 There is an ethical contradiction inherent in the current practice of obstetrics in the United States, a unique ethical dilemma that affects all Americans.
There is an ethical contradiction inherent in the current practice of obstetrics in the United States, a unique ethical dilemma that affects all Americans.
It concerns all of us, even if we, or one of our own family members, is not expecting a baby any time soon.
But first, what we are & what we are NOT saying:
This plea for common sense is not an indiscriminate rant about the obstetrical profession. No one, least of all me as a former labor and delivery room nurse for 15 years, is questioning the life-saving ability of modern obstetric medicine for women with high-risk pregnancies or those who develop serious complications during labor.
In fact, we are uniformly grateful that skilled obstetricians and high-tech obstetrical services are readily available to those whose lives and well-being depend on such interventions.
But currently, the noble humanitarian goals of obstetrics are not being realized for the healthy 70 to 85% of the childbearing population. This is not an inconsequential issue, either in the number of families affected (approx. 3 million every year), the expense in scarce but precious healthcare dollars, or the impacts on the lives of women, their babies, their families, and society.
 In the United States, healthy low-risk laboring women are being subjected to the routine use of a system for fetal monitoring during labor that does not improve the outcomes for themselves or their babies when compared to the time-tested and proven method of routinely monitoring the well-being of a fetus during labor with either a special stethoscope (fetoscope) or a hand-held Doppler.
In the United States, healthy low-risk laboring women are being subjected to the routine use of a system for fetal monitoring during labor that does not improve the outcomes for themselves or their babies when compared to the time-tested and proven method of routinely monitoring the well-being of a fetus during labor with either a special stethoscope (fetoscope) or a hand-held Doppler.
 Rigorous scientific research has repeatedly documented that the low-tech, high-touch, one-on-one method known as auscultation is as effective an electronic monitoring machine, with the added benefits that auscultation does NOT increase the C-section rate, while c-EFM does.
Rigorous scientific research has repeatedly documented that the low-tech, high-touch, one-on-one method known as auscultation is as effective an electronic monitoring machine, with the added benefits that auscultation does NOT increase the C-section rate, while c-EFM does.
The facts are crystal clear — the routine use of continuous electronic fetal monitoring (c-EFM) on healthy, low-risk women, as compared to regularly scheduled hands-on listening with a Doppler by the L&D nurse or midwife, revealed NO reduction in the rate of cerebral palsy and similar neurological problems in newborns.
Understanding the legal theory behind these facts
An important Supreme Court ruling by Justice Brennen made a legal distinction that is helpful in understanding this issue. Justice Brennen’s ruling noted that it was illogical to treat two different things as if they were the same, and equally illogical is to treat two of the same things as if they were different.
Based on this distinction, the current use of c-EFM is illogical, as it treats two very different groups as if they are the same. In other words, healthy childbearing women with normal low-risk pregnancies are being treated the same as women with high-risk pregnancies or other situations that put their fetuses at great risk.
Because c-EFM is appropriate in high-risk situation does NOT make it appropriate for women who are do not have a high-risk pregnancy and are not suffering from other complications that are uniquely risky for their unborn babies.
EFM is not the “Buckle-up for Safety” device
its promoters claim
 Hospitals and the obstetrical profession treat c-EFM as the central source of safety in childbirth, the way seat belts are seen as the universal answer to automobile safety.
Hospitals and the obstetrical profession treat c-EFM as the central source of safety in childbirth, the way seat belts are seen as the universal answer to automobile safety.
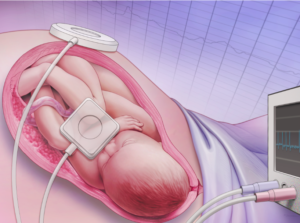
From this buckle up for safety perspective, the two EFM straps that go around the mother’s abdomen and plug into a computerized EFM machine is the obstetrical version of mothers-to-be wearing their seatbelt during labor. Just as we expect new parents to put their newborn in an infant car seat for the trip home from the hospital and buckle their own seat belts, we likewise see EFM belts as able to keep healthy baby safe during labor and birth.
But give the indisputable facts communicated in hundreds of studies and randomized controlled trials, the idea that 2 EFM straps encircling the pregnant abdomen of low-risk women ever minute of their labor is the height of craziness!
The facts are immutable and indisputable
The current system treats all healthy women with normal pregnancies as if they were high-risk. More to the point, it does this without improving outcomes for babies and while increasing medically-unnecessary surgical deliveries, and its many complications, including increased maternal mortality and morbidity.
That hospital corporations and individual obstetricians believe continuous EFM will help to defend them in case of a malpractice suit also does not make its use appropriate, unless institutions or practitioners first obtain informed consent that identifies the primary effect of EFM to be a risk-management strategy for protecting the hospital or obstetrical attendant.
This informed consent must include the information cited above — that the healthy baby of a healthy pregnant woman with a normal term pregnancy does NOT benefit from c-EFM. The same continuous electronic monitoring system that protects the obstetrician and hospital is simultaneously exposing the baby’s mother to the life-threatening risks associated with the increased rate of Cesarean deliveries when c-EFM is used during labor .
C-EFM: The Crux of the Obstetrical Profession’s Ethical Dilemma
 The crux of the ethical contradiction I referred to earlier is obstetrical profession’s practice of using an expensive technology designed to help the unborn babies of women with high risk pregnancies and applying this technology universally to women who are low-risk. While there are many health and safety aspect of this ethical dilemma, one the most important to society is an economic issue known “value added”.
The crux of the ethical contradiction I referred to earlier is obstetrical profession’s practice of using an expensive technology designed to help the unborn babies of women with high risk pregnancies and applying this technology universally to women who are low-risk. While there are many health and safety aspect of this ethical dilemma, one the most important to society is an economic issue known “value added”.
The Economic Principle of “Value Added” — failed policy for the public or bonanza for hospitals as money-making businesses?
The economic principle of ‘value-added’ describes paying an additional amount of money in order to get goods or services that are substantially BETTER (and definitely NOT worse) than it would been without the added goods or services. The obstetrical profession and hospital corporations would like us to believe that its policies and protocols and the many intervention routinely used during normal labor and birth — especially the use of continuous EFM — adds substantial ‘value’ by substantially contributing to the safety of both mother and baby.
Unfortunately for healthy women with normal low-risk pregnancies, c-EFM is value subtracted!
Real “Value Added” ~ Scientific evidence that properly restricts the use of EFM to very high-risk patients
The logical step at this point is to end all obstetrical protocols in American hospitals that make the universal use of c-EFM the standard of care for all laboring women. This represents 70-80% of healthy pregnant women at term. In place of the ineffective and often harmful policy of universal EFM, this new standard must include two very specific and dramatic changes.
Transparency: Healthy women with normal pregnancies need to be fully informed about the ineffectiveness of c-EFM when used on a low-risk population. Informed consent prior to the use of c-EFM must also identify the mother’s increased risk of having an unnecessary emergency CS during labor, with all the risks of complications associated with Cesarean surgery.

“Obstetrical department staff sitting at desks to monitor banks of electronic fetal monitors”
The hazards associated with EFM, both at the bedside and for central electronic monitoring systems need to become common knowledge. This is true whether electronic monitoring is done at the bedside or uses a centralized monitoring system. Hospitals using a central monitoring system have an even greater increase in C-sections than bedside EFM. Bedside monitoring has the advantage (one hopes!) of the L&D nurse or midwife coming into the room much more frequently to check both the fetal monitor printout AND the laboring woman.
I want to note that central EFM monitoring, while being even more “high tech”, is NOT better or safer! It means L&D nurses, doctors and midwives are all sitting out in the hallway at a long desk watching EFM monitoring screens instead of being in the room with the laboring patient. The result is a significantly greater number of Cesareans per 100 deliveries when compared to hospitals what use bedside EFM.
Second, the use of EFM must be replaced by auscultation as the appropriate standard of care for healthy women with normal low-risk pregnancies and spontaneous onset of labor.
When compared to vaginal birth, how much riskier is Cesarean delivery?
 In 2004, a maternity nurse advocacy group — the Maternity Center Association of NYC started in 1918 but now known as the Childbirth Connection (see hx & info at end of post) published a 28-page booklet entitled “What Every Pregnant Woman Needs to Know About Cesarean Section”
In 2004, a maternity nurse advocacy group — the Maternity Center Association of NYC started in 1918 but now known as the Childbirth Connection (see hx & info at end of post) published a 28-page booklet entitled “What Every Pregnant Woman Needs to Know About Cesarean Section”
Cesarean Risks: In the section that identifies increased complications known to be associated Cesarean delivery, it lists 25 risks for the childbearing woman that are unique to C-section, starting with its increased rate of maternal death. It also lists 9 unique risks for newborns born by C-section, including accidental scalpel lacerations of the unborn baby that occur when making the incision into the mother’s abdomen, and prematurity due to an error in dating the pregnancy.
 Vaginal Birth Risks: Under the section listing risks unique to vaginal birth (i.e. problems or complication NOT also associated with Cesarean delivery), it lists 3 risks for mothers (starting with painful vaginal area) and 1 for the newborn.
Vaginal Birth Risks: Under the section listing risks unique to vaginal birth (i.e. problems or complication NOT also associated with Cesarean delivery), it lists 3 risks for mothers (starting with painful vaginal area) and 1 for the newborn.
As detailed in the MCA’s fold-out, the increased danger of Cesarean does not end with the surgical delivery. This makes Cesarean one of those negative ‘gifts’ that keep on giving, since a certain set of risks are carried into the future. These are complications that trace back to the previous-Cesarean into future pregnancies that affect both the childbearing woman and her unborn or newborn baby.
In addition to the standard intra-operative complications (ex. excessive bleeding, medical errors) that are immediate, there are also delayed and downstream consequences of previous Cesarean surgery. These include an increased rate of serious morbidity (complications and prolonged or permanent disability) and maternal death.
This list includes a 6% secondary infertility rate (unable to get pregnant again after a CS due to post-operative infection), a 13-fold increase in emergency hysterectomies during or within 14 days of delivery, dramatic jump in abnormal placental implantation in subsequent pregnancies. This placental complication is associated with a 7%-to-10% maternal mortality due to intraoperative hemorrhage or post-op infection in women diagnosed with a placenta accreta or percreta that required a Cesarean hysterectomy to deliver their next baby.

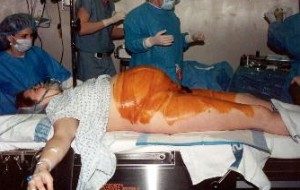
Regional surgical center in SE that specializes in performing Cesarean hysterectomies on pregnant women diagnosed with placenta percreta. Note super-sized operating room with specialized equipment incl interventional X-ray machine and at least 20 specialized hospital staff. The cost of an operation like this approaches and may even supercede organ transplant. Note how the mother herself has all but disappeared from the scene as surgeons suture the incision in her abdomen, and her baby lays by itself in the specialized neonatal crip surrounded by NICU nurses and the neonatologist.
“One picture is worth a thousand words“
The photograph above exposes the reality associated with the routine use of EFM in the US and subsequent spike in CS, which results in a host of delayed and downstream complication that are extremely expensive to the healthcare system while being extremely profitable to doctors and hospitals. This situation is the polar opposite of “value added”, unless you are describing the cascade of additional “billable units” that come with having a 33% Cesarean rate, and then with treating the 33 additional Cesarean-related complications that it spawns.
At least one obstetrician has honestly acknowledge that the most dangerous thing about Cesarean deliveries are the “repeat Cesareans”. Post-Cesarean pregnancies have a statistically significant increase in intra-operative hemorrhage, placenta accreta/percreta and increased need to perform Cesarean hysterectomies and peri-partal hysterectomies. Maternal mortality is MORE likely in a repeat C-section than in the first Cesarean surgery.
In light of the greatly increased need for medical and surgical interventions in prior Cesarean women, and subsequently increased need for much more expense hospital care and invasive procedures, the “value added” by the greatly liberalized, often ‘elective’ use of Cesarean delivery is a great deal of additional profit to hospitals.
The hospital industrial complex has created its own revenue stream — a kind of a perpetual motion machine for printing money by routinely dispensing a model of highly medicalized so-called “normal childbirth” services. This kind of care begins by hooking the newly admitted mother up to a continuous monitoring machine, and end in unexpected Cesarean surgery about 31% of the time, followed by “repeat” Cesareans 87% of the time,
Like the surgical error of taking out the healthy kidney (instead of the diseased one), invasive obstetrical also creates a hospital-dependent population of childbearing women that have to return again and again to the same or a different hospital for expensive care made necessary by the over zealous obstetrical intervention (c-EFM) that resulted in the first medically unnecessary Cesarean surgery.
As a result, hospital OB department perpetuate an endless stream of future patients who were told they had to have a repeat Cesarean, or has such a nightmare labor the last time (ex. two-day Pitocin induction) or the honestly but erroneously believed that a repeat Cesarean was much safer than a vaginal birth after a previous Cesarean (VBAC).
 Biographical Note on the Maternity Center Assoc/ChildbirthConnection.org
Biographical Note on the Maternity Center Assoc/ChildbirthConnection.org