
Easy-2-share link to this post: https://tinyurl.com/y53plzej
EFM Mayday Series ~ Chapter 5 ~
Twenty-first century maternity care for health childbearing women with normal pregnancies must require the American obstetrical profession to provide full information about the inherent risks of all obstetrical interventions. This particularly applies to the routine induction or augmentation of labor with the drug Pitocin, the routine use of continuous EFM during the labors of low- and moderate-risk women and the “liberal” use of Cesarean surgery under the false premise that surgical delivery is better, safer or easier than a normal vaginal birth.
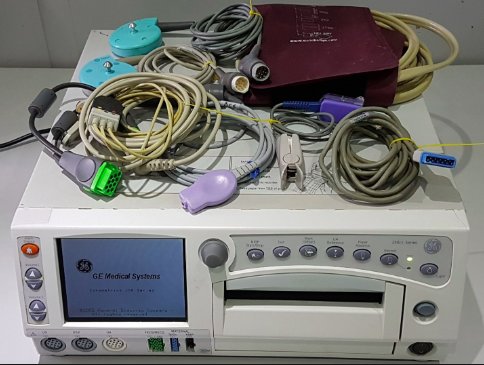
The negative effects associated with the routine use of continuous EFM during labor by healthy women have been amply and repeatedly documented since the technology was first adopted by hospitals in the 1970s. This expensive technology requires the childbearing woman to labor while lying in bed, or standing right next to her bed so the cables of the electronic monitoring device encircling her pregnant abdomen can be connected to its central processing unit.
Unfortunately for all of us, routine use of continuous EFM produces no benefit to either mother or unborn baby. Nonetheless, the second most frequently cited reason for performing a Cesarean in first-time mothers is “non-reassuring fetal heart rate” according to the EFM.
The negative effects of routine EFM are cascading and lead to a statistically-significant increase in surgery-related complications at the time of the Cesarean and in future pregnancies, such as post-Cesarean placental abnormalities, risk associated with repeat C-sections and 6% secondary infertility.
This includes a significant increase in the rate of Cesarean-related maternal deaths due to intra-operative, immediate post-op, delayed and long term complications of Cesarean section. Normal bleeding from tiny blood vessels during and after the surgery cause post-operative adhesions to form in the new mother’s abdomen, making repeat C-sections more difficult and more dangerous than the first (or ‘primary’) Cesarean.
All this information must be included in the public discourse.
In addition, modern maternity care in America must immutably establish the legal and ethical right of childbearing women to say “no” to unwanted obstetrical interventions (per ACOG Committee Opinion #214).
A political action supporting & protecting our right to say “NO” to unwanted sexual advances as well as invasive obstetrical protocols unless we have given our informed consent.

Standing on the shoulders of the Me-2 movement to launch Me-3:
A contemporary women’s movement specifically related to exposing and combating inappropriate gender-related issues relative to sexual conduct in which the male of the species takes advantage of the female of the species.
This included unwanted sexual advances or being forced to have non-consensual sexual arrangements (such as date rape). It also includes verbal insults and free-form socially-sanctioned humiliating of women — for sport or political gains — relative to their gender-related biology and reproductive health.
One infamous example of this was a prolonged, often daily verbal attack by Talk-radio host Rush Limbaugh. He targeted a young woman by name who testified before the US Congress about access to and the expense of oral contraceptives. Mr. Limbaugh repeatedly ranted and make fun of the idea that ‘normal’ (i.e. non-controversial) access to reproductive health services, such as birth control pills and medically prescribed hormonal treatments that require taking oral contraceptives, should be covered by health insurance plans.
What is ME3, and how is it different?
Me3 greatly expands the Me2 conversation beyond the sex and power-based interactions btw a man and a woman, or a between men and women in those instances that devolve into a generally unequal, demeaning and ultimately harmful contact in which the woman objects and says “NO” but the man dismisses, belittles and simply refuses to stop his aggressive behavior.
Me3 opens up female gender-related issues to other areas of reproductive biology, to historical issues and to the modern consequences of decisions made decades, even centuries ago by men acting from a male-centric social perspective within male-controlled professions such as the historical development of obstetrical medicine as long ago as the ancient Greek and Roman civilizations.
Unfortunately, traditional ways of thinkings and customs from 2,500 years ago still negatively impact women in the 21st century.
The new surgical speciality of Obstetrics and Gynecology ~ USA, 1910
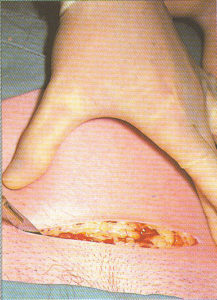
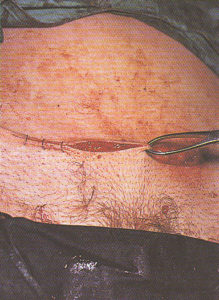
Obstetrical surgeon making the initial skin incision for Cesarean delivery
Beginning with Hippocrates in Ancient Greece, obstetrics was seen as part of the general (i.e. not a surgical) practice of medicine — that is, birth was not seen a surgical process ‘performed’ by the doctor, but was a facet of normal female biology in which the mother gave birth under her own power.
This perspective applied even if a physician sometimes had to assist the process of birth by cutting or repairing an episiotomy incision, using forceps or retrieving a retained placenta.
However, gynecology has always been primarily a surgical speciality. In 18th and 19th century America, the professional relations between these two medical disciplines were very unfriendly, as each discipline saw themselves as the best choice for all of a woman’s reproductive and childbirth needs. At that time, general practitioners (GPs) were able to use obstetrical forceps as part of their scope of practice, but they were not trained to perform Cesarean surgery.
This historical power-disparity between GPs) and GYN surgeons made the two professions into adversaries and economic competitors.
Unfortunately for general practitioners this was not a level playing field. When the maternity patient of a GP needed a C-section, he had no choice but to call on a gynecological surgeon to perform the operation. However, GYN surgeons didn’t respect or trust the medical skill of a mere “GP” and certainly didn’t like being at their beck and call.
On the other hand, general practitioners didn’t like being lorded over by gyn surgeons, and were keenly aware that GYN surgeons never reciprocated by referring healthy maternity patients to GPs. If this sounds like the historical and contemporary relationship between midwives and OBs, then you perfectly understand the contentious issues between GP and GYN surgeons in the late 19th century and early 20th century.
Dr. J. Whitridge Williams, MD, trained as a gynecological surgeon, appointed Chief of Obstetrics & then Dean of Johns Hopkins School of Medicine, 1900-1923
In 1899, Dr. JW Williams (author of “Williams’ Obstetrics“) commented on this disturbing professional rivalry that occasioned so many bitter disagreements. The relationship between the two disciplines was marked by a deep mutual distrust, hot tempers, name-calling and occasional fist fights in public.
Another physician of that era said:
“At present, gynecology considers that obstetrics should include only the conduct of normal labor, or at most … cases that can be terminated without radical operative interference, while all other conditions should be brought to him [i.e. the gynecologist] — in other words, that the obstetrician should be [nothing more than] a man-midwife.
The advanced obstetrician, on the other hand, holds that everything connected with the reproductive process of women is part of his field, and if this contention were sustained, very little would be left for the gynecologist.”
Dr. Williams was convinced that neither profession could advance until both joined forces to create a hybrid profession of obstetrics and gynecology as a new surgical speciality in America. In the early 20th century, influential leaders of these two disciplines joined forces to eliminate economic competition and elevate both disciplines by entering into a “gentleman’s agreement” that created the new American surgical speciality of Obstetrics and Gynecology.
It’s hard not to notice that the one thing these two disciplines never thought of, which was asking women what they wanted when it came to reproductive health, maternity care and normal childbirth.
Pulling the rug out from underneath Childbearing Women
The idea that obstetrics should be part of a surgical speciality and that childbirth was an operation performed by the surgically-trained doctors on woman rendered unconscious under general anesthesia started with America obstetricians and was confined to the US for a very log time.
This new hybrid discipline of medical and surgical practices reflected the historical male perspective of the medical profession. Doctors generally saw the female gender as being biologically inferior to males, as well as reflecting the historic social bias against women as “emotional creatures” who were intellectually inferior to men.

1910 labor patient being prepared for Twilight Sleep drugs — frequently repeated injections of scopolamine and narcotics . The L&D nurse placed a hood over the woman’s head and then put her in an obstetrical straight jacket with a single continuous sleeve that is pins the mother’s arms behind her back,
This new surgical discipline in the US promptly defined pregnancy as a nine-month disease that required a surgical cure.
Obstetrician-gynecologists likewise defined normal childbirth as surgical procedure that legally could only be ‘performed’ by an MD trained in obstetrical surgery.
This turned healthy childbearing women into the patients of a surgical speciality and normal childbirth into a surgical procedure. As a critical historical event, this is the last and most important UNTOLD story of the 20th century.
Under this new system, the professional role of L&D nurses was to provide pre-op and post-op support services to the surgical speciality of obstetrics.
Having defined childbirth as a surgical operation, the first-stage labor was referred to about by doctors as “the waiting period before the doctor was called“. The nurse’s job was to provide pre-op care while teach of her ‘surgical’ patients labored .
When the birth-operation became imminent, nurses called the doctor to come to the L&D and assist the obstetrical surgeon during the surgical procedure of “delivery” conducted in a sterile operating room.
As an operation, vaginal delivery included rendering the mother-to-be unconscious under general anesthesia (ether or chloroform). Then an episiotomy was performed, forceps were used to deliver the baby, followed by the manual removal of the placenta and suturing of the perineal incision.
The intra-operative period ended with the obstetrician’s last stitch. At that point, the newborn baby and newly-delivered mother both became “post-op” patients whose care again reverted to the nursing staff. The baby was sent to the newborn nursery and the still-unconscious new mother to a postpartum recovery room.
The end of normal birth and those that supported the normal physiology of childbirth
Since midwives were trained in the professional discipline of midwifery and not the surgical discipline of obstetrics, the obstetrical definition of birth as a surgical procedure instantly eliminated access to the non-interventive care provided by midwives.
Ultimately, the obstetrical definition of normal childbirth as a surgical procedures resulted in the abolition of professional midwifery in the United States for the following 75 years.
The Surgical Billing Code for normal childbirth: NSVD
This classification of normal vaginal childbirth (no forceps or c-section) as a surgical procedure in the US has never been changed, and today, obstetrician fees are still being reimbursed under the surgical billing code “NSDV” i.e. Normal Spontaneous Vaginal Birth.
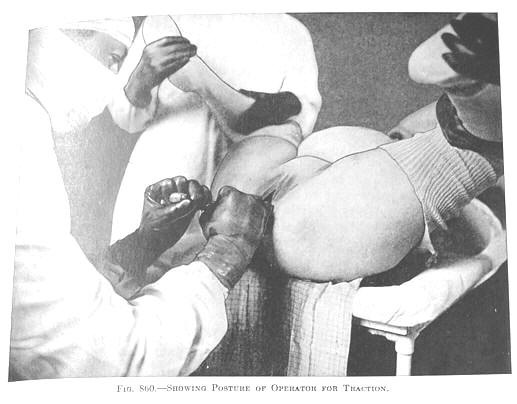
1920s forceps delivery under general anesthesia on a labor patient who first was medicated with the amnesic and hallucinogenic Twilight Sleep drugs of scopolamine mixed with narcotics
Throughout the 20th century in America, and now into the 21st century, the male-orientation of the obstetrical profession has systematically disadvantaged childbearing women.
This also has a negative influence on their unborn and newborn babies (50% of whom are male), their husbands, other domestic partners, older children and their entire extended family. This is especially devastating when iatrogenic or nosocomial factors result in the preventable death of a new mother.
If she is married, her husband is widowed and her children left without a mother. When the deceased mother is the single head-of-household, her newborn infant and the older children will be orphaned.
A Riddle: What do American Tobacco Companies and our current hospital-based, technologically-enhanced obstetrical system have in common?
Obviously, this issue is light years away from the health-damaging issue of cigarette smoking, but unfortunately, there are disturbing similarities in the behaviour of the tobacco companies and those of the public response of the obstetrical profession, which is to say decades of denial in the face of overwhelming scientific evidence of harm.
Both of these entities — tobacco companies AND our current hospital-based obstetrical system — enjoy enormous economic gains from perpetuating the status quo
Both sell something — a produce or a service — to healthy people that is dangerous and in many instances results in life-threatening ‘complications’ and even death
Both have historically maintained that what they sold (cigarettes) or the services they provided (high-medicalized, high-tech obstetrical care) were either beneficial or benign
What both have in common is that business decisions made by them result in unnecessary illness and preventable death in formally healthy people, and does so at great personal cost to American families and economic costs to society that are NOT being reimbursed by either of these entities.
It’s time to make different choices, so where do we begin?
As outlined in this Mayday! series, thousands and thousands of smart, dedicated people have tried to fix these problems over the last 75 years. This includes dozens of grassroots activists, professional organizations of nurses, midwives, childbirth educators and historical advocates for normal childbirth like Childbirth Connection (formally known as the Maternity Care Association of NYC).
 So far, none of these activists groups has been able to fundamentally change the way obstetrics is practiced in America — that is to say, as a surgical speciality that routinely services a population of healthy women by applying a model of highly-medicalized, interventive, invasive and a technologically-centric care originally developed to treat high-risk pregnancies and serious complications, but since the introduction of EFM in the early 1970s, has been defined as the universal standard of care for ALL women, including the 70-80% of the childbearing population that are healthy and have normal pregnancies.
So far, none of these activists groups has been able to fundamentally change the way obstetrics is practiced in America — that is to say, as a surgical speciality that routinely services a population of healthy women by applying a model of highly-medicalized, interventive, invasive and a technologically-centric care originally developed to treat high-risk pregnancies and serious complications, but since the introduction of EFM in the early 1970s, has been defined as the universal standard of care for ALL women, including the 70-80% of the childbearing population that are healthy and have normal pregnancies.
What is wrong with this picture? Plenty!
 Healthy low-risk women and their healthy unborn and newborn babies:
Healthy low-risk women and their healthy unborn and newborn babies:
(a) don’t benefit from the routine use of c-EFM and many other routine interventions such as elective induction of labor
(b) Suffer harm related to biologically unnecessary medical treatment (iatrogenic) and (hospital-related) complications (nosocomial), in particular, those associated with the higher C-section rate that resulted from mechanical error, misleading or misinterpreted EFM monitor strips.
 (c) The well–documented and unambiguous direct cause-and-effect relationship between the use of continuous EFM during labor and increased rate of Cesarean surgeries.
(c) The well–documented and unambiguous direct cause-and-effect relationship between the use of continuous EFM during labor and increased rate of Cesarean surgeries.
This introduces unnecessary and unnatural risks associated with the many complications during and after the surgery, which in turn result in serious maternal morbidity and increased mortality without any offsetting benefit to these mothers, their babies or to society.
Action Plan Starts Here
While earlier political activities have been unable to correct the inappropriate obstetrical standard of care used in the US for healthy women with low-risk pregnancies, I believe there is a successful strategy that has not yet been proposed which will actually work.
It is simple and straightforward, will not increase the cost of maternity care but will dramatically reduce the C-section rate and its associated complications. This will in turn reduce the costs for health insurance companies and the federal MediCaid program.
The goal and plan is to rehabilitate the provision of maternity care in America so that healthy women with normal low-risk pregnancies are not treated as if they were high-risk.
Obviously, this will requires legal and legislative action.
This Mayday series is making the following 3 proposals:
 1. That fully-informed patient consent be legally required so healthy low-risk women with healthy pregnancies can make fact-based choices about the kind of maternity care that best suits them.
1. That fully-informed patient consent be legally required so healthy low-risk women with healthy pregnancies can make fact-based choices about the kind of maternity care that best suits them.
This would naturally include specific information about the two very different methods — auscultation and continuous EFM — for monitoring the well-being of their fetus during labor. This would also include other obstetrical policies, protocols and procedures that might be recommend to them during their pregnancy or labor, such as routinely recommending induction on or before the woman’s due date.
This information must acknowledge the inability of c-EFM to improved perinatal outcomes in low-risk pregnancies, and increased risk to the childbearing women directly associated with the statistically-significant increase in Cesareans (and their inevitable complications) relative to the routine use of c-EFM on healthy low-risk women.
It also must acknowledge additional increased risk — over and above the normal bedside electronica fetal monitoring — in hospitals that use a central monitoring system.
2. Embarking on public information campaign that includes investigative journalism from organization such as Propublica, PBS and NRP
3. Requiring manufacturers and distributors of continuous EFM devices to acknowledge their legal “Duty to Warn“. This must include a product disclaimer printed in the technical manual shipped with each electronic fetal monitor machine that reports the published findings of scientific studies over the last 49 years.
The consensus of the scientific literature has unambiguously established c-EFM as ineffective at reducing the incidence of cerebral palsy and similar neonatal encephalopathies (i.e. neurological problems).
In addition, the routine use of c-EFM is medical inappropriate during the labors of healthy low-risk laboring women, as it increases the cost of care, the rate of Cesarean surgeries (with its associated increase in risks and complications) without any correlating benefit to the mother or baby.
Last but not least, is an additional “Duty to Warn” by the manufacturers of central EFM systems (CMS). Developers and manufacturers of the CMS most also acknowledge the scientifically-established fact that central EFM systems currently being used in hospital L&D units have an even higher C-section rate than the hospital’s standard use of c-EFM in which an L&D nurse is personally responsible for ‘monitoring’ the fetal monitor strip in real time.
Exploring these actions:
 I. Lack of fully informed consent: The obstetrical profession must acknowledge and communicate to childbearing women under their care the negative aspects of the highly-medicalized, often invasive obstetrical standard of care as routinely applied to healthy childbearing women in the US.
I. Lack of fully informed consent: The obstetrical profession must acknowledge and communicate to childbearing women under their care the negative aspects of the highly-medicalized, often invasive obstetrical standard of care as routinely applied to healthy childbearing women in the US.
This includes (but is not exclusive to) the following topics:
- Highly-medicalized management of normal labor and birth in a hospital setting associated with increased risks of iatrogenic and nosocomial complications
- Information on the document ineffectiveness of continuous EFM at reducing the rate of cerebral palsy & newborn encephalopathies when used routinely on healthy, low-risk mothers-to-be
- Well-know risks associated with the routine use of Pitocin to speed up (augment) normal labors and the subset of procedures associated with the use of Pitocin during labor:
- mandatory use of continuous EFM whenever Pitocin is being given
- immobilization of the mother in her hospital bed
- use of intravenous fluids (IVs) over many hours or even day, which can overload the laboring woman’s circulatory system and increase likelihood of cardiac problems
- increased need for epidural anesthesia
- automatic blood pressure monitor on her upper arm and pulse-oximeter on her finger
- repeated bladder catheterizations and/or indwelling Foley catheter
- oxygen administered by face mask to anytime the nursing staff is worried about data on the EFM strip
- Induction, including side-effects of prostaglandin gel (Prepadil & Cervidil, etc) for cervical ripening, misoprostol (Cytotec) for inducing labor and the need to use of Pitocin IV to pharmaceutically advance an artificially induced labor and associated need for epidural anesthesia and other known and unknown risks associated with induction and Pitocin augmentation
- Substantially-increased risk of unnecessary and unplanned C-section in hospitals that have central EFM monitoring systems, which are documented to have an even higher rate of CS than c-EFM attended in the laboring woman’s room by L&D nurses, midwives, residents and attending physicians.
Economic Realities of c-EFM and other medically inappropriate obstetrical interventions
The unproductive expenses for society associated with ineffective obstetrical policies and protocols result in increased level of medically-unnecessary Cesareans and all related complications. This includes higher insurance premiums for individuals and employers and higher taxes for everyone to support the federal Medicaid programs reimbursement of hospitals and obstetricians for.
- In addition is lost wages for families associated with longer hospital stays, re-hospitalization and longer recovery time for the new mother.
- Social crisis resulting from high maternal mortality associated with continuous use of EFM on healthy women during labor and its associated higher rate of Cesarean surgery and its immediate, delayed and downstream complications.

The disproportionate burden that lack of fully informed consent relative to the current highly-medicalized obstetrical standard places on low-socio-economic women, women of color, those in same-sex relationships and other LGBT individuals.
When women of color, or as members of an ethnic minority receive prenatal care or are hospitalized during labor, they are even less likely to be fully informed about the risks of obstetrical interventions and invasive procedures before they are performed on them (without their fully informed consent) than middle and upper-class and non-ethnic patients.
This often triggers a cascade of events that negatively impacts their newborns (i.e. admission to NICU), reduces the likelihood that breastfeeding will be successful and will create an economic crisis for the family when the post-Cesarean mother is unable to return to work within 6 weeks, which is when her pregnancy disability terminates.
 II. Investigative Journalism – ProPublica (a Work-N-Progress)
II. Investigative Journalism – ProPublica (a Work-N-Progress)

III. Legislative ~ Mandating fully informed consent & eliminating “physician preference”
The ensconced and pervasive effect of “physician preference” has been unacknowledged for more than a century when when it came to GYN surgery in the US. The misogynistic injustice perpetrated on women with a breast cancer diagnosis and pointed out by women activists continues to fuel the wrong use of continuous EFM and its associated increase in Cesarean rates and associated increase in maternal mortality.
We need to legislation that officially eliminates the pervasive idea of “physician preference” is a professional privilege accorded to all MDs. That means that your doctor is free to make treatment decisions based on what he personally prefers or thinks is the ‘better’ option.
Just one of many historic examples were gynecological surgeons that routinely performed radical mastectomies without ever discussing other non-radical but scientifically effective options with the patient and her family. For more than a century, obstetricians in the US routinely induced labors in women who had not medical indication, and likewise scheduled elective Cesareans just because the doctor preferred this option or was going on vacation and wanted to get all his patients delivered before leaving town.
Other options included a simple surgery often described as a “lump-ectomy”, partial mastectomy or surgical techniques that favored reconstructive surgery such leaving the nipple in place when it was not adjacent to or in close proximity to the tumor.
Due to a consumer protection legislation passed by the California Legislature, all surgeons who treat breast cancer are now required by law to provide breast cancer patients a California DCA’s issued pamphlet that fully informs women dx with a malignant breast tumor of this full range of options.

We are seeking the same type of full information in standardized form as a state-mandated pamphlet relative to the routine use of an expensive and yet ineffective medical device known as continuous EFM on healthy women with normal term pregnancies as the obstetrical standard of care and the well-documented increase in Cesarean surgeries associated with the use of c-EFM in normal labors
These Cesarean-related complications include:
- Intra-operative and immediate complications: drug or anesthesia reactions, hemorrhage, shock, peripartum emergency hysterectomy (13 Xs higher rate following CS than vaginal birth) that requires days or weeks in the ICU
- Post-op complication requiring a post-Cesarean mothers to be treated for an infection following her surgery
- Inability to establish or maintain breastfeeding when new mothers have to be re-admitted to the hospital with a drug-resistant infection the requires a week or more of IV antibiotics
- Delayed complications in previous-Cesarean mothers who develops a placenta accreta or increta in a subsequent pregnancy that is so extensive a Cesarean-hysterectomy is required
- Downstream complications in which previous-Cesarean mothers finds themselves to be one of the unlucky 7 to 10% of placenta percreta patients that, in spite of being care for in one of the best hospitals with the best doctors, blood banking and best of modern medical and technological equipment, dies from a massive and uncontrollable hemorrhage
- Rare long-term complication a post-Cesarean mother dies months later from post-op complications such as a necrotic bowel caused by adhesions that develop due to her Cesarean surgery
- Secondary infertility when post-Cesarean women finds they are no longer able to get pregnant due to a post-Cesarean surgery infection that scared their fallopian tubes
- Maternal death due to an intra-operative, post-operative, delayed or downstream complication of her most-often medically UNNECESSARY C-section
- Impact on Spouse and other family members — maternal death makes her husband or partner into a widower and leaves their children without a mother.

Special high-tech OR & Invasive Radiology operating room and staff of 20+ for performing Cesarean-hysterectomies on previous-CS women with a placenta percreta (probably in Houston, which has a regional percreta center that serves Tx and surrounding states)
IV. Legal Strategy ~ Manufacturers’ Duty to Warn & Product Disclaimer on EFM equipment
This legal strategy would begin by producing a legal document to informed all American manufacturers and distributors of continuous EFM devices that they have a legal “Duty to Warn”, and thus required to include a product disclaimer.
This would need to report the consensus of scientific studies and other forms of research conducted over the last 50 years, which has unambiguously documented that healthy laboring women with normal low-risk pregnancies do NOT benefit from the routine use of continuous EFM as defined by a reduction in the rate of CP and other neonatal encephalopathies, while this same demographic of c-EFM laboring women bear a significant increase in unplanned Cesareans deliveries and their sequela.
In addition, the manufacturers of central EFM systems (CMS) have a further “Duty to Warn” over and above the standard bedside use of c-EFM. Developers and manufacturers of the CMS must acknowledge the scientifically-established fact that central EFM systems currently used in hospital L&D units have an even higher C-section rate than the hospital’s standard use of c-EFM in which an L&D nurse is personally responsible for ‘monitoring’ the fetal monitor strip in real time at the laboring woman’s bedside.
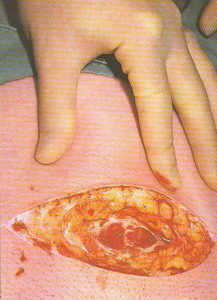
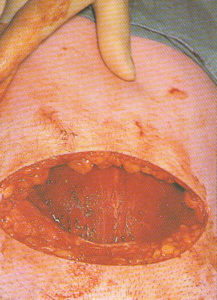
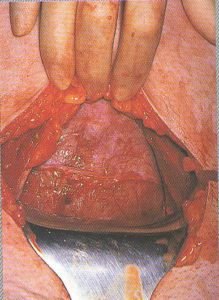
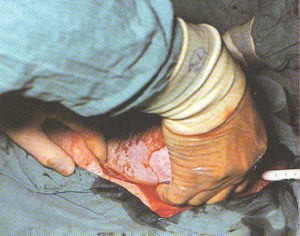
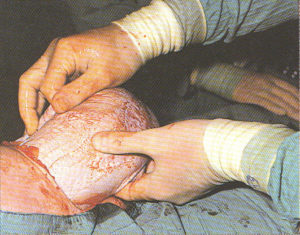
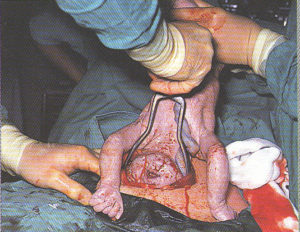
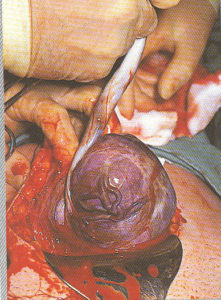
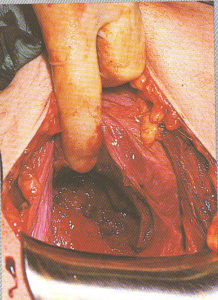
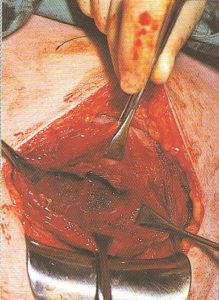
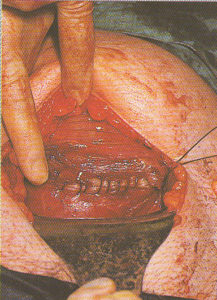
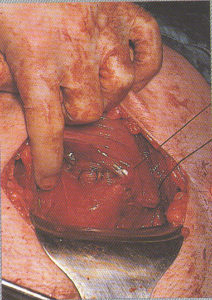
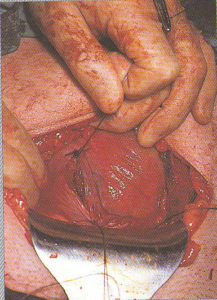
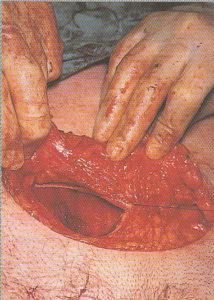
Step-by-step photos of Cesarean surgery
Incision, delivery of baby, removal of placenta and suturing
the 7 layers of bodily tissue from surface skin to the mother’s uterus
|
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
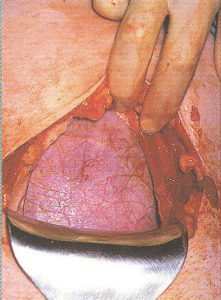
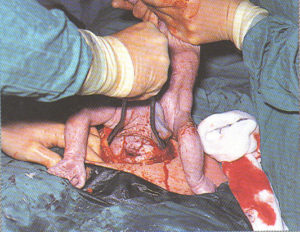
Externalization of the uterus
After the baby is delivered, many OB surgeons lift the uterus
out of the new mother’s abdominal cavity and
lay it on top of the her’s abdomen.
This makes it easier for the surgeon
to see what they are doing while
suturing the uterine incision.
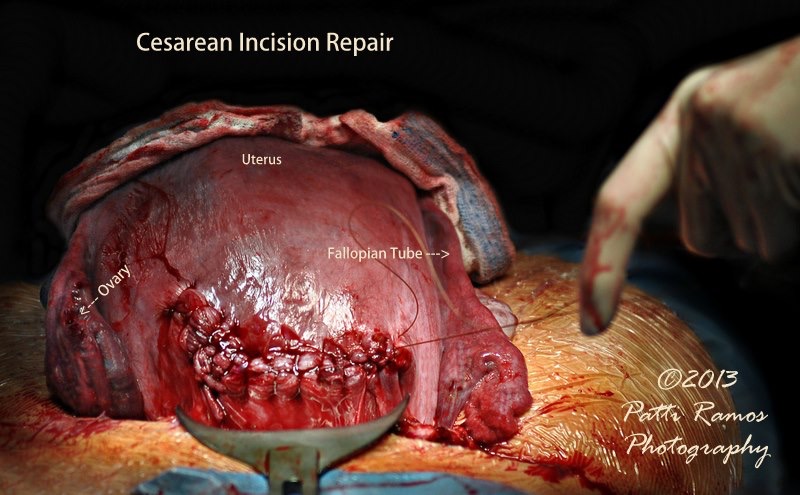
Suturing of the Cesarean incision, using a popular technique in which the uterus is lifted up out of the mother’s abdomen and as an externalized organ, is set on her abdominal wall so the surgeon can see better and be in a better situation for suturing the uterine incision
Connecting Up the Dots: Additional chapter are Work-N-Progress ~

Stay tuned!
Over the next week or two, I’ll be posting background information about how EFM became the standard of care, how the hospital-obstetrical- department financial deal works and other critical pieces of the puzzle.
