 Faith Gibson
Faith Gibson
California Licensed Midwife 041

February 2025 ~
Part 1-a ~ word count: 2117 reading time approximately 15 minutes
History of the word “midwifery”
The word “midwifery” comes from 16th century Middle English. It simply meant “with-woman” in relation to childbearing. In the narrowest sense, any woman who stays with and helps another woman during the childbearing process is providing midwifery care as a verb (but not as a noun or formal title).
 The term “man-midwife” historically referred to male doctors who regularly attended “cases of childbirth”.
The term “man-midwife” historically referred to male doctors who regularly attended “cases of childbirth”.
Formally, midwifery is defined as: “skilled, knowledgeable and compassionate care for childbearing women, newborn infants and families across the continuum from pregnancy, birth, postpartum and the early weeks of life.”
According to research by paleontologists, the modern birth canal in Homo-sapiens evolved 200,000 years ago. Since that time, our homo-sapiens species has apparently been actively managing childbirth as an aspect of gender-based care. Older and more experienced women who had experienced giving birth themselves assisted younger women giving birth for the first time. It is highly likely that women with childbirth experience also provided a helpful social and practical presence to women having additional babies.
Only one group of our ancient ancestors was identified as managing childbirth by sending the laboring girl or women out into the surrounding wilderness to give birth alone or die trying. It’s highly likely that this heartless branch of the homo-sapiens species was unable to propagate in sufficient number to make it into the modern gene pool.
Childbirth ~ a topic not fit for polite society
Childbirth, midwifery, and obstetrics are not very interesting topics for most adults, even though three million adolescent girls, wives, and mothers gave birth each year during the 20th century. That’s approximately 300 million births, or a tiny tad less than the current population of the United States, which is right now is 335 million. But if women stopped having babies, our country would eventually cease to exist. Clearly a safe and successful childbirth is very much in our national interest.
Even though the continuation of our species is 100% dependent on the success of female reproduction, very few of us homo-sapiens seem to have any personal interest in how our culture deals with childbirth – that is, does it support or ignore it?
Different cultures have very different relationships with the issue of childbearing women and childbirth. Some countries publicly ignore the issue altogether, apparently unbothered by a very large number of new mothers that die during or soon after childbirth and the many orphans they leave behind.
 Other countries wisely developed a “safety net” that was part of their national healthcare system. This generally includes access to maternity care for healthy childbearing women provided by professionally-trained midwives.
Other countries wisely developed a “safety net” that was part of their national healthcare system. This generally includes access to maternity care for healthy childbearing women provided by professionally-trained midwives.
This includes a collaborative arrangement between midwives and a local general practice physician. The GP physicians are able to provide backup medical care, as well as to initiate hospital transfer if there is a serious problem.
The majority of European countries provide maternity care to all its pregnant citizens, with professionally-trained midwives being the country’s primary birth attendants. A few years ago, the statistics for the UK identified 30,000, professionally trained midwives and 2,000 obstetricians who provide hospital-based services as needed. As a result of this supportive and responsive system, the maternal mortality rate in most European countries is two to four times lower than the MMR for the United States.
“The United States has the highest maternal mortality rate among high-income countries.” Commonwealth publication 2022
[Note-2-self –> provide a link to original Internet post]
Unlike the national maternity care programs in Canada, Japan, Australia, the EU, and most of the rest of the developed world, America has mostly turned a blind eye to the gender-based biology of reproduction, assuming that somehow giving birth and raising a family just isn’t very interesting or important.
 For 125, the US has had the very highest maternal mortality rate of all developed countries
For 125, the US has had the very highest maternal mortality rate of all developed countries
Since the earliest decade of the 20th century, the US has the highest MMR of all the wealthy countries in the world. What is it about the maternity care system in the United States that its outcomes are so different than other developed countries?
The US spends twice as much money on hospital-based obstetrical facilities and in-patient services than other wealthy countries. Obstetricians provide more than 90% of all childbirth-related services in our country since the beginning of the 20th century, and yet for the last 125 years, the US has consistently had the highest MMR of any comparably developed country.
In 1910, the number of new mothers in America that died per 100,000 births was 850. That is a death rate of one new mother dying for every 118 births. At this very same time, the number of new mothers in Sweden who died per 100,000 was only 230. That was only one death out of 435 births or 3.6 times safer than in the US!
Obviously, all developed countries have reduced the maternal mortality rate by many orders of magnitude when compared to the 1910.
The United States, which prides itself as having the best everything, has had the very highest rate of maternal deaths of all industrialized countries since 1910.
But today, and for the last 125 years, the US has been in last place for wealthy industrialized countries when it comes to preventing unnecessary maternal deaths.
Currently, the maternal death rate in the United States of America is 20.1 per 100,000. According to the Index Mundi, the US is in the 128th place worldwide:
| 123 | Romania | 19 | |
| 124 | Oman | 19 | |
| 125 | Latvia | 19 | |
| 126 | Moldova | 19 | |
| 127 | Ukraine | 19 | |
| 128 | United States |
19 |
|
| 129 | Turkey | 17 | |
| 130 | Uruguay | 17 | |
| 131 | Tajikistan | 17 | |
| 132 | Saudi Arabia | 17 | |
| 133 | Russia | 17 |
American Childbearing women would be safer if they went to any of the following countries:
Turkey, Uruguay, Tajikistan, Saudi Arabia, Russia, Iran, Albania, Bahrain, Chile, Hungary, Kuwait, Korea-South, Kazakhstan, Canada, Bulgaria, Bosnia-Herzegovina, Estonia, Qatar, New Zealand, Portugal, and Croatia
Back to the big Question: Why should men and non-pregnant women care about the sky-high mortality rate in the United States?
 There are several reasons to care about the low quality of maternity care in America and resulting high rate of maternal deaths. The most important is simply that there is absolutely no good reason for these personal disasters.
There are several reasons to care about the low quality of maternity care in America and resulting high rate of maternal deaths. The most important is simply that there is absolutely no good reason for these personal disasters.
Healthy childbearing women do not “need” to die, and except for mortuaries and cemeteries, it certainly doesn’t do much for the economy.
But for every one maternal death, 70 laboring women had life-threatening complications during labor or birth, or within 42 days of giving birth. This may result in life-long disabilities for these new mothers.
Preventable illness or injury associated with childbearing is known as maternal “morbidity“. A great many of these complications were the direct result of routine obstetrical interventions, such as scheduled induction before the baby’s due date, based on the very dubious claim that it is ever so slightly “safer” for the unborn baby.
Unfortunately, when the obstetrical system routinely intervenes by doing medically unnecessary elective inductions, which has become the new “standard” adopted by many obstetricians and hospital OB departments, the length of time the mother-to-be spends lying in a hospital bed is greatly increased. This inevitably includes being hooked up to 6 or 7 or even more devices, IVs and electronic technologies that force her to stay in bed during the entire labor.
This is accompanied by a high level of drugs and medical interventions, almost always requiring the mother to be given epidural anesthesia. When the mother’s water (i.e. the amniotic sack) is broken in an attempt to start the labor but it doesn’t work, doctors often insist that the baby be delivered by unplanned Cesarean surgery to prevent infection.

Making elective induction before the baby’s due date into the new obstetrical “norm” in the US
According to two studies done a few years ago in Europe, the neonatal mortality rate for births that occurred before the mother’s official due date, there was a small statistical advantage for babies born during the 39th week of pregnancy. The mortality rate for babies born during the seven days prior to the mother’s due date was 4 per 1,000, compared to 7 per 1,000 for babies born during the seven days that started with the mother’s due date.
The study consisted of thousands of pregnant women, some of whom were very healthy, while others were not necessarily so healthy but didn’t have an officially diagnosed disease such as diabetes, anemia, hypertension, etc.
However, demographic studies this sort — numbers separated from the actual circumstances which are unknown to the statastition — do not include any personal information about the childbearing woman’s life circumstances, such as the levels of stress she was regularly exposed to, such as already being the mother of several children while living in small apartment with an alcoholic or abusive spouse, or a very difficult economic situation, such as being unemployed, living on the streets or in a homeless shelter.
Based on those two studies, the American obstetrical profession recommends that all healthy pregnant women with perfectly normal and healthy term (37+ weeks) pregnancy be electively hospitalized and induced during the week before their due date.
 As noted above, being born before the due date may or may not have a small advantage for the baby.
As noted above, being born before the due date may or may not have a small advantage for the baby.
But what we do know for sure is that induced labor before the childbearing woman’s body is ready to give birth spontaneously always has a very much longer and much more painful labor, accompanied by a long list of labor-related interventions and statistically greater likelihood of an unplanned Cesarean surgery during the labor.
 For the pregnant woman, being induced means a much longer time in the hospital labor room while lying in a hospital bed while hooked up to an impressive number of medical and electronic paraphernalia.
For the pregnant woman, being induced means a much longer time in the hospital labor room while lying in a hospital bed while hooked up to an impressive number of medical and electronic paraphernalia.
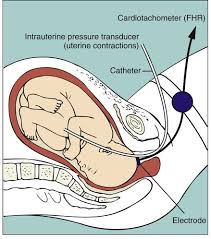
Being admitted to any hospital in America almost always (according to a Google search it’s 85% of the time) a continuous electronic fetal monitor, known to fans of the Monty Python movie “The Meaning of Life” as “the machine that goes ping” strapped around her abdomen.
Being induced means having a needle in your arm connected to a plastic tube that goes up to one or more IV bottles designed to constantly drip Pitocin (sometimes also a saline solution or D5W) into your bloodstream.
There will also be an automatic blood pressure on one arm that goes off without warning about every 15 minutes, and a pulse oximeter on one of her fingers that glows in a way that is reminiscent of the extraterrestrial from outer space in the movie: “ET Call Home”.
Lying in bed hour after hour while hooked up to all this medical equipment is so miserable for the most labor patients that pretty soon everyone — patient, spouse, L&D nurse and the OB doctor — will all agree that epidural anesthesia is needed to get the mother-to-be through the many long hours of being trapped in bed while being inducted.
The hospital anesthesiologist soon appeared in the room and put an epidural catheter in the laboring woman’s back, which made the patient numb from the waist down. The anesthesia pump would be hooked up to yet another IV pole that huddled together at the top of her hospital bed.
But unfortunately, a side effect of being anesthetized from nipples to the knees is that the mother can no longer feel her bladder, which also means she can’t urinate spontaneously. The nurse will need to put in an indwelling Foley catheter in her bladder that will silently drain urine into a plastic pouch attached to her hospital bed for the remainder of her labor.
Statistically she will be darn lucky if some spurious reading from the electronic fetal monitor — the second most frequent reason for doctors to do an emergency C-section on a first time mom during labor — or the doctor’s concern that she’s been pushing too long and “the baby maybe getting tired”.
Vacuuming the baby out when the mother gets too tired to push
The first thing obstetricians do under these circumstances is use an obstetrical device known as a “vacuum extractor”. It is somewhat reminiscent of a miniature toilet plunger – a 4-inch around rubber cap that is attached to the unborn baby’s scalp at one end, while the other end is connected to a small hand-pump.
When it is repeatedly pumped, the vacuum extractor creates a strong suction on the top of the baby’s head that allows the obstetrician to pull the unborn baby down farther down, until the doctor can get his or her hands on the baby and extract it from its mother’s body.
I was present at a hospital birth in which the doctor asked the nurse to go get a vacuum extractor, but the mother delivered quickly and it was never used. Since the package was opened, it was no longer technically “sterile”, which meant it would have been thrown in the waste basket. However, I asked one of the nurses if I could keep it to demonstrate to my childbirth classes how a vacuum extractor worked, so she let me take it.
Not long after, I demonstrated how vacuum extraction worked to our childbirth education class. I pressed the round rubber vacuum disk that is usually attached to the top of the unborn baby’s head against the palm of my left hand. I was surprised and pleased that it fit so perfectly. Then I stated pumping the handle that sucked the very small amount of room air between my hand that the rubberized fetal “disk”.
But I was soon horrified to see that the suction being created between the palm of my hand and the suction disk (which usually is attached to the unborn baby’s head) was so very strong that collapsed the bones in my left hand – the ones that ran between my wrist at one end and my fingers at the other. In essence the natural “dome” that would naturally be the back of my hand was sucked inward until it created a depression or a hollow pit, something like a shallow sink hole in lawn.
On that occasion, I concluded that it was wrong to believe that vacuum extraction was just a benign device — handy and yet “no big deal” from the standpoint of the baby’s head!
Instead I had another fact-based reason to insist that the “right use of gravity” is Mother Nature’s best gift to childbearing women, the best way to avoid the need to use medical and surgical instruments to ‘remove’ the baby from its mother’s body.
Pitocin, EFMs, and the hospital attorneys’ fear of litigation!
Whenever Pitocin is used to induce or speed up labor, electronic fetal monitoring is required by the hospital’s malpractice attorneys.
 If the baby goes into some kind of fetal distress and does poorly after its birth, lawyers hope the EFM tracing will be normal and therefore able to prove that it wasn’t the hospital or doctor’s fault.
If the baby goes into some kind of fetal distress and does poorly after its birth, lawyers hope the EFM tracing will be normal and therefore able to prove that it wasn’t the hospital or doctor’s fault.
Many of these same issues apply to the use of epidural anesthesia, which also obliterates the ability to make “right use of gravity” so not infrequently it results in additional obstetrical interventions such as Pitocin IV to make the labor more effective.
Unfortunately, when laboring women lie in bed for a protracted period of time, it sometimes triggers fetal distress and this usually means the baby will be delivered by emergency C-section.
As the “gift that keeps on giving”, a searching “Cesarean” on the Internet brings up pages of published studies that have identified 33 frequent complications and when unusual and rare complications are accounted for, there are more than 100 potential complications triggered by the Cesarean or its complications.
Complications inevitably require the use of more drugs, additional expensive and painful procedures, or surgery that often introduces new complications that so severe that the new mother is in the ICU for a month.
The gift that keeps on giving comes in three flavors
The complications from Cesarean surgery come in three different categories. Only 5 -to-10% of Cesarean surgeries are medically necessary to save the life of the mother or baby or both. The complications associated with Cesarean surgery or its sequelae days, weeks, months, or years later in three categories, which are”
(A) Immediate, (B) Delayed and (C) Downstream complications
I thank God that such a rescue operation and the obstetricians are very good at performing this surgery even in a very serious emergency.
However, two-thirds of all Cesarean were most likely not medically necessary; instead they were triggered by the use of unnecessary obstetrical intervention, many times based on the doctor or hospital’s fear of a malpractice lawsuit, in what would otherwise have been a normal vagianal birth for mother and baby.
 This lose-lose situation does NOT have to be the “business as usual” for childbearing families in America. No one wants the first month of their newborn’s life to be in the hospital nursery while their new mother is being treated for unexpected complications in the hospital’s ICU.
This lose-lose situation does NOT have to be the “business as usual” for childbearing families in America. No one wants the first month of their newborn’s life to be in the hospital nursery while their new mother is being treated for unexpected complications in the hospital’s ICU.
This foolish system has never been the “norm” in Japan, European countries and most other parts of the world. This not only wastes lives, but obstetrical interventions and their complications often cost a small fortune.
End of Part 1-a; will post a link to the part 1B after it is finished.
@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@
 Note to Self — move this unfinished text to the next post i
Note to Self — move this unfinished text to the next post i

Childbirth in the United States is disastrous for childbearing women when compared to other comparable developed countries and has been very bad for a very long time – 125 years to be exact.
Since 1900, the maternal mortality rate for our very wealthy country has been at the very bottom of the list for maternal deaths when compared to other wealthy developed countries.
I have already described the travesty of so-called normal childbirth in the obstetrical department all over the United States that I personally witnessed as an L&D nurse. This was during the bad old days when Twilight Sleep drugs were still being used during labor (at least in racially-segregated southern states), general anesthesia was routine for white labor patients and normal birth was conducted as a series of surgical interventions that included episiotomy, forceps extraction of the unborn baby, manual removal of the placenta and suturing the perineal incision.
But I don’t believe this story can be fully appreciated. The major part of the story is the routine use of horrifically dangerous and dysfunctional interventions in normal childbirth that went on unchallenged for more than 70 years.
But I am also grateful to the small but important handful of obstetricians who clearly saw the total irrationality of the American obstetrical profession and spoke up frequently and forcefully.
Unfortunately, the influential leaders in early 20th century obstetrics simply, stubbornly refused to listen and insisted on “having it their way” no matter how many innocent women and babies died. The historical record is crystal clear — what the American obstetrical profession routinely, as the formal “standard of care” for healthy childbearing women, really was a criminal act. This consisted of the routine use of painful and medically unnecessary obstetrical interventions and conducting so-called ‘normal’ childbirth as a surgical procedure that included general anesthesia, the routine use of forceps and manual removal of the placenta.
America. No one want the first month of their newborn’s life be in the hospital nursey while its new mother is being treated for unexpected complications in the hospital’s ICU.
This foolish system has never been the “norm” in Japan, European countries and most other parts of the world. This not only wastes lives but obstetrical interventions and the complication that so often result in cost a small fortune.
PENDING –> future link to next section of part one
In 1932 imported to stand-along list of salacious comments by obstetricians about midwives
As Americans, we are generally so proud of having the very “best” of everything – cars, schools, the best universities, democracy, computers, the Grand Canyon, great beaches – that we haven’t paid attention to what happens to millions of American women who give birth every years and the shocking news that more of American mothers die during or within 42 after giving birth that any other developed countries. The MMR is so high in the US that we fall belong a long list of so-called “third world countries”.
