~ 3B ~
Index for this last post
- Central Fetal Monitoring: The newest kid on the block half a century later
- Trying to build a better mousetrap instead of building a better foundation
- Why the subtle distinction btw acidemia & hypoxia matters
- The Glaringly Obvious Effect of EFM — turning healthy women into passive & bed-ridden maternity patients
- Photo Album ~Women disappearing into the obstetrical “system” — passive non-persons laying on their backs, covered by drapes while their “providers” peer out at them over surgical mask
- Excerpt –> Violence Against Women in Health Care Institutions: an emerging problem ~ British Medical Journal /The Lancet, May 11, 2002
Central Fetal Monitoring: The newest kid on the block half a century later
The introduction of central monitoring allows hospitals to centralization the fetal monitoring function of their L&D units. This new system for transmits the data from individual EFM machines to a central display system; it is just the latest iteration of this fever pitch to replace people with electronics.
 Central fetal monitoring frees up nurses so they no longer have to be personally present in the mother’s labor room. They can skip the patient’s labor room altogether while they monitor several labor patients at one time from the comfort of their chair at the central nurses’ station in the hallway.
Central fetal monitoring frees up nurses so they no longer have to be personally present in the mother’s labor room. They can skip the patient’s labor room altogether while they monitor several labor patients at one time from the comfort of their chair at the central nurses’ station in the hallway.
- The guidelines for healthy women with uncomplicated pregnancies do not recommend continuous monitoring.
Trying to build a better mousetrap instead of building a better foundation
During the 1970s, EFM became the de facto standard for obstetrical care in the US. and replacing simple periodic auscultation (IA) with continuous electronic fetal monitoring. As noted in the many studies quoted above, the universal use of EFM did not turn out to be the answer to the obstetrician’s prayer as everyone hoped.
But this disappointment did nothing to dislodge obstetrical faith in electronic monitoring systems. The profession spent its a huge proportion of its resources trying to improve and refine EFM’s electronic circuitry and making other tweaks the machinery, alway anticipating that the perfected ‘magic bullet’ was just around corner.
Unfortunately, this blind faith in the ability of c-EFM to eliminate newborn neurological complications created a series of problems, not the least of which was a malpractice nightmare for obstetricians. Having extolled the virtues of obstetrical care augmented by c-EFM and Cesareans as a virtual guarantee of a ‘perfect’ baby every time actually set up a situation in which obstetricians got sued every time they didn’t deliver “the goods” — i.e. a perfect baby.
The much bigger and more important picture is even more an issue for childbearing families and for society is developing effective way to do what EFM said it would do, but turned out not to be able to “delivery the goods”. This of course in to find the real cause and prevention of cerebral palsy and similar newborn problems.
The obstetrical profession’s fifty-year focus on refining and expanding the EFM system diverted attention away from studies that looked into other origins and explanations for the unexpected problems of cerebral palsy and neurologically-damaged babies subsequent to perfectly normal pregnancies and normal labors and births.
In addition, these researchers concluded that development of cerebral palsy and other forms of permanent neurological damage extremely rare during a normal labors. This held true even when some FHR abnormalities consistent with intrauterine hypoxia were recorded by the monitor tracing. The science identifying the biological origins of CP and newborn neurological damage found that metabolic acidemia (as differentiated from respiratory acidemia) was directly associated with a baby that developed CP. At the same time, researcher were able to determine that brief to moderate episodes of hypoxia (inadequate oxygenation at a cellular level) were not associated with increased rates of CP and newborn encephalopathy.
Why the subtle distinction btw acidemia & hypoxia matters
The distinction btw metabolic acidosis and labor-related hypoxia is subtle even for highly-trained medical professionals. But this is critically important, as the reasoning behind c-EFM was the assumption that fetal hypoxia during labor was the causative agent in cerebral palsy and similar neurological problems.
Continuous EFM was specifically developed to detect the slow development of hypoxia over long periods as the unborn baby was being exposed to less-than-adequate oxygenation (such as a placental insufficiency, post-mature pregnancy or maternal hypertension).
The other known cause for CP and neonatal encephalopathies are of course acute obstetrical emergencies, such as a placental abruption, cord prolapse or a life-threatening medical emergency for the mother. But again, these emergency have little or nothing to do with EFM, as they are usually diagnosed by other symptoms and monitoring the vital signs of the mother. No form of EFM, no matter how well ‘perfected’, can predict, prevent or treat these occurrences.
If you are interested in learning how intermittent auscultations (IA) works, this link will take you to a stand-alone post on IA
Conclusion
As long as this essay is, I didn’t include many issues known to increase the problems associated with our highly-medicalized obstetric system.
The topic that got the short shift was the simple but profoundly important principles of physiological management. Physiologic methods aim to safely manage childbirth without depending on drugs like Pitocin to progress the labor, narcotics to manage pain, or surgical procedures to deliver the baby.
Instead of obstetrical interventions, midwives depend on the normal physiology of childbearing, which in turn depends on mothers being able to move around freely, receive one-on-one support, able to use upright positions and make right use of gravity, as well as non-drug methods of pain relief that include walking, hot showers, and submersion in a deep water tub.
Midwives believe in the innate ability of childbearing women to labor spontaneously, push their babies out under their own power and properly take credit for this accomplishment.
As midwives, we do our part by fully present throughout active labor, eyes-on, ears-on, hands-on care and generous frequent encouragement. This includes but is not limited to monitoring the physical wellbeing of the mother, and intermittent auscultation (IA) of the fetus, to be as sure as possible that we would detect any problems for the unborn baby and take appropriate action.
Contrast this with allopathic medicine, which is officially defined as the use of drugs, surgery and ionizing radiation. American MDs are not interested in learning about ways to do things that don’t include the use of drugs or surgery. As a result, our medical schools don’t teach the physiological management of normal childbirth. Practicing obstetricians generally don’t know, don’t use, don’t like, don’t understand, don’t believe in and certainly don’t approved of physiologically-based care or practitioners (i.e. midwives) who use provide physiological management.
So it comes as no surprise that over 90% of women laboring in the obstetrical system are given epidural and are continually monitored. The blow-back from this creates a consistent set of other problems that require the same few interventions — IV Pitocin to speed up the labor, maternal oxygen mask as minor but non-reassuring changes begin to show up on EFM strip and far too often, the decision to do an emergent c-section based on a combination of slow or no progress and increasing signs of possible fetal distress as recorded by the EFM (i.e. non-reassuring fetal heart rate).
The Glaringly Obvious Effect of EFM — turning healthy women into passive & bed-ridden maternity patients
What stick out most in my mind as I googled photos of electronic fetal monitors and laboring women as was how EFM turned healthy women into passive maternity patients, lying still and listless in bed, so as not to infer with working of the the machines they were hooked up.
Everything about the design of ‘modern’ obstetrical units and the ministrations of the L&D staff revolves around the hospital’s computer-based electronic fetal monitoring system. The nurses have to keep graph paper in the tray, unplug all the leads every time the mother has to go to the bathroom, and most time-consuming of all, repeatedly tweak the placement of the toco and monitor belts on the mother’s belly find the signal and be sure its being is recorded.
Everyone hopes that EFM tracing will keep the doctors and the hospital from being sued and the icy fear in the back of their mind that they might slip up and the EFM proof needed to prevent litigation can’t be found.
But the real tragedy is what c-EFM does to laboring women. They have been ‘disappeared’ from the system. Instead of healthy individuals experiencing the most important and joyous day of their lives, they have been dependably turned into faceless compliant patients doing their part to make the OB department into a profit center for the hospital.
Stand-alone version of the section on IA — principles and technical skills
Women disappearing into the obstetrical “system” — passive non-persons laying on their backs, covered by drapes while their “providers” peer out at them over surgical mask
 |
 |
 |
 |
 |
 |
 |
 |
 |
 Obstetrician using surgical scissors to cut an episiotomy |
 |
 |
 Obstetrical surgeons delivering the baby thru the Cesarean incision |
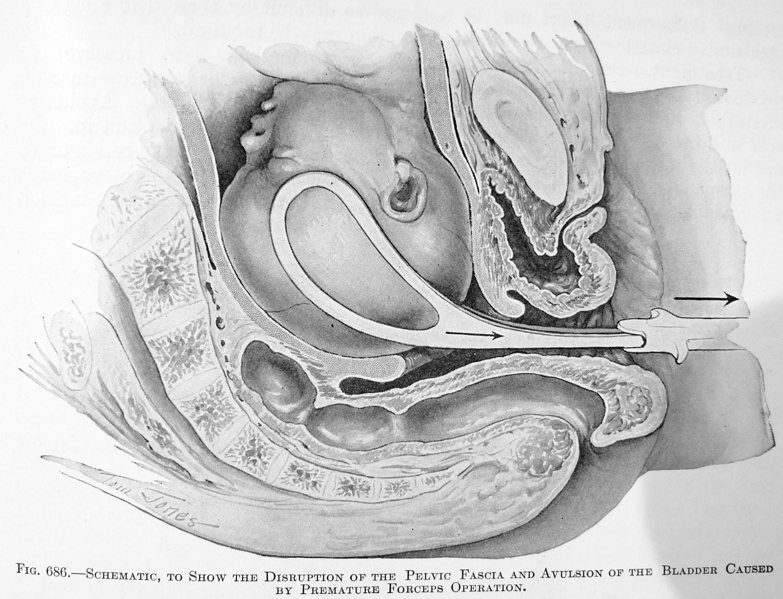
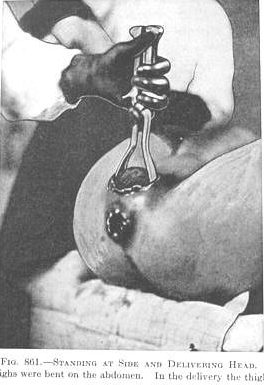
 Breech baby being extracted through the uterine incision after forceps were used to deliver its head |
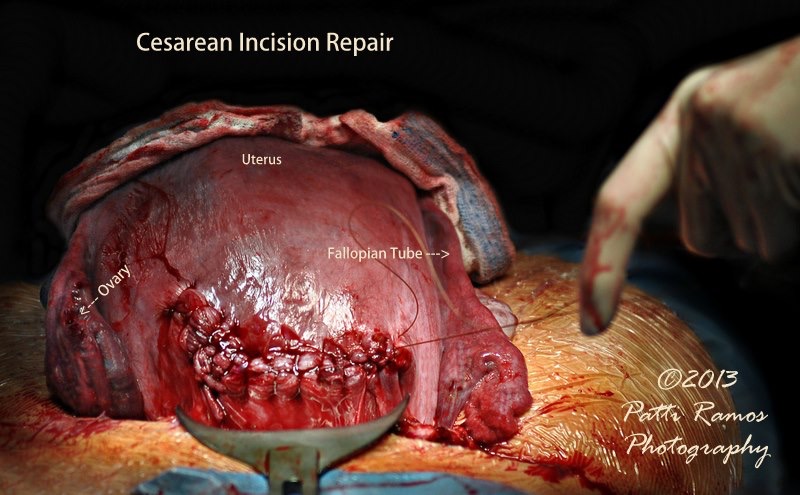 After the baby was delivered by C-section, the mother’s uterus was lifted out of her abdomen through the incision and placed on the outside of her body while the obstetrical surgeon sutures up the 4-inch incision into the uterus itself |
Excerpt –> Violence Against Women in Health Care Institutions: an emerging problem ~ British Medical Journal /The Lancet, May 11, 2002
Other important forms of violence against women occur in reproductive health services and deserve more discussion than is possible in a short article.
These forms include excessive or inappropriate medical treatments in childbirth, such as doctors doing caesarean sections for reasons related to their social or work schedules or financial incentives or adhering to obstetric practices that are known to be unpleasant, sometimes harmful, and not evidence based, including shaving pubic hair, giving enemas, routine episiotomy, routine induction of labour and preventing women having companions in labour.
Shoulder Dystocia Rate Constant Despite Risk Factors – Medio-legal Implications Parity, C-Section, Birth Wt / Ob.Gyn.News, May 15, 2003, Vol 38, No 10;
Shoulder dystocia appears to occur at a constant rate, despite increased cesarean sections and variations in other risk factors, Dr. Michael Lucas reported at the annual meeting of the Society for Gynecologic Investigation.
“It seems counterintuitive,” said Dr. Lucas of the University of Texas, Houston, in an interview. “There’s this notion that if we manipulate the risk factors we should see a lower rate of shoulder dystocia, but that does not appear to be the case.”
His study of more than 12,650 births in two Houston hospitals showed a similar rate of shoulder dystocia, despite differences in the risk factors of parity, birth weight, cesarean delivery, and operative vaginal delivery between the two hospital populations. The findings could have implications in the defense of shoulder dystocia cases.
“The argument has always been that there are risk factors for shoulder dystocia, which the physician should have acted on,” he said. “Our data suggest this is not true. It may at least be argued that we can take a population with a much different rate of risk factors and have virtually the same rate of shoulder dystocia. This is important clinically, because it supports the notion that our options and our ability to avoid trauma with this complication are limited.”
Dr. Lucas researched the obstetric databases of an urban public hospital and a community teaching hospital … The community hospital had twice the rate of cesarean deliveries, fewer multiparous mothers, a lower operative vaginal delivery rate, and smaller babies, factors usually associated with lower rates of shoulder dystocia.
Still, both hospitals had virtually the same incidence of shoulder dystocia: 1.1% and 1.3% of vaginal births at the public and community hospital, respectively…The community hospital had a higher cesarean delivery rate than the public hospital (30% vs. 14%) and more babies weighing less than 4,000 g (59% vs. 41%).
Babies with shoulder dystocia tended to be smaller (3,844 g vs. 4,117 g) at the community hospital .. The operative vaginal delivery rate was higher at the public hospital than at the community hospital (11% vs. 8.5%).
… the high cesarean delivery rate, lower rate of multiparity, and lower birth weight at the community hospital were not associated with a reduced rate of shoulder dystocia.
“It seems intuitive to say if you avoid a vaginal delivery you can lessen the rate of shoulder dystocia, but this doesn’t appear to hold water,”Dr. Lucas said.
