillin became available) — Numbers that don’t lie
@@@@@@@@@@@@@@@@ copied to 2-B @@@@@@@@@@@@@@@@@@@@@@@@
However, Sweden kept meticulous health records for its entire population going back nearly 200 years and their maternal mortality statistics shed considerable light on this controversy. Unlike the US, they had a national program for the training of midwives and professional midwifery was identified by the Swedish government as the standard of care for healthy childbearing women.

Midwifery Training Program ~ classroom and instructorAs long as things were normal, babies were born at home under the care of a professionally-trained midwife. Anytime the midwife believed it necessary or prudent to call the local physician, he was obliged to come. If he thought it necessary, the mother was transferred to a district hospital that had obstetrical services.
In 1881 — the same year the French microbiologist Louis Pasteur’s Germ Theory of infectious disease was published and internationally-recognized — the Swedish Parliament passed a law requiring midwives and physicians that attended “cases of childbirth” to regularly and scrupulously wash their hands, abide by the principles of antisepsis and sterilize any instruments used during childbirth.
Unfortunately, no laws of this kind were passed in the US during this same period.
 In 1900, the MMR in Sweden was only 230 per 100,000 births (or a ratio of 1:431).
In 1900, the MMR in Sweden was only 230 per 100,000 births (or a ratio of 1:431).
{**Explaining “ratio” (1:431) statistics: the smaller the second number is, the more mothers are dying. It’s the same as using injury-accidents statistics to calculate how many times you can drive your car without being in hurt in an accident. If its 1 out of a 1,000, that’s good, but if its only 1 out of 10 times you get behind the wheel, that’s bad and you’ll probably have a serious car accidents 2 or 3 times a month.}
By comparison, the United States reported 520 to 850 maternal deaths per 100,000 live births (ratio of 1:127) or 3.4 times higher. One doctor of the era noted that our death rate for new mothers was the highest in the entire western hemisphere except for Brazil. 3
“As to maternal mortality, …during 1913 about 16,000 women died..; in 1918, about 23,000…and with the 15% increase estimated by Bolt, the number during 1921 will exceed 26,000.” [Ziegler, MD 1922-A]
A document published by the CDC on maternal mortality reported that our MMR was very high compared when with the lower rates achieved in much less prosperous European countries. The very highest MMR ever recorded in the US occurred between the years 1900 and 1932.
The CDC paper notes that:
“… the majority of these deaths were preventable” {due to} “obstetric care by poorly-trained and untrained medical practitioners. Inappropriate and excessive surgery and obstetrical interventions (e.g. induction of labor, use of forceps, episiotomy, cesarean section) were common during the 1920s”.

Early 1900s doctors medical bag with 2 kinds of obstetrical forceps and little glass bottles with ether to administer to the mother during the pushing 2nd) stageThis horribly high MMR precisely lines up with the obstetrical campaign championed by Dr. JWW to hospitalize increasing numbers of childbearing women in the US. Before the discovery of antibiotics (Sulfa-1938) the single most frequent killer of new mothers was an infection (septicemia or ‘blood poisoning’).
This is a known complication of unnecessarily hospitalizing healthy women, most especially if combined with routinely using invasive procedures the frequently lead to hemorrhage, which damages her immune system and makes her more vulnerable to bacterial infection. In other words, these deaths were primarily iatrogenic (caused by unnecessary or poorly performed medical treatments) or nosocomial (the result of the hospital’s bio-hazardous environment).
Two years after implementation of Dr. JWW’s Plan (1916) to electively hospitalized healthy childbearing women as maternity patients the MMR was 800 per 100,000 (1:125). In 1925 (9 years later) it shot up to 1,250 per 100,000 (1:80). This is 4,050 totally preventable maternal deaths in just nine years.
Numbers Don’t Lie ~ but tell us how many mothers die
If judged by the same statistics for the MMR in Sweden’s midwifery system 25 years earlier (1900) and using an averaged rate based for the United States MMR spread from its low in 1900 of 750 per 100k to its high in 1925 of 1,250 per 100K, we get an average MM rate for the US over those 25 years of 1,000 maternal deaths per 100K.
By subtracting the 232 maternal deaths per 100K rate in Sweden during this same time, the number of “extra” deaths in the US (i.e, higher than the Swedish system) is 768 per 100K. When we multiply that rate by 20 (the annual birth rate in the US was 2 million, which = 20 sets of 100,000) and multiply that number by the 32-year long period that the US had the highest MMR in our history, we find a total of 245,760 medically-unnecessary maternal deaths that exactly coincide with the period of medically-managed childbirth as the ‘hot new thing’ in obstetrics.
This highly contrasts with the MMR for the same historical period for the professional midwifery system in Europe that was still relying on the time-tested physiologically-based childbirth practices in concert with access to obstetrical services when indicated.

Typical hospital birth 1940-50-60s — mother under general anesthesia (note the presence of anesthesiologist at the mother head (rt side of photo) and a profoundly depressed newborn baby in the doctor’s hands.Nonetheless, the obstetrical profession, using it’s a money-fueled PR machine, managed to convince the public that the sky-high MMR in the US was all the fault of midwives and a few old-fashioned doctors still attending homebirths and doing everything the old/wrong way.
National newspaper and magazine articles quoted influential obstetrical leader as insisting that if 100% of childbearing women could be convinced to have hospital births, it would virtually eliminate these preventable deaths. Worse yet, they used these horrifically high statistics as part of a campaign strategy to promote elective hospitalization of maternity patients as so much safer.
I recently heard a radio interview of someone living in California who frequently flew back and forth to the east coast. He said he was no longer willing to do this, noting that “United is the airline that never apologizes no matter what they do“.
Apparently, the airlines and all five presidents and the Army generals that masterminded the Vietnam War were all reading out of the obstetrical profession’s playbook, since the profession never ever admits it was wrong, never says ‘sorry’ and no matter how much overwhelming scientific evidence its presented with, it never agrees to end harmful practices but instead just doubles down! {check out the ARRIVE study being used to set a new standard that routinely induces labor at 39 wks for healthy pregnant women}
 Preventable Injury & Death: What the war in Vietnam and the war on normal childbirth had in common
Preventable Injury & Death: What the war in Vietnam and the war on normal childbirth had in common
The take-home message is pretty simple. During the same pre-antibiotic era (prior to 1938), Swedish midwives within a system that provided assistance by local doctors when needed, had a ratio of maternal mortality was one of the lowest in the world in 1900 – 1 death out for every 431 births.
At that time (1900) the US rate MMR was approximately 1 out of 125 or 3.4 times higher. By 1916, the US mortality rate had increased slightly to 1 out of 127.
But by 1925 (just 9 years), the MMR had skyrocketed to 1 maternal death out of every 80 births or 5.4 times higher than Swedish midwives in 1900.
Imagine the uproar if the United States had 5.4 times more passenger planes crashed than any other countries. Given that the laws of aerodynamics are the same the world over, there surely would be outrage and inquiry and demands to ‘fix the problem’.
But these mothers died one by one by one with only their husbands and their older children and family members as grieving witnesses. There was no inquiry because they died in a hospital; this was interpreted to mean that childbirth itself was so dangerous that even the best doctors and all the extraordinary abilities of a modern hospital were not enough to save them from the wanton viciousness of Mother Nature.
In a most disturbing way, these deaths made obstetricians into heroes that were being lauded for saving the lives of thousands of healthy childbearing women every year.
BLACK News ~ 2 years of OB mismanagement = as many maternal deaths as all Vietnam War deaths
 The unnecessary military “intervention” we call the Vietnam War killed 50,000 of the 2,709,918 Americans soldiers that served in Vietnam over 11 years (1964-1975).
The unnecessary military “intervention” we call the Vietnam War killed 50,000 of the 2,709,918 Americans soldiers that served in Vietnam over 11 years (1964-1975).
The MMR in the US for maternity patients for just two years — 1924-25 — was equal to the 50,00 deaths in the bloody 11-year Vietnam War.
The maternal death ratio during this period was only slightly lower (1:80) than that of US soldiers killed in Vietnam (1:54).

Thank you, Dr. Williams, for your good intentions, but unfortunately, things went about as wrong as they possibly could and the disturbing story is a long way from being over.
https://tinyurl.com/y8udohl6
https://www.cdc.gov/mmwr/preview/mmwrhtml/mm4838a2.htm
Addition quotes from Historical Documents
The citation number at the end of each paragraph includes the year (ex. 1397) and a letter (1937-A). This combination of numbers and letters will permit interested readers to find the specific document’s name. Unfortunately, a very large number of these references are from the Transactions for the American Association for the Study and Prevention of Infant Mortality {TAASPIM}.
There were 5 of these national meeting attended by all the movers and shakers of the American obstetrical profession. As far as I know, these transcripts are not available on the internet. I had to type them into a WORD program in order to post excerpts of them online.
Here is the LINK to access the Citation Key
Ø “We have had a small but convincing demonstration by the Frontier Nursing Service of Kentucky of what the well-trained midwife can do in America. …. The midwives travel from case to case on horseback through the isolated mountainous regions of the State. There is a hospital at a central point, with a well-trained obstetrician in charge, and the very complicated cases are transferred to it for delivery”. [1937-A]^136
Ø “In their first report they stated that they have delivered over 1000 women with only two deaths — one from heart disease, the other from kidney disease. During 1931 there were 400 deliveries with no deaths. Dr. Louis Dublin, President of the American Public Health Association and the Third Vice-president and Statistician of the Metropolitan Life Insurance Company, after analyzing the work of the Frontier Nurses’ midwifery service in rural Kentucky, made the following statement on May 9, 1932:
Ø “The study shows conclusively that the type of service rendered by the Frontier Nurses safeguards the life of the mother and babe. If such service were available to the women of the country generally, there would be a savings of 10,000 mothers’ lives a year in the US, there would be 30,000 less stillbirths and 30,000 more children alive at the end of the first month of life.”
Ø “What are the advantages of such a system? It makes it economically possible for each woman to obtain expert delivery care because the expert midwife is less expensive than an expert obstetrician.
Midwives have small practices and time to wait; they are expected to wait; this what they are paid for and there they are in no hurry to terminate labor by ill-advised operative haste.” [1937-A] {*}
However, we must also take into account the fundamental sexism and chauvinism of Western culture dating as far back as biblical times. Unfortunately, far too many of these habits, which treat women and girls like a second and inferior class — are still with us today. The US Senate is still primarily an exclusive club for wealthy white men; the public sexism of the current US president is blatant, while he is not merely unrepentant but profoundly pleased with himself.
As I reviewed my internet media library of obstetrical photos amassed over the last 25 years, it was stunning to realize how many of the childbirth photos in historical obstetrical textbooks look like bondage, S&M toys, isolation and methods of torture used on terrorists — hoods over the laboring woman’s head, straight-jackets, leather wrist restraints that tied women on their back and spread-eagle to the 4 corners of their labor beds, as well different types of obstetrical stirrups.
Dr. Williams didn’t invent misogyny or male chauvinism, but its is clear that as a white male from a wealthy and socially-elite family, college educated and trained in an all-male profession, he transferred the paternalism and misogyny of his day into a pattern of behavior that treated white women as second-class citizens and poor, working-class or ethnic women as objects to be controlled and used to achieve his goals as an influential leader in the field of obstetrical medicine and as Dean of the Johns Hopkins School of Medicine.
