Easy short cut to sare –> https://tinyurl.com/ycee9xv7
{ Originally posted in 2010 }
I discovered the missing piece of the puzzle in a small book published in 1914 ‘TWILIGHT SLEEP ~ Simple Discoveries in Painless Childbirth“ {click above for access to the original source material}.
It was written by Dr. J. Whitridge Williams, a famous obstetrician, with the help of Dr. Henry Smith Williams, a physician colleague and famous science-writer of his day.
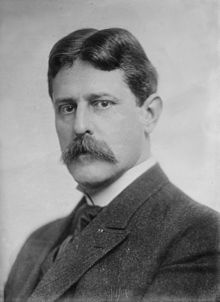 In 1914, Dr. J. Whitridge Williams, former chief of obstetrics at Johns Hopkins and current Dean of the University’s medical school, commissioned and personally participated in the writing of a book called “Twilight Sleep: Simple Discoveries in Painless Childbirth”. Despite its provocative title, its target audience was not childbearing women but husbands, the medical profession itself, public officials and wealthy philanthropists likely to provide generous endowments to Johns Hopkins and similar large teaching hospitals
In 1914, Dr. J. Whitridge Williams, former chief of obstetrics at Johns Hopkins and current Dean of the University’s medical school, commissioned and personally participated in the writing of a book called “Twilight Sleep: Simple Discoveries in Painless Childbirth”. Despite its provocative title, its target audience was not childbearing women but husbands, the medical profession itself, public officials and wealthy philanthropists likely to provide generous endowments to Johns Hopkins and similar large teaching hospitals
The main purpose of the book was to introduce and develop support for Dr. JWW’s plan for a nation-wide system of general hospitals. He envisioned a coast-to-coast network of small and medium full-service community hospitals equipped to provide the same 20th-century state-of-the-art medical services (in quality if not quantity) as his own alma mater, Johns Hopkins University Hospital in Baltimore, Maryland.
As a fully-equipped general hospital, Johns Hopkins was able to provide the same high level of comprehensive medical and surgical services as had been available in Western Europe for two centuries through a nationalized system of general hospitals. Unfortunately, there was no such ‘system’ in the United States and only a dozen or so big general hospitals in the entire country.
Dr. Williams’ book was a blueprint for dramatically changing the business model of American hospitals to make them dependable and increasingly profitable by re-writing the economic contract between society and hospitals. Topics covered in depth in this little book (128 pages) were the urgent need to develop a new countrywide system of modern, fully-equipped general hospitals AND especially Dr. Williams’ innovative ideas for funding such a massive project without involving the federal government or depending on any financial scheme that the AMA thought smacked of its dreaded bug-a-boo: ‘socialized medicine’.
Last but certainly not least was a controversial topic that occupied the first four of the book’s eight chapters and might best be described as a fanciful and fact-free form of “Obstetrical Darwinism“.
Dr. Williams tells an imaginative story about a new childbirth-related pathology identified by him that only affected “civilized” and “cultured” women of the “most highly developed type” (i.e. healthy middle and upper-class white women).
He described the problematic effects of civilization on this particular demographic of smart, socially sophisticated, educated, and economically-secure American wives, noting that: “such cultured women are precisely the individuals who should propagate the species and thus promote the interests of the race“.
This concept also expresses his belief that the lower classes, especially immigrants and black and brown people were ‘precisely’ the type of people who should NOT be “propagating the species”. Therefore upper-class white women had to be convinced to have more babies!
Dr. Williams paints a Darwinian picture of a devolving evolution due to “the hot-house conditions of civilized existence.” He explains:
“These artificial conditions often determine that the less fit rather than the most fit individuals shall have progeny and that undesirable rather than the desirable qualities shall be perpetuated.”
The problem Dr. William’s alluding to is a pathological level of childbirth-related pain experienced by healthy women in this demographic. This extreme pain caused dangerous levels of psyche distress that were a shock to the system of these naturally “nervous and sensitive women” were overwhelmed and mentally unable to cope.
This was especially severe for the most ‘delicate‘ type of women. The normal pain of a spontaneous labor and birth put these women at great risk of a nervous breakdown, so severe that prolonged hospitalization in a mental institution would become necessary.
Dr. Williams pointed out the many problems that could befall husbands if they were so unlucky as to have their wives languishing away in an asylum for weeks or months after giving birth, leaving their husbands to care for the older children and a newborn, while also attempting to earn a living and pay the mental institution.
To prevent these horrific problems for wives that were intelligent, sensitive or delicate (and whose wife doesn’t fit into at least one of those categories), Dr. Williams instructed husbands about the “Simple Discoveries in Painless Childbirth” described in his book, and strongly recommends that these men no longer permit their wives to have a baby at home under the care of a community midwife or country doctor.
Instead, the smart thing to do is insist that their wives go immediately to the hospital when labor begins. Then their wives should be properly medicated with frequently repeated doses of Twilight Sleep drugs throughout the many hours of labor and only be allowed to give birth after being rendered unconscious by general anesthesia.
This would prevent the ‘little woman’ from having a postpartum psychotic episode and protect her husband from becoming a victim once-removed from the dangers of a ‘natural birth’ in this ‘delicate’ demographic — that is, one without the benefit of drugs and anesthesia and associated obstetrical interventions, such as episiotomy, forceps delivery, manual removal of the placenta and stitches to close the sizable episiotomy incision.
Fortunately, and no doubt by the sheerest of happenstances, the pathological level of childbirth-related pain that required hospitalization only affected the very same middle and upper-class families that luckily could afford these much more expensive hospital-based obstetrical services.
In his own words: Dr. JWW’s explained that:
“… women of primitive and barbaric tribes appear to suffer comparatively little in labor, coupled with the fact that it is civilized women of the most highly developed nervous or intellectual type who suffer most.”
“… the cultured woman of to-day has a nervous system that makes her far more susceptible to pain and to resultant shock than was her more lethargical ancestor of remote generations….”
“… every [labor] patient who goes to the hospital … will pass through what otherwise would be a dreaded ordeal in a state of blissful unconsciousness.”
“In Johns Hopkins Hospital, no patient is conscious when she is delivered of a child. She is oblivious, under the influence of chloroform or ether.
The book’s target audience was definitely not childbearing women or even the public, but certainly would be of interest to husbands who could afford to pay for hospital-based maternity care and to all the hospitals of the era that were eagerly lining up to provide this very profitable fee-for-service that included the elective hospitalization of a million or more healthy childbearing women every year as paying customers.
The Dark Side of the Moon – Institutionalizing maternity care and its consequences for healthy childbearing women and their families
Unfortunately for us, Dr. J. Whitridge Williams’ plan was a two-edged sword. He was a true hero that did marvelous things for the American people by providing them with dependable access to state-of-the-art hospital services. Modern medical miracles, which would someday include heart transplants and re-attaching severed limbs, were for the first time available to everyone in their own community or within reasonable driving distance. Over the last century, this certainly has saved many million lives and untold suffering.
But at the same time, Dr. JWW was also a villain. His economic “plan” for electively hospitalizing healthy maternity patients, which successfully financed a for-profit general hospital system all across the entire country, ALSO resulted in the most profound change in normal childbirth practices in the history of the human species.
Hospital-based obstetrical services, as the new and modern standard for childbirth in America immediately replace the personal services of a midwife with institutional-based care provided by virtual strangers.

1917: Profoundly-medicated and semi-conscious laboring woman under the influence of powerful Twilight Sleep drugs. She has been encased in the hospital’s version of a ‘straight jacket’ for her own ‘safety’. Her arms are bound so she won’t hurt herself and the restraint device is tied to the rails of the bed to prevent her from falling out bed and breaking an arm or knocking out one of her teeth in case she gets agitated (a side-effect of the drug scopolamine)
In Dr. JWW’s own words:
“… every patient who goes to the hospital may have full assurance that she will pass through what would otherwise be a dreaded ordeal in a state of blissful unconsciousness.”
On his watch, healthy childbearing women were turned into the hospitalized patients of the new surgical specialty of obstetrics and gynecology and normal childbirth became a surgical procedure ‘performed’ by a physician using forceps on a mother rendered unconscious by general anesthesia.
“In Johns Hopkins Hospital,” said Dr. Williams, “no patient is conscious when she is delivered of a child. She is oblivious, under the influence of chloroform or ether.
“Let the robust, phlegmatic, nerveless woman continue to have her children without seeking the solace of narcotics or the special attendance of expert obstetricians if she prefers. But let her not stand in the way of securing such solace and safety for her more sensitive sisters.”
As for the effect of narcotic drugs, scopolamine and anesthetics gases on the unborn baby, Dr. William’s book boldly makes the case that the baby is it is actually safer for the baby when its mother is medicated with hallucinogenic and amnesic drug scopolamine.

The very early days of hospital nurseries, in which 6 babies are bunked together in a special hospital bed
“Famed scientists disputes fetal-neonatal damage as a result of the scopolamine narcosis of its mother:
“the tendency to retard respiration on the part of the child may sometimes be beneficial, preventing the infant from inhaling too early, thus minimizing the danger of strangulation from inhalation of fluids.
It appears that statistics of the Frauenklinik show that the percentage of infant mortality is low.”
“As against an infant mortality of 16 percent [editor’s note ~ that is 160 baby deaths per 1,000 births] for the state of Baden [Germany] in the same year, a report on 421 ‘Twilight Sleep’ babies showed a death-rate of 11.6 percent [i.e. NNMR of 116 per 1,000]
“For this strikingly low mortality of the children during and after birth under semi-narcosis, an explanation was sought of Professor Ludwig Aschoff, the great German authority on morbid anatomy.
He offered the theoretic explanation that slight narcotization of the respiratory organs during birth by extremely minute quantities of scopolamine[e] is advantageous to the child, as it tends to prevent permanent obstruction of the air-passage of children by premature respiration during birth.”
This new system replaced the participation of a fully conscious and undrugged laboring woman who can talk and walk around and ask for various kinds of support and follow the suggests of other to help her be more comfortable or to push more effectively and remember the birth of her baby with a physically-immobile drugged laboring woman who is in a virtual ‘zombie’-like trace throughout her labor. No family members are allowed to be present in the L&D ward.
As a hospitalized labor patient, she will be kept lying flat in bed with leather wrist-restraints and obstetrical version of a straight-jacket until its time to move her to the delivery room for the surgical procedure of “delivery”. Normal childbirth for a healthy woman began by rendering her unconscious under general anesthesia while the surgical procedure of ‘delivery’ was performed by an obstetrically-trained physician-surgeon in a special operating room. Obstetrically managed delivery included the routine use of episiotomy, forceps, manual removal of the placenta and stitching up the episiotomy incision in her perineum.
As soon as the baby was delivered it was taken away to the hospital nursery (still unseen by its mother) so it can be closely observed for the next 12 hours to be certain that the narcotic drugs and anesthetic gases giving to its mother do not cause for her newborn baby to stop breathing or suddenly choke. The still unconscious mother will be moved to an OB recovery room for the next couple hours without yet knowing if she had a boy or a girl.
Dr. JWW’s plan from the perspective of the hospital system:
Phase #1: The first coordinated step required that all existing hospitals in the US open new ‘lying-in wards’, hire a nursing staff and arrange for the medical management of normal childbirth by local doctors. After the birth, both mother and new baby would remain hospitalized for the following two-weeks, requiring a postpartum ward for new mothers and a newborn nursery to provide care to babies.
Phase #2 was to identify or create a demographic or ‘target population’ whose use of these new services would be profitable to the hospital. Dr. Williams answer was to target middle and upper-class healthy maternity patients who were financially able to pay for these services came up with was both an obvious and at the same time, a brilliant idea — what he and many others considered to be w was middle and upper-class women those families who could afford to pay for hospital-based maternity services
Phase #3 closed this innovative financial loop. What started as relatively the small idea (offering maternity services) expressly for the purpose of making a profit, were carried out at a scale that would fundamentally and forever change the nature of the hospital business. The old restraints that keep hospitals unprofitable were being swept away, to be replaced by a model that ultimately created a modern nationwide system of well-equipped general hospitals as the ‘gift that kept on giving’.
In a remarkable bit of reverse engineering, Dr. Williams turned the story as we think of it today on its head. To our modern perspective, this seems like a “tail wags the dog” scenario, but in his version, the ‘tail’ was what we now think of as the full-service general hospital in every community.
The profitability of the ‘baby business’ is what made everything else – the modern hospital system — possible.
Telling the Truth, the whole Truth, and Nothing but the Truth, so help me GOD!
But we cannot ignore the unintended consequences that resulted from Dr. Williams’ plan to electively hospitalize healthy maternity patients as paying customers — the cash cow of a new, profit-driven hospital system and a financial bridge to Dr. William’s meta-goal, which was financing a nationwide system of general hospitals.
Dr. Williams own words highlight the direct connection between elective hospitalization of healthy maternity patients, and the ability to use the profitable revenue that would generate, to purchase capital-expensive equipment (such as x-ray equipment) and enable a specialty facility to upgrade itself into a full-service general hospital:
“With this kind of dependable patronage, lying-in (ie. maternity) hospitals would be able to … provide laboratory, x-ray and other services necessary to provide for a well-equipped surgery department”.
From Dr. Williams’ perspective, and later on economic interest of the obstetrical profession, this “dependable patronage” was NOT primarily done for the safety and well-being of childbearing women and their unborn and newborn babies. The facts are clear and unambiguous: Inventing elective hospitalization of healthy for normal childbirth was not about better or safer care for mothers and babies, it was about developing the ‘patronage’ of childbearing families so these normal biological acts would occur in a proprietary setting where, like taxi cabs, the meter was always running and families billed for every aspect of these services. This new profit stream would then be used to upgrade and remodel hospital buildings and purchase capital-intensive equipment like institutional autoclaves (sterilizers), microscopes, x-ray machines and expanding the size of the hospital.
When all this was sorted out, the newly upgraded hospital would be able to charge even MORE for its services and be in a better position to compete with other hospitals in the area. Nowhere in these economic statistics does it mention that iatrogenic diseases — especially hospital-acquired septicemia, the potentially-fatal infection historically known as childbed fever — would be responsible for the deaths of 10,000 new mothers every year (a number that rose to 25,000 in the year 1925).
Year after year, literally thousands of new mothers died of deadly hospital-acquired infection, and still, the obstetrical profession and organized medicine continued to insist that hospital childbirth was the new, modern, and far better, safer way to have a baby. This disastrous situation continued unabated until the bacteria-killing drug sulfa and the antibiotic penicillin became widely available to the public in March of 1945
What all this means in our own time

Today over 4 million American women have hospital births every year. Approximately 70% to 80% of these women are healthy and have a normal pregnancy with one baby in a head-down position that delivers at term.
Instead of chloroform, up to 95% of labor patients are given epidural anesthesia. And like a magic trick for the hospital, (pulling a rabbit out of a hat!) this biological process automatically makes a second ‘paying customer’ — the new baby that is officially admitted to a hospital nursery and billed to the mother’s account.
It is not unusual for a healthy woman who gives birth to a healthy term baby with good Apgars to receive a hospital bill for her two-day stay that varies from a low (!) of $12,000 to as much as $50,000. I personally know a family that has a normal birth at a local hospital who received a bill for $50,000.
Approximately 30 million people in the US are admitted to acute-care hospitals every year. Maternity ‘patients’ (i.e. mothers and babies) account for 8 million of those annual admissions. Decade after decade, the two most frequent admitting diagnoses are ‘normal childbirth with no complications’ and ‘newborn with no complications‘.
In this rase to fill up hospital beds with paying customer, second place goes to x-ray angioplasty procedures, which is a mere 700,000 a year.
Dr. JWW’s plan to use electively hospitalized maternity patients as the cash cow of hospitals as profit-making businesses is still alive and well in the 21st century.
However, this fascinating historical story is far, its a long way from being over; in many ways, the next stage is even more enlightening.
Continue to ~ Part 1-b
So stay tuned!
TinyURL for Part 1 of this ~https://tinyurl.com/ycee9xv7.
To access parts 2 & 3, just clicking on the link at the bottom of parts 1 and 2. Additional posts on this topic usually have a unique TinyURL at the beginning.
 The working title of my research is (so far):
The working title of my research is (so far):
“How Childbirth Got Trapped on the Wrong Side of History: How healthy women were turned into the patients of a surgical specialty and normal birth into a surgical procedure — the last and most important UNTOLD story of the 20th century”.
Total Word Count for this post: ~ 3751
