| EXCERPTS & Commentary for mothers, midwives & others
NOTE: The full PDF version of this paper should be available online.
The lead author, Dr David Grimes, is one of a very small number of physicians to be board-certified in both Ob-Gyn and preventative medicine. He trained at UCSF and worked with midwives at San Francisco General Hospital. In 1994 he was asked by the Medical Board of California to define “supervision” of LMs by obstetricians, per the requirement of the newly passed LMPA.
If you have read my post on how to make physician supervision work, it was Dr. Grimes suggested definition of a workable model of obstetrical supervision – that is, the practitioner identified for an LM to contact when her client required medical evaluation or treatment or had needs that otherwise exceeded her scope of practice — that was the heart of our ideas for crafting regulations.
I have included his bio about him at the bottom of this research paper.
David A. Grimes, MD, and Jeffrey F. Peipert, MD, PhD
VOL. 116, NO. 6, DECEMBER 2010
OBSTETRICS & GYNECOLOGY 1397
From FHI, Research Triangle Park, North Carolina; the Department of Obstetrics and Gynecology, University of North Carolina School of Medicine, Chapel Hill, North Carolina; and the Division of Clinical Research and the Department of Obstetrics and Gynecology, Washington University in St Louis School of Medicine, St. Louis, Missouri.
Corresponding author: David A. Grimes, MD, FHI, PO Box 13950, Research Triangle Park, NC 27709; e-mail: dgrimes@fhi.org.
 Abstract Abstract
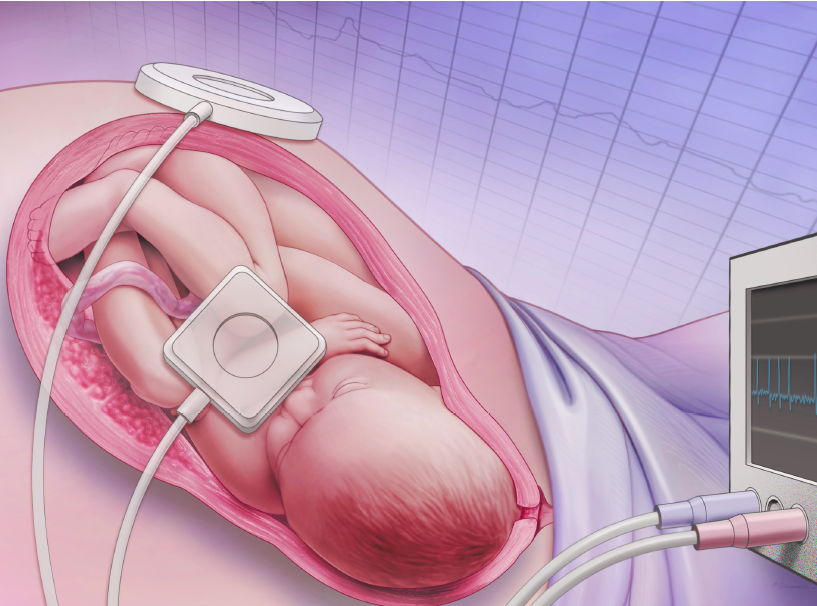
Electronic fetal monitoring has failed as a public health screening program. Nevertheless, most of the four million low-risk women giving birth in the United States each year continue to undergo this screening.
The failure of this program should have been anticipated and thus avoided had the accepted principles of screening been considered before its introduction. All screening tests have poor positive predictive value when searching for rare conditions such as fetal death in labor or cerebral palsy. This problem is aggravated when the screening test does not have good validity as is the case with electronic fetal monitoring. Because of low-prevalence target conditions and mediocre validity, the positive predictive value of electronic fetal monitoring for fetal death in labor or cerebral palsy is near zero. Stated alternatively, almost every positive test result is wrong. To avoid such costly errors in the future, the prerequisites for any screening program must be fulfilled before the program is begun.
*A new drug must present a rigorous set of experimental data before it is licensed for use, and until it is licensed, patients are not permitted to obtain it. The same rigor should apply to medical screening.” [1]
{* I paraphrased just this introductory sentence for clarity – all the rest of document is original text only}
Electronic fetal monitoring has failed as a public health screening program. Randomized controlled trials of electronic fetal monitoring compared with intermittent auscultation reveal that electronic fetal monitoring statistically significantly increases instrumental and cesarean deliveries for women but provides no long-term benefits for children. [2]
 Clinicians, too, have suffered indirectly because of the epidemic of litigation and “expert” testimony that electronic fetal monitoring has spawned about fetal heart-rate tracings. [3] Sadly, the failure of electronic fetal monitoring could have, and should have, been predicted and thus avoided. Clinicians, too, have suffered indirectly because of the epidemic of litigation and “expert” testimony that electronic fetal monitoring has spawned about fetal heart-rate tracings. [3] Sadly, the failure of electronic fetal monitoring could have, and should have, been predicted and thus avoided.
The fundamental error made decades ago was viewing electronic fetal monitoring as an obstetric technology for an individual woman, and not as the national public health screening program that it is.
This error was compounded by naïvete´ about screening principles and exaggeration of the value of positive results. [4]
What Is Screening?
Screening is the testing of large numbers of apparently well persons to identify those at increased risk of disease. Because screening is done among asymptomatic persons, the ethical burden on those ordering the tests is higher than when performing tests on ill persons. This is because false-positive results of screening can deprive persons of their perceived health, prompt unnecessary diagnostic tests and procedures with their attendant morbidity, and waste money and other resources.5 Hence, stringent requirements must be met before a screening program starts. This did not happen with electronic fetal monitoring.1 We will restrict our commentary to the usual use of electronic fetal monitoring as a screening test in asymptomatic women; when used in women with signs or symptoms suggestive of adverse outcomes (eg, meconium-stained amniotic fluid), electronic fetal monitoring could be considered a diagnostic test.
Avoiding …. Mistakes
 Electronic fetal monitoring during labor is not recommended for women at low risk. [10 , 11, 12] Despite these consistent recommendations on both sides of the Atlantic Ocean, approximately 3.4 million US women at low risk are screened annually with electronic fetal monitoring.[10] Electronic fetal monitoring during labor is not recommended for women at low risk. [10 , 11, 12] Despite these consistent recommendations on both sides of the Atlantic Ocean, approximately 3.4 million US women at low risk are screened annually with electronic fetal monitoring.[10]
{Note by FG: Situations in which physicians continue to order or perform procedures that lacks a scientific foundation or are in direct opposition to the best evidenced is called “physician preference” and describes a choice made by the doctor to ignore professional sources due to some personal benefit to themselves, including a perceived advantage in case there is a lawsuit. This represents a process of asymmetrical risk-shifting, cost-shifting and at times, blame-shifting, in which these burdens are shifted from the physician to the mother and/or the unborn baby.
Nonetheless, it still is a personal and not a professional or scientifically-based choice that is almost always done without first informing the patient and obtaining the patient’s consent. This means the physician did not acknowledge that the recommended treatment reflected his or her personal choice and therefore was not evidence-based care but 19th century “authority-based” medicine predicated on the individual opinion of that particular doctor at that particular time.}
Aside from the wasted money and time, electronic fetal monitoring increases operative deliveries, yet offers no lasting benefit to children. [2,10]
 Electronic fetal monitoring harms women; compared with vaginal births, cesarean deliveries are associated with a statistically significant increase in uncommon but serious complications, including: Electronic fetal monitoring harms women; compared with vaginal births, cesarean deliveries are associated with a statistically significant increase in uncommon but serious complications, including:
- cardiac arrest
- hemorrhage requiring hysterectomy
- venous thromboembolism
- major infection
- Cesarean deliveries have also been linked with placenta accreta in later pregnancies
Electronic fetal monitoring should be reserved for women at increased risk of adverse outcomes [11] in whom screening will perform better. As the frequency increases, the positive predictive value will rise.
However, for rare outcomes, the improvement is negligible. For example, if the risk of fetal death in labor were 10-fold higher (500 per 100,000) than that in Table 3, the positive predictive value would be 285/ 31,130, or 1%, assuming the same sensitivity and specificity.
With a 10-fold increase in the frequency of intrapartum death, 99% of positive tests are still wrong, illustrating the limited value of such screening. This is an inescapable, but little understood, principle of screening.
More common but less serious, fetal acidemia at birth may provide the most charitable assessment of electronic fetal monitoring. In a large randomized controlled trial with a frequency of fetal acidemia at birth (umbilical cord artery pH less than 7.15) of 10%, nonreassuring fetal heart rate patterns had a positive predictive value of 37%.[13] Even for this common outcome, most positive tests were wrong.
Final Conclusions:
Screening is a public health strategy that transcends clinical disciplines.
Whether the target condition is neural tube defect, scoliosis, osteoporosis, abdominal aortic aneurysm, or cerebral palsy, accepted criteria for mounting a screening program must be satisfied before screening is begun. [5,12]
Paradoxically, few clinicians who routinely use electronic fetal monitoring in labor would use a pregnancy test (or home smoke detector) that is wrong almost every time a positive signal appears. [4]
Careful evaluation of a screening test must be done before, not after, a program has been widely adopted and disseminated. [1]
By then, the damage has been done.
REFERENCES
1. Law M. Screening without evidence of efficacy. BMJ 2004;328: 301–2.
2. Alfirevic Z, Devane D, Gyte GM. Continuous cardiotocography (CTG) as a form of electronic fetal monitoring (EFM) for fetal assessment during labour. The Cochrane Database of Systematic Reviews 2006, Issue 3. Art. No.: CD006066. DOI: 10.1002/14651858.CD006066.
3. Lent M. The medical and legal risks of the electronic fetal monitor. Stanford Law Rev 1999;51:807–37.
4. Steurer J, Fischer JE, Bachmann LM, Koller M, ter Riet G. Communicating accuracy of tests to general practitioners: a controlled study. BMJ 2002;324:824 – 6.
5. Grimes DA, Schulz KF. Uses and abuses of screening tests. Lancet 2002;359:881– 4.
6. Martin DH, Cammarata C, Van Der Pol B, Jones RB, Quinn TC, Gaydos CA, et al. Multicenter evaluation of AMPLICOR and automated COBAS AMPLICOR CT/NG tests for Neisseria gonorrhoeae. J Clin Microbiol 2000;38:3544 –9.
7. Larma JD, Silva AM, Holcroft CJ, Thompson RE, Donohue PK, Graham EM. Intrapartum electronic fetal heart rate monitoring and the identification of metabolic acidosis and hypoxic–ischemic encephalopathy. Am J Obstet Gynecol 2007;197:301.e1– 8.
8. Walsh CA, McMenamin MB, Foley ME, Daly SF, Robson MS, Geary MP. Trends in intrapartum fetal death, 1979 –2003. Am J Obstet Gynecol 2008;198:47.e1–7.
9. Hirtz D, Thurman DJ, Gwinn-Hardy K, Mohamed M, Chaudhuri AR, Zalutsky R. How common are the ‘common’ neurologic disorders? Neurology 2007;68:326 –37.
10. Intrapartum fetal heart rate monitoring: nomenclature, interpretation, and general management principles. ACOG Practice Bulletin No. 106. American College of Obstetricians and Gynecologists. Obstet Gynecol 2009;114:192–202.
11. National Collaborating Centre for Women’s and Children’s Health. Intrapartum care. Care of healthy women and their babies during childbirth.
Available at: www.nice.org.uk/nice-media/live/11837/36275/36275.pdf Retrieved June 4, 2010.
12. US Preventive Services Task Force. Guide to clinical preventive services. 2nd ed. Baltimore (MD): Williams & Wilkins; 1996.
13. Vintzileos AM, Nochimson DJ, Antsaklis A, Varvarigos I, Guzman ER, Knuppel RA. Comparison of intrapartum electronic fetal heart rate monitoring versus intermittent auscultation in detecting fetal acidemia at birth. Am J Obstet Gynecol1995;173:1021– 4.
@@@@@@@
David Grimes, M.D., FACOG, FACPM is one of a small number of U.S. physicians Board-certified in both obstetrics and gynecology and in preventive medicine.
He obtained his undergraduate degree in biology from Harvard then attended medical school as a Morehead Fellow at the University of North Carolina. He completed his residency in obstetrics and gynecology at that institution, interrupted by two years at the U.S. Centers for Disease Control and Prevention. After earning certification from the American Board of Obstetrics and Gynecology, he earned certification in Public Health and General Preventive Medicine from the American Board of Preventive Medicine.
Dr. Grimes has had a dual career in clinical ob/gyn and in preventive medicine for the past three decades. He served as an epidemiologist at the Centers for Disease Control for nine years. He has also been a faculty member in four medical schools: Emory University, University of Southern California, University of California-San Francisco, and University of North Carolina. He has received major teaching awards from each of the four schools. He serves as Principal Investigator for a National Institutes of Health T32 training grant (Training in Epidemiology and Clinical Trials), a consortium of the University of North Carolina, Duke Clinical Research Institute, and Family Health International.
Through the auspices of the Berlex Foundation Faculty Development Courses, he has taught research methods to over 1400 obstetricians/gynecologists in the U.S. Through the Centers for Disease Control and Prevention and Family Health International, he has taught research methods to physicians and scientists in Kenya, Ethiopia, India, Bangladesh, and Egypt. Over the past thirty years, he has lectured extensively in the U.S. and in countries on six continents.
He has chaired or served as a member of Data Safety and Monitoring Boards for randomized controlled trials being conducted by the World Health Organization, the National Institutes of Health, and the pharmaceutical industry.
Dr. Grimes’ research interests have focused on fertility regulation, technology assessment, sexually transmitted diseases, and clinical epidemiology. He has published over 300 peer-reviewed articles, forty textbook chapters, and several books. He serves on the editorial boards of several journals, including The Lancet, Obstetrics and Gynecology, Obstetrical and Gynecological Survey, and Contraception. In 1994, he received the Issue of the Year Award from the American College of Obstetricians and Gynecologists and in 1997 the Distinguished Service Award from the same organization. In 2006, Dr. Grimes was elected to the Institute of Medicine of the National Academies of Science. In 2007, he was elected an Honorary Fellow of the Faculty of Sexual and Reproductive Healthcare of the Royal College of Obstetricians and Gynaecologists.
He currently serves as Vice President of Biomedical Affairs at Family Health International and Clinical Professor in the Department of Obstetrics and Gynecology at the University of North Carolina School of Medicine. |
 Begin with this link, which has references from studies on efficacy of EFM published in professional journals between 1969 & 1978
Begin with this link, which has references from studies on efficacy of EFM published in professional journals between 1969 & 1978