~ 1B ~ word count 2,100
In the first place ‘Do No Harm’
Conforming opinion to facts — acknowledged
scientific evidence — within an ethical framework
In his autobiography, The Story of My Life, Dr. Marion Sims
wrote about the advantages of working on people
that were essentially his property (i.e. women slaves):
“There was never a time that I could not,
at any day, have had a subject for operation.”
oOo
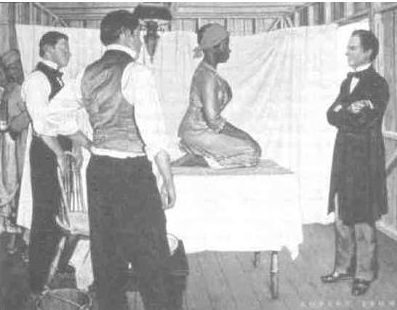
Dr. Sims, a southern slaveholder, self-taught 19th-century surgeon, and inventor of the vaginal spectrum, began experimenting in 1845 w/ surgical treatments to repair damage from childbirth, particularly vaginal fistulas. He perfected his techniques by operating, repeatedly and without anesthesia on the same 3 women slaves. He repeatedly used the slave named Lucy (photographed here) to demonstrate or teach his surgical techniques to medical students and other doctors.
Contemporary history of Dr. Sims & his statute in NYC’s Central Park
*o*O*o*
This post is dedicated to the 19th-century American slave Lucy,
in memory of all her unnecessary suffering, as well as the disturbing fact
that today black mothers in the US still have a maternal mortality
rate 3-to-4 times greater than white mothers.
Beginning with First Principles
This second post begins by establishing a “First Principle” as a foundation for evaluating and judging the validity of medical practices, including those of obstetrics and other healthcare disciplines.
This foundational principle is a combination of both ethics and pragmatics, and is best communicated by these two maximums:
First ~ The 2,500-year-old Hippocratic Oath for the practice of medicine in all its branches: says: “In the first place do no harm”
Second ~ A socially pragmatic but scientifically-sound ethical policy of: “Conforming our opinions to the available facts“

The R2D2 of the obstetrical world
With this ethical pragmatism in mind, I begin with the scientific evidence — facts — reported in the many dozens of studies published since 1975 to determine if continuous EFM was more, less or equal in effectiveness to auscultation — the traditional method of monitoring unborn babies during their mother’s labor — and if there were any side effects or other “unintended consequences” of c-EFM.
In many instances, I’ve included a link to these research documents when they are available (original study or excerpts) on the Internet. Sometimes a quote or excerpt in the post will still have its citation number that is active (a clickable link). I also have a subdirectory with a small sample of this research.
The consensus of the scientific literature on routine EFM of healthy women with normal pregnancies
A very large volume of research (1975-2019) in the US on the effectiveness of routine EFM in low-risk pregnancies (70-85% of the childbearing population) has concluded:
Compared to auscultation in a healthy low-risk cohort, EFM fails to predict, prevent or reduce the incidence of cerebral palsy and other newborn neurological disorders.
Stated more explicitly:
When the protocols of auscultation — listening regularly with a fetoscope or hand-held doppler for one full minute or longer — are used during the labors of healthy women with normal pregnancies, the neurological outcome for their babies is the same as EFM — no difference in CP rates or other perinatal neurological problems associated with childbirth.
 But that is not the end of the EFM story. In addition to a lack of benefit to the newborn baby, the use of c-EFM in this healthy population is associated with a statistically-significant increase in Cesarean surgeries.
But that is not the end of the EFM story. In addition to a lack of benefit to the newborn baby, the use of c-EFM in this healthy population is associated with a statistically-significant increase in Cesarean surgeries.
It turns out that auscultation is safer for mothers. They get the same outcome for their babies, but no increase in their Cesarean rate and associated maternal morbidity and higher mortality.
Under the principles of “Informed Consent”, all birth attendants who provide care to healthy women with low-risk pregnancies have a duty, from a legal and ethical standpoint, to inform healthy women and their families that auscultation has been shown scientific evidence to be “best practice” for women like themselves.
Reducing the C-section rate in important at several levels, as it directly eliminates all the immediate and long-term complications associated with this major surgery. This includes issues such as intra-operative hemorrhage, blood transfusions, post-operative infection, ICU admission, prolonged hospital stays, re-hospitalization, and a 13-fold increase in emergency hysterectomies within 14 days of giving birth.
Delayed complications of Cesarean surgery include abdominal adhesions and bowel obstructions and secondary infertility and the extremely controversial topic and risks of VBAC – laboring and giving birth vaginally after a previous C-section.
 Downstream complications include several very complications in post-cesarean pregnancies including uterine rupture and placental abnormalities that result in unexpected fetal demise, placental abruption, and abnormal placental implantation.
Downstream complications include several very complications in post-cesarean pregnancies including uterine rupture and placental abnormalities that result in unexpected fetal demise, placental abruption, and abnormal placental implantation.
Complications of abnormal implantation include placenta previa, placenta accreta, and the catastrophic and potentially fatal placental percreta. This describes a placenta that grows thru the uterine wall and attaches itself to the mother’s abdominal organs. Delivery requires a Cesarean hysterectomy and despite the most expert care in the very best hospitals, placenta percreta is associated with a 7-10% maternal mortality rate from a torrential hemorrhage.
Last, but certainly not least, are the potential complications associated with subsequent vaginal births (VBAC).
Greater economic burden of Cesarean delivery and its complications
The increased C-section rate associated with routine use of EFM is rarely or never acknowledged by hospitals and the obstetrical profession. However, the immediate and long-term costs associated with each Cesarean are extraordinary, especially for families that are under- or uninsured.
But when that expense is multiplied by our high C-section rate, it is no surprise that health insurance companies often refuse to insure women who have had a previous Cesarean. They don’t want to cover the extra expense when new mothers have to spend days in the ICU, get blood transfusions, need an emergency, be re-hospitalized, or is diagnosed with placenta precreta that will require a very risky Cesarean hysterectomy.
 Excellent studies that found no statistically-significant benefit when EFM was routinely used on healthy women with low-risk pregnancies, but identified a significant increase in Cesarean delivery rate associated with continuous electronic monitoring
Excellent studies that found no statistically-significant benefit when EFM was routinely used on healthy women with low-risk pregnancies, but identified a significant increase in Cesarean delivery rate associated with continuous electronic monitoring
As the series progresses, I will continually provide relevant references and excerpts from published research. I’m beginning with the eight listed below, as they report some of the most startling facts about this controversial topic. A forensic evaluation of these facts directly supports the information in this provided in series and my conclusions are consistent with the consensus of the scientific literature.
Here is a link to subdirectory of EFM studies and other research on related topics
Links and excerpts from a set of studies and other research that is particularly helpful.
1. ACOG Task Force on Neonatal Encephalopathy & Cerebral Palsy;
Am. College of Obstetrician & Gynecologists 2003
- the majority of newborn brain injury does not occur during labor and delivery.
- …. most instances of neonatal encephalopathy and cerebral palsy are attributed to events that occur prior to the onset of labor.
2. Ob.Gyn.News ~ September 15, 2003 Documentation Important in CP Deliveries:
The increasing cesarean delivery rate that occurred in conjunction with fetal monitoring has not been shown to be associated with any reduction in the CP rate……
Only 0.19% of all those in the study had a non-reassuring fetal heart rate pattern….If used for identifying CP risk, a non-reassuring heart rate pattern would have had a 99.8% false positive rate….” [emphasis added]
3. Electronic Fetal Monitoring as a Public Health Screening Program: The Arithmetic of Failure;
Dr David Grimes and Jeffrey F. Peipert, MD, PhD; OBSTETRICS & GYNECOLOGY, Vol 116, No. 6, December 2010
“… fetal monitoring has failed as a public health screening program.
Randomized controlled trials of electronic fetal monitoring compared with intermittent auscultation reveal that electronic fetal monitoring significantly increases instrumental and cesarean deliveries for women, but provides no long-term benefits for children. [2]
“the positive predictive value of electronic fetal monitoring for fetal death in labor or cerebral palsy is near zero.
Stated alternatively, almost every positive test result (of EFM) is wrong.”
4. Ob.Gyn.News; August 15, 2002 Vol 38, No 8 edition C-Section to Prevent Cerebral Palsy: Results May Be a Wash
“Performing cesarean section for abnormal fetal heart rate patterns in an effort to prevent cerebral palsy is likely to cause as least as many bad outcomes as it prevents” …..the false-positive rate for these abnormal fetal heart patterns was 99.8% (N.Engl. J. Med 334[10:613-19, 1996)
“Extrapolating from this study, Dr. Hankins calculated that a physician would have to perform 500 C-sections for multiple late decelerations or reduced beat-to-beat variability to prevent a single case of cerebral palsy.
But since Cesarean section carries a roughly 0.5% risk of future uterine rupture, those 500 C-sections would result on average in 2.5 uterine ruptures. This, in turn, would cause one case of neonatal death or cerebral palsy….”
5. Fetal Heart Rate Monitoring Update: The Good, the Bad and the Atypical
The Female Patient April 2011, includes 8 additional references
“Despite the widespread use of EFM, there has been no decrease in cerebral palsy. … a meta-analysis of randomized control trials has shown that EFM has no effect in perinatal mortality or pediatric neurologic morbidity.2
However, EFM is associated with an increase in the rate of operative vaginal and cesarean deliveries.1”
6. Ob.Gyn.News; August 1, 2002, Vol 36, No 15 ~ Elective C-section Revisited by Dr. Elaine Waetjen
….why shouldn’t we offer prophylactic C-section to prevent this problem later in life?
The answer is that the evidence does not support this approach. Preventive strategies should cause no more harm than the disease or problem that they are tying to prevent. Ideally, they should incorporate some kind of screening to identify people at risk. They should be cost-effective and based on very good evidence of benefit. Elective C-section to preserve pelvic floor function fails on all their measure.
“Cesarean surgery causes more maternal morbidity and mortality than vaginal birth. In the short term, C-Section doubles or triples the risk of maternal death, triples the risk for infection, hemorrhage, and hysterectomy, increase the risk of serious blood clots 2 to 5 times and causes surgical injury in about 1% of operations.
In the long term, cesarean section increases the mother’s risk of a placenta previa, accreta or percreta, uterine rupture, surgical injury, spontaneous abortions and ectopic pregnancies while decreasing fecundity.
7. Fetal Monitoring: Creating a Culture of Safety With Informed Choice; Lisa Heelan, MSN, FNP-BC J Perinat Educ. 2013 Summer; 22(3): 156–165. doi
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4010242/
Continuous EFM was embraced by the obstetric community, including nursing even though clinical trials did not show evidence supporting its use in low-risk women when compared to Auscultation (Banta & Thacker, 1979; Dixon, 1981; Haverkamp, Thompson, McFee, & Cetrulo, 1976).
The indiscriminate use of EFM in the labor room is not improving outcomes and is actually causing harm to healthy women with uncomplicated pregnancies.
Employing a low-tech, high-touch approach needs to be the main philosophy while providing nursing care to most laboring women.
8. Uncertain Value of Electronic Fetal Monitoring in Predicting Cerebral Palsy
Karin B. Nelson, M.D., James M. Dambrosia, Ph.D., Tricia Y. Ting, B.S., and Judith K. Grether, Ph.D. New England Journal of Medicine 1996; 334:613-619 DOI: 10.1056/NEJM199603073341001
The introduction and wide dissemination of fetal monitoring occurred before randomized clinical trials had evaluated its efficacy.
More than 20 years and 11 randomized trials later, 1-6 electronic fetal monitoring appears to have little documented benefit over .. auscultation with respect to perinatal mortality or long-term neurologic outcome.
Furthermore, probably in part because of the widespread use of fetal monitoring,7 the rate of cesarean section has increased, with a resulting increase in maternal morbidity and costs but without apparent decrease in the incidence of cerebral palsy.
MedScape Ob/Gyn & Women’s Health; 9/16/02
What I learned on my first day of school
as a student nurse and will never, never forget . . .
by Bonnie Faith Grunow Gibson, LM

On my first day of class as a brand new nursing student, our instructor and director of the program, Miss Etta McLaughlin (who I worshiped) began our education as healthcare professionals by telling this story to 17 fresh-faced and eager young women with no idea what it meant to be a nurse or other professional healthcare provider:
“Long ago and far away there was an older woman who sold eels in the town square. She showed up every market day with a small table, a stool to sit on, a wood cutting board, knife, container of pins, and two buckets — one filled to the brim with black, slimy, wriggling eels and the other bucket was empty.
As was her custom, she spent her day reaching into the bucket and extracting one eel at a time. Then she deftly stretched the creature out on the wooden cutting board and swiftly plunged a pin into its head at one end and another pin into its tail. Once the eel was secured stretch out to its full length, she picked up her knife and made a well-practiced incision that split the eel open ran from stem to stern. Then she separated the parts to be sold, which went into the empty bucket, and discarded the leftover parts on the ground.
One day a stranger came to town and walked around the market and visited all the stalls. When he came to the one that sold ells, he stopped and just watched for a considerable length of time as the old woman endless repeated the motion of reaching into the bucket to withdraw a very much alive and wiggling ell, and then nailing, slicing and extracting eel meat.
Finally, the spoke up, voicing distress about something that looked to him like a barbaric ritual. He asked the ell seller why she didn’t just kill the eels first, or at the very least, knock them out before cutting them open? Don’t she care that she was unnecessarily inflicting terrible pain on these helpless creatures?
She stared at him for a second or two and in a bored but patient voice as if explaining to a child, said:
“Mister, I’ve been doing this for 20 years and they ought to be used to it by now.”
After Miss Eta finished this story, she went on to say:
“This is what it’s like to be a hospital patient undergoing any kind of frightening or painful medical treatment or procedure. No matter how familiar you are with the treatment or how long you’ve been doing it, the patient isn’t “used to it by now”, and never will be! The hard long tube, needle or scalpel always goes into the patient’s body, never into the doctor, nurse and other staff.
It’s up to you, as healthcare providers, to never forget the painful and fearful reality of the patient’s experience”.

