This continues the history of fetal monitoring as a Verb:
Development of automated electronic fetal monitors replaces Auscultation
 With the clarity of hindsight, we now know that just recording the one-minute fetal baseline rate was not sufficient to identify subtle indicators of fetal distress.
With the clarity of hindsight, we now know that just recording the one-minute fetal baseline rate was not sufficient to identify subtle indicators of fetal distress.
In the decades before and after the ideas expressed in Dr. DeLee’s 1924 textbook, untold numbers of unborn babies unexpectedly ‘crashed’ during labor or were born severely depressed.
It’s not surprising that American obstetricians and worried parents continued to wonder if better information on the biological status of the fetus — a way to know what the fetal heart rate was during every minute of the entire labor & birth — would allow them identify unborn babies in trouble in time to rescue them before damage was done.
The very first attempt to record a FHR by using an electric machine came in 1906, which was when Dr. Cremer invented the first ‘fetal monitor’, which was an electro-cardiogram that used abdominal and intra-vaginal electricalleads. (!)
Other physician-inventors attempted to determine fetal status using a microphone to magnify the auscultated FHR and electronic phono-cardiography to record it. They ultimately decided that such devices could not provide the kind of consistent results that would allow them and other obstetricians to identify early indications of fetal distress.
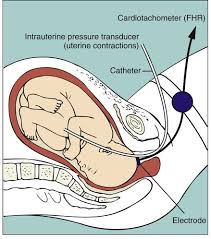
But in 1958, Dr. Edward Hon, the pioneer of modern EFM, developed the first system for capturing continuously the fetal ECG and coined the terms early, late, and variable decelerations. I don’t know for sure that Dr. Hon knew about Dr. DeLee’s observations in the 1920s, but whether he did or not, he applied Dr. De Lee’s theories and methods.
In just five years (1964), Dr. Callagan had developed a commercially viable system for capturing the FHR with Doppler technology.

By the late 1960s, EFM systems by Dr. Hon were commercially available in the United States (1968). Other pioneers in these electronic systems include Dr. Hammacher in Germany who reduced noise-to-signal ratios and Dr. Caldeyro-Barcia from Uruguay, who was father of a number of fetal monitoring terms, including Montevideo units and long-term and short-term variability.
By the early 1970s, electronic fetal monitors had been purchased by 20% of hospital obstetrical units. Today, 100% of labor and delivery units have electronic fetal monitors and over 90% of hospital births include the use of c-EFM, along with an epidural anesthesia rate over 80%.
A web article called How to read a EFM on VeryWellFamily.com concluded its description of EFM (obviously from the perspective of hospitals) by saying that c-EFM:
“… also allowed the monitoring to be done without one-on-one care at the bedside.”
EFM: Really good for business
The report about this enormous market costs a whopping $4,000, and that is only for a single person or company to read. As reported by AMR, the business in developing countries is a particular plum, very lucrative in just the sheer number of hospitals and to be perpetuated by ‘repeated business’, making it the equivalent of a ‘futures market‘ for electronic fetal monitoring devices.
 Hospitals spend much more on electronic monitoring systems than handheld Dopplers. This is consistent with a decision NOT to hire enough nursing staff to do one-on-one intrapartum care that includes the use of IA.
Hospitals spend much more on electronic monitoring systems than handheld Dopplers. This is consistent with a decision NOT to hire enough nursing staff to do one-on-one intrapartum care that includes the use of IA.Obviously hospital administrators did the math and quickly realized that making $400 each hour from insurances companies for each electronically monitored labor patient was far more profitable than losing $30-$45 each hour for each nurse’s salary who would instead monitor (the verb) the unborn baby using IA.
- blood transfusions
- emergency hysterectomy
- postpartum infections
- rehospitalizations
- all the downstream emergencies:
-
- placenta percreta in future pregnancies that requires a Cesarean hysterectomy
- ICU admission for as long as to 20 days
- maternal death for 7 to 1o out of 100 women.
The routine use of electronic fetal monitoring as the standard of care for healthy women with normal pregnancies is high-tech, high-cost, non-evidence-based care. [EvidenceBasedBirth.com]
Since the first EFM was purchased by the first hospital, the push to expand c-EFM has been ever up, up, upward, irrespective of the science, damn the torpedoes, full speed ahead! There is no doubt that a constant pitch for buying the latest hot new upgrade is being driven by the EFM manufactures, for whom the sale of EFM equipment is so profitable.
Interestingly enough, the economic goals of EFM manufactures fit perfectly with those of hospitals, for whom billing insurance carriers and the federal *Medicaid program hundreds of dollars an hour makes the use of c-EFM into one of their favorite “cash cows”.
As for the health insurance industry, they can afford to reimburse hospitals at this extraordinary rate because it’s just a pass-through for premiums paid by their customers. Anytime the insurance carriers aren’t making as much profit as they want, they can hike premiums up to the moon and back and there is NOTHING we, the public, can do — we either pay or become uninsured. So “cost containment” is not a necessary aspect of health insurance as an unregulated industry.
[**Medicaid pays for half of all births in the US]
For hospitals, this profit-making scenario is the polar opposite of having to spend hundreds an hour to hire enough L&D nurses to provide one-on-one care (i.e. to ‘midwife’ as an active verb) each patient, using IA to monitor the fetus as an eyes-on, hands-on process performed in real time by a real person.
Central Fetal Monitoring: The newest kid on the block half a century later
The introduction of central monitoring allows hospitals to centralization the fetal monitoring function of their L&D units. This new system for transmits the data from individual EFM machines to a central display system; it is just the latest iteration of this fever pitch to replace people with electronics.
 Central fetal monitoring frees up nurses so they no longer have to be personally present in the mother’s labor room. They can skip the patient’s labor room altogether while they monitor several labor patients at one time from the comfort of their chair at the central nurses’ station in the hallway.
Central fetal monitoring frees up nurses so they no longer have to be personally present in the mother’s labor room. They can skip the patient’s labor room altogether while they monitor several labor patients at one time from the comfort of their chair at the central nurses’ station in the hallway.
- The guidelines for healthy women with uncomplicated pregnancies do not recommend continuous monitoring.
Next in Mayday Series:
