Text from Huffington Post — photos added
LINK to original post –> http://www.huffingtonpost.com/entry/the-global-epidemic-of-unneeded-cesarean-sections-its_us_590935eee4b05279d4edc0eb

Some women choose elective cesarean surgery, but it should be noted that as the new mother, she (the woman herself) is virtually (and realistically) erased from the picture. Cesarean section of something done by doctors on the inert body of the mother-2-be.
Ask anyone, as I have, in a range of health care and academic settings: why are Cesarean section (C-section) rates so high in middle- and high-income countries? You’re likely to hear that “women demand it.”
It turns out that this is absolutely not the case. In study after study, women indicate that they want what’s best for them and their babies, and mostly want a C-section only if it’s medically indicated.
According to the World Health Organization (WHO), there is no benefit to mother or baby if the average C-section rate is higher than 10 percent for any given country, and overall, you are likely to see worse outcomes for babies as rates climb over 20 percent. And the WHO has laid out very clearly who should be considered for C-section and who should not.
To answer those questions, it’s helpful to look at which countries have the lowest and highest rates. Low-income countries have low rates because they just don’t have the resources — trained medical staff, operating rooms — to provide life-saving C-sections when needed. The countries with the most evolved health systems — mostly those in northern Europe — have the lowest rates, but even there, none are below the WHO-recommended 15 percent threshold.
The most shocking data on C-section rates come from countries that are in the middle-income category. Countries with average C-section rates above 40 percent include China, Mexico, Iran, Brazil, Turkey, Egypt, and the Dominican Republic. And within low- and middle-income countries, C-sections are often determined by economic status: as was described in a recent Lancet article, mothers with low incomes get “too little too late” from the public sector, and those with higher incomes get “too much too soon” in the private sector.

The true reasons for the high C-section rates are more complex. Birth is a natural event that usually can be supported to a good outcome without surgery, yet labor wards generally give low priority to enhancing women’s own abilities to give birth; instead, we over-medicalize care around birth and promote interventions that make C-sections more likely.
C-sections are promoted as “routine,” while their side effects and implications for future deliveries are understated.
Unquestionably, the deck is stacked against natural delivery. In many health systems, there is a financial incentive for physicians to recommend C-sections rather than natural delivery. Elective C-sections also allow providers to avoid the lifestyle disruption of attending to natural deliveries that occur at all hours of day and night.

Breech extraction via Cesarean
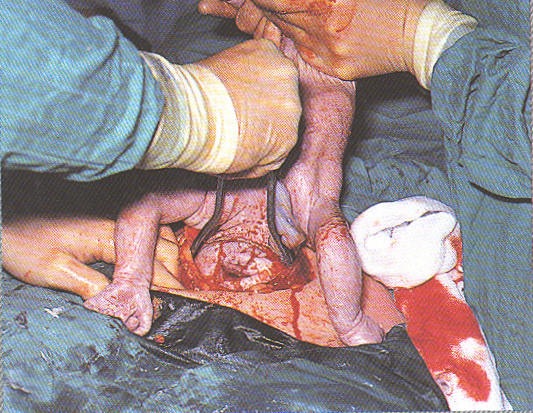
Cesarean forceps delivery for after-coming head of breech baby
Brazil is attempting to show that it’s possible to do the right thing and reverse decades of sharp increase in C-section rates.
Brazil sits atop the countries with the highest C-section rates: 85 percent of deliveries in the private care system and 45 percent in the public system. Many obstetric units in Brazil have never seen a natural delivery, and many obstetricians have never delivered a baby without C-section.
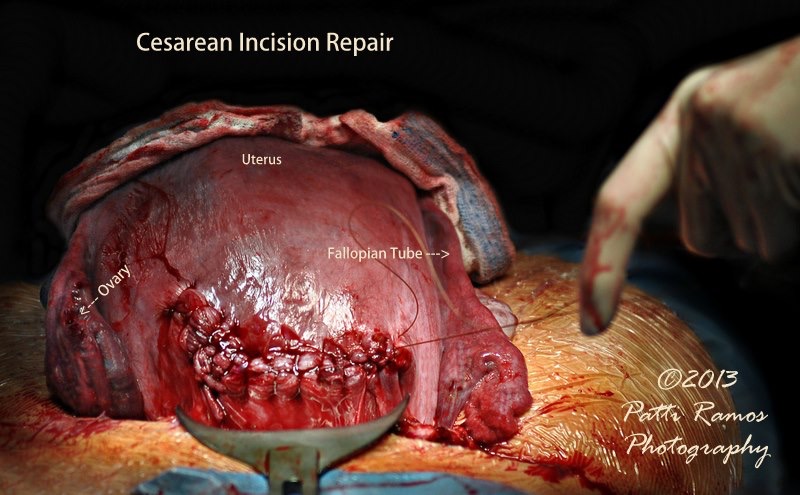
After the baby is removed from the mother’s uterus, a common surgical practice used in the US is to ‘externalized’ the uterus — lift it thru the incision and lay it on the outside of the mother’s abdomen while the surgeon is suturing the organ. This is why it is possible to see the entire uterus and fallopian tubes.
Moving from a norm of surgical intervention to a norm of natural delivery requires a massive culture shift and a major system redesign. Many stakeholders — hospitals, regulators, insurers, providers, health system administrators, and mothers — have assembled a coalition to try to achieve exactly this ambitious aim.
Using a health systems redesign and quality improvement approach pioneered by the Institute for Healthcare Improvement, 150 hospitals in the private and public sectors are gathering in Sao Paulo this week to learn from a trailblazing group of 26 hospitals who showed it was possible to make a major dent in C-section rates in a short period of time.
Led by a team from the Albert Einstein Hospital, clinicians were re-trained in natural childbirth, worked in teams, created an environment of care that promotes natural childbirth, and empowered women to clearly state their wishes.

Over 18 months, these 26 hospitals have doubled their rates of natural delivery. They still have a long way to go — average C-section rates dropped from about 80 to 60 percent — but this gathering of 150 hospitals promises to reverse a 30-year trend of relentless increases in C-section rates.
There is much yet to do around the world. In low-income countries, women are dying from lack of lifesaving C-sections, while in middle and high-income countries, C-sections are often used as a shortcut for personal or institutional profit or care provider convenience.
Ultimately, for every mother and newborn, there is a “right” care response that may result in a natural delivery or C-section as part of a safe birth. Brazil’s experiments with new natural delivery designs are leading the way for countries across the world where many C-sections are not the right response.
 |
 |
 |
