Overview (Part 1 of 7)
Easy-to-share link ~ https://tinyurl.com/y5q26wbn
Note: this link leads to the first post only. To access sequential parts of the story, just follow the link at the bottom of each post.
 Faith Gibson, LM
Faith Gibson, LM
Former L&D nurse,
MBC’s Midwifery Advisory Council 2007-2013
Part 1 Overview is broken into two consecutive posts to make reading easier.
Historical Overview
How the ‘wrong use’ of obstetrics came to be the standard of care for healthy women in the US in 1910, why we should care now and what can be done to fix these problems
A fast trip in the Way-back Machine ~ 1500-1900: Four hundred years before the development of “modern medicine”, during the Age of Enlightenment in Europe, the new science of human anatomy and physiology opened up new ways of thinking about ‘the healing arts’, as medicine was historically known.
But simply seeing “under the hood“, that is, the ability to label human body parts and figure out how the pipes connected up to each other did not immediately or directly provide doctors with cures for the great multitude of diseases that plague the human condition. Knowing what a pancreas looks like and understanding what it does is good, but that’s a long way from being able to chemically synthesize insulin to treat diabetes. That didn’t happen until 1923, almost 400 years later.
However fascinating, the accurate understanding of human anatomy made only a tiny difference in the ability of doctors to effectively treat painful or fatal diseases. During this pre-antibiotic era (all human history before the 1935 marketing of sulfa drugs in Germany), the biological risks of childbearing went on pretty much as before, which is to say that pregnant women died of eclampsia (the complication that killed the character “Sybil” on Downton Abbey), while hemorrhage and infection took the lives of other new mothers.
Luckily the scientific method of inquiry continued to soldier on, century after century, building on the knowledge of earlier discoveries. Many dedicated scientist-physicians advanced medical science by ‘standing on the shoulders’ of those who went before them. Their love of learning built up this powerful new body of knowledge, minute by minute, day by day, decade after decade, each tiny advance followed faithfully by other diligent scientists.
Eventually, this dedicated and often dogged patience in organic chemistry, the biological sciences, and physics, combined with soaring imaginations, created what we now call the “modern” or scientific practice of medicine. These medical advances were soon applied to the realm of pregnancy and childbirth and this eventually allowed doctors to accurately diagnose abnormal conditions. In most cases (but not all) obstetricians, in combination with the technical services of acute-care hospitals, could effectively treat the most common complications of childbearing.
 Historically, the medical discipline of obstetrics and the surgical discipline of gynecology were economic rivials and the bitterest of enemies. Doctors from these two disciplines often had heated argument so intense that a first-fight broke out.
Historically, the medical discipline of obstetrics and the surgical discipline of gynecology were economic rivials and the bitterest of enemies. Doctors from these two disciplines often had heated argument so intense that a first-fight broke out.
The animosity became so bad that influentical leaders in each discipline decided something had to be done to end this unseemly (and very unprofessional) rivalry. So in the early 1900s, they combine the medical discipline of obstetrics and surgical discipline of gynecology it a new hybrid surgical specialty of obstetrics and gynecology.
However, what we now enjoy as “modern medical science”, with its many new medical “miracles”, magic bullets and wonder drugs, did not become a fully realized until May of 1944 when wartime production of Penicillin was sufficient to supply the civilian population. A therapeutic dose of this life-saving ‘magic bullet’ cost $35 in 1945.
At this point in history, obstetrics had earned its place as a full partner in the advancement of medical science. Newer, better and expanded medical treatments meant antibiotics to treat septicemia (childbed fever) and other infections. Blood typing was able to identify the mother’s Rh-factor and make transfusions safer if needed to treat hemorrhages. Safer anesthetic methods, improved surgical techniques developed by battle surgeons during WWII, allowed obstetricians to prevent unnecessary suffering and disabilities and save many lives.
Personally, I’m profoundly grateful for the wonders of modern obstetrical medicine, as is everyone I know.
A Two-edged Blade
Unfortunately, the obstetrical miracles of the 19th and 20th century also had a distinct shadow-side. Obstetrics was part of the American medical system that had its roots in “German” method — what we now call an “allopathic” (as contrasted with homeopathic) medicine. The primary methods of allopathic treatments are prescription drugs and surgery.

Vail of Scopolamine
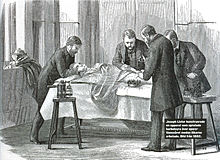
In different eras of obstetrical history were heavily influenced by different ill-advised or unnecessary interventions in normal childbirth were popular. In the early 1900s, when doctors replaced midwives and childbearing women began to be routinely hospitalized, the contemporary “style” was called “knock’em out, drag’em obstetrics”. This mandated that every laboring women be repeatedly injected with a dangerous drug cocktail known as “Twilight Sleep” (morphine and scopolamine) during labor and kept in a semi-conscious state.
Under these circumstances, the family of was not permitted to visit or even see the laboring woman, nor was she allowed to eat or drink, even if she was in labor for 24-48 hours (routine IV hydration was not yet part of OB care). During these many hours, the mother was subjected to repeated vaginal exams.
Normal birth, which had been renamed as the surgical procedure of “vaginal delivery” was conducted on a mother rendered unconscious with general anesthesia (ether or chloroform). Under the obstetrical model, women no longer “gave birth” under their own power, but instead were “delivered” by the expertise of the doctor.
 As with other forms of allopathic medicine, this often made the ‘treatment worse than the disease‘, only in this case, there was no ‘disease’ that needed to be treated but the idea that the best way to avoid complications was the “pre-emptive strike”.
As with other forms of allopathic medicine, this often made the ‘treatment worse than the disease‘, only in this case, there was no ‘disease’ that needed to be treated but the idea that the best way to avoid complications was the “pre-emptive strike”.
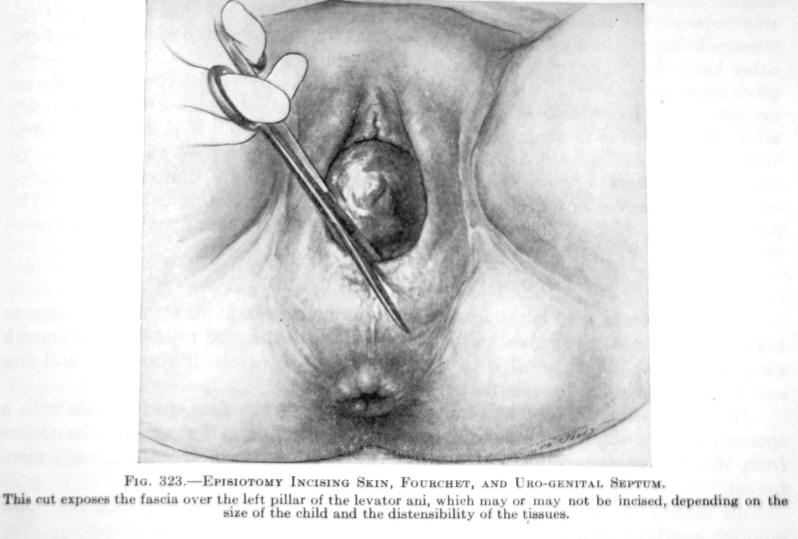
In these cases, what would have been the treatment for a particular problem was used ‘prophylactically’. For example, cutting an episiotomy to prevent the mother from having a perineal ‘tear’ and using forceps to be sure the baby didn’t get stuck and require a forceps delivery.
In the bio-hazardous environment of a hospital, each invasive procedure (vaginal exam, episiotomy, use of forceps, manual removal of placenta, etc) risks introducing a potentially-fatal bacteria. During this pre-antibiotic era, puerperal sepsis (often called childbed fever, now referred to as ‘septicemia’) was the most frequent cause of maternal death until penicillin became publicly available in 1944.

Mother delivered under general anesthesia, severely depressed baby
The “right use” of obstetrical prowess has always been its unique ability to effectively treat complications. Depending on the circumstances, obstetrics could obviously be a great force for good, or that same ability to overwhelm Mother Nature could also cause great harm.
In such cases, these drastic medical treatments, invasive surgical procedures, and their side-effects were seen as the price to be paid for saving the life of mother or baby.
But when these restrictive policies, drastic interventions, powerful drugs, and invasive surgical procedures were (or are) used routinely on healthy women with normal pregnancies, it is a decidedly “wrong use” of obstetrics.
In these cases, healthy women with no life-threatening condition or complications faced all the same risks, side-effects, and complications but without any benefit. Since this high level of medicalization was not necessary, these women and their newborns got nothing in return for bearing the pain, humiliation and these many healthy risks routinely inflected in the course of care.
Turning the Mother’s Shield into the Obstetrician’s Sword
The issue that arises again and again in this 7-part series is the very normal expectation by the public and by each patient that a doctor’s duty is “In the first place, do no harm”.
When a doctor’s care results in harm for whatever reason, its called an “iatrogenic” complication. It doesn’t matter if the iatrogenic harm was the result of acts or omissions by an individual doctor or a consequence of inappropriate policies, practices or protocols decreed by the entire obstetrical profession to be the proper “standard” of care.
The medical profession across the board is always responsible for putting the needs of each individual patient before the personal need or convenience or professional status of an individual doctor or the profession of medicine itself.
 Over the centuries, physicians who practiced obstetrics were often mistaken about what was helpful or safe and their understanding of biology before the modern age was often inadequate or incorrect. This included several historical incidences of note: The discovery by Dr. Semmelweis that fatal childbed fevers were an infection spread on the unwashed hands of doctors, and the scandal when his Austrian colleagues refused to wash their hands; Dr. Williams and the routine use of twilight Sleep drugs and general anesthesia; Dr. DeLee and his promotion of routine forceps deliveries.
Over the centuries, physicians who practiced obstetrics were often mistaken about what was helpful or safe and their understanding of biology before the modern age was often inadequate or incorrect. This included several historical incidences of note: The discovery by Dr. Semmelweis that fatal childbed fevers were an infection spread on the unwashed hands of doctors, and the scandal when his Austrian colleagues refused to wash their hands; Dr. Williams and the routine use of twilight Sleep drugs and general anesthesia; Dr. DeLee and his promotion of routine forceps deliveries.
In all of these cases, it was bull-headedness and hubris that prevented the obstetrical profession from correcting potentially-fatal problems that resulted in the preventable deaths of more than million new mothers and their newborns between 1840 and 1940.
These problems arose when mistaken beliefs lead to the uncritical use of unscientific and harmful practices or the propagation of irrational policies.
Far too often in the history and even contemporary times (current misuse of EFM), ill-advised but ‘customary’ practices have been held in a death grip by influential leaders because the status quo was the advantage of the obstetrical profession. Instead of doing what was best for the women and families they served, the institutionalized use of medically-unnecessary interventions systematically introduced artificial risks that resulted in preventable complications in otherwise healthy women or their newborns.
 When obstetrical interventions used to effectively treat specific complications are routinely or ‘pre-emptively’ used in healthy women with normal pregnancies, the outcome of these policies and practices are neither helpful or benign. Over the centuries and continuing into the present day, the shadow side of obstetrical has been responsible for perpetuating harmful practices that caused a great deal of unnecessary suffering and sometimes resulted in the preventable deaths of both mothers and babies.
When obstetrical interventions used to effectively treat specific complications are routinely or ‘pre-emptively’ used in healthy women with normal pregnancies, the outcome of these policies and practices are neither helpful or benign. Over the centuries and continuing into the present day, the shadow side of obstetrical has been responsible for perpetuating harmful practices that caused a great deal of unnecessary suffering and sometimes resulted in the preventable deaths of both mothers and babies.

Extremely depressed baby after its healthy mother was given narcotics during labor, general anesthesia during delivery, and forceps used to pull the baby out. Notice that its umbilical cord is flat with no blood circulating between the placenta and the baby
Unfortunately, the shadow side of the obstetrical practice is never acknowledged in public or incorporated into public policy debates on our current obstetrically-defined maternity care system. This needs to be corrected, along with reintroducing the scientific principles of physiological management as the standard of care for healthy women with normal, low-risk pregnancies.
Providing a long view of what I referred to in the title as the “dark history of obstetrics” is the subject of this series of essays.
