Why Medical & Maternity Care in the US Doesn’t Work: The coming revolution ~ Special reading for special friends, academic researchers, & investigative journalists
 Subdirectory ~
Subdirectory ~
Links to Essays & References
Easy-to-share-link –> https://tinyurl.com/y3gtvdvd
 Connecting Up the Dots:
Connecting Up the Dots:
Ten informative essays based on 50 years of historical, political and legal research on the practice of medical and midwifery, biology of normal childbirth, our dysfunctional healthcare system, its many harmful practices, and the central role of organized medicine in shaping this problematic system.
* How the medicalization of normal childbirth came about, why it doesn’t work and how it introduces unnecessary harm to healthy women with normal pregnancies
* Why we can’t wait for or depend on the federal government to fix these problems
* Why those who understand these problems and the urgent need to reform our healthcare system must as individuals become political change agents
*Read one of the ten essays multi-part series and pass that information on to others

I’m from a Mennonite family that for the last 200 yrs has dressed “plain”. Plain-dress includes the traditional head covering, which is NOT a ‘prayer bonnet’ (& has nothing to do with prayer!) After I was arrested in 1991 by our State’s Medical Board and criminally prosecuted for the next 20 months (charges were eventually dismissed), I became politically involved in legislative efforts and attending Medical Board meeting. Obviously my “plain dress” was a barrier to interacting with the State Medical Board & Legislature, so I invented a form of dressing that is still ‘plain’ and simple, but no longer so distracting.
** A few words about myself **
After graduating from nursing school I worked for many years as an L&D nurse and later as an ER nurse. I became a professional midwife in 1996; I now provide community-based maternity care, attend planned home births and accompany client families to the hospital when they need or want obstetrical services.
I’m also am a long-time political activist working to de-medicalize normal childbirth and pass needed midwifery legislation. I was appointed by the California Medical Board to the Midwifery Advisory Council in 2007; after serving two terms I retired from the Council in 2013. However, I continue to be politically active and a frequent thorn in the side of our Medical Board.
 I’ve always been a “reader” with a particular interest in historical topics. Over the last five decades, I’ve read well over 500 books (including textbooks) on the history and practice of obstetrics, midwifery, modern models of maternity care, and the (currently dysfunctional) healthcare system in the United States.
I’ve always been a “reader” with a particular interest in historical topics. Over the last five decades, I’ve read well over 500 books (including textbooks) on the history and practice of obstetrics, midwifery, modern models of maternity care, and the (currently dysfunctional) healthcare system in the United States.
During that time, I also became the mother of three healthy children. This included giving birth to my first daughter in the back seat of our car in the hospital’s driveway as the only way to avoid being forcibly medicated (i.e. without any need for or my consent) with the standard Twilight Sleep drugs during labor and rendered unconscious with general anesthesia so the doctor could perform an unnecessary episiotomy and forceps delivery to extract my 5# 12 oz (slightly premature but healthy) baby girl.
I now am the proud grandmother of two grandsons, one of whom is in his second year at an osteopathic medical school.
I also created and maintain 9 other websites in addition to this one.
But first, the Most Important Book to Read this year
Become part of the “Gift that Keeps on Giving” by reading “The Price We Pay: What broke the American Healthcare system & how to fix it”
Until now, we midwives thought WE were the crazy ones, or that we were the ONLY people who knew that the whole system was dysfunctional.
We often saw “business as usual” at doctors’ offices, hospital wards and drugs stores that charged usury prices and instinctively knew that these things were crazy, harmful and outrageously, unforgivably unethical (if not outright criminal) but assumed it was so hopeless that we “mere mortals” could do nothing about it.
We were dramatically wrong, as it we, as midwives and the thousands of people we eventually influence, that have to become a revolutionary force for good. Changing our dysfunctional system for the better is our “revolutionary war”, not a shooting war like the one in 1776, but just as important to our democratic way of life. We must fight, in combination with other political activists, and eventually win against special interest groups, organized medicine, big pharma, EFM manufactures, and the abuse of partisan politics to block or sabotage reform efforts.
We also must acknowledge the deep lack of understanding by so many Americans that wrongly and sadly assume that America has “the best damn healthcare system on the Planet“. For a rich country, we actually have one of the worst.
But we can and we must come together to make it better and better until one of these days — 10 or 20 years from now — we might actually be able to brag that we did have a system that really sucked, but we kept working until we got it fixed and now, we really do have one of the best health and medical systems on the planet.
Become the “Gift that Keeps on Giving” by reading “The Price We Pay” and encouraging two friends or family members to do the same — read and get 2 more people you know and like to do the same!
Introduction & explanation of ten of my most politically important essays and historical documents
The following links lead readers to the best of 5 decades of my historical, political and legal research on the professions of medicine and midwifery, the biology of normal childbirth and the dysfunctional healthcare system that has burdened Americans for the last century.
I’m a lifelong reader and especially interested in history. As a new maternity nurse working the night shift, I read several early 20th century obstetrical textbooks (1904, 1912, 1924, 1937) by Dr. DeLee and Williams when we weren’t busy. When we were busy, it was my job to give our labor patients the massive amounts of narcotics drugs typical of the era that often caused such deep respiratory depression in their babies that it prevented them from breathing after they were born.
Several of our OBs didn’t like me, probably because I (foolishly) believed a mentally competent adult woman, even if pregnant (especially if pregnant!) had the right to refuse massive quantities of mind-altering Twilight Sleep drugs that depressed the respiration of their newborn — frequently repeated injections of narcotics and the amnesic and hallucinogenic drug scopolamine — and for speaking out about abusive obstetrical practices such as using 4-point leather wrist-restraints to keep narcotized labor patients from falling out of bed.
As a result, I got fired three different times. After 14 long and very frustrating years years as an agent for “knock’em-out, drag’em out obstetrics” I permanently retired from nursing and cross-trained into traditional midwifery.
A decade there was a knock at my door at noon on a Friday, and I found myself being handcuffed arrested in the presence of my youngest daughter, jailed and criminally charged with 5 counts of practicing medicine without license. This gave me a good reason to get real smart, real quick about the law and the legal system, the politics of organized medicine, the legislative history of midwifery in the United States and how our history was so dramatically different than the professional discipline of midwifery in Western Europe and other parts of the world.
Essay topics included but are not limited to:
My eldest grandson Devin, 1993
The historical and contemporary record of organized medicine (i.e. the AMA) century-long efforts to prevent any kind of national health insurance, which was denigrate and despised as “socialized medicine”.
This medical system doesn’t focus on keeping people from getting sick, since that is not what medical school prepares them for, and it would not be profitable to them. Seen from the perspective of the allopathic medical system, spending time on preventing (rather than treating) disease would be to a waste of their expensive medical education.
Instead, the allopathic profession used it political influence in 1910 (after publication of the Flexner Report written at the request of the AMA) to make the non-allopathic practice of medicine illegal.
This eliminated the legal practice of all the other (non-allopathic) “healing arts”, which included practitioners of naturopathy, osteopathy, homeopathy, and chiropractors. Organized medicine was able to be get state laws passed that criminalized the practice of other non-MD practitioners such as herbalists, midwives, and other types of non-medical healthcare providers.
Having eliminated pushback of any kind, MDs and hospital administrators created a “medical services delivery system” (MSDS), which is the most accurate description of our current dysfunctional so-called “healthcare” system which in fact is NOT care about keeping us healthy but waiting until we are sick.
The invention of elective hospitalization of healthy maternity patients by Dr. J. Whitridge Williams in 1910 as a new and profitable economic model for hospitals is still the standard of care for normal childbirth. This discussed fully in Post #5: “The Economic Story of American Hospitals: The invention of elective hospitalization in 1914, thus creating the economic engine for our private & corporate-owned American hospital system”.
Several more essays provide historic and contemporary background explaining why are current healthcare system is so profoundly dysfunctional. These include:
- The Debate on Health Care Policy Reform: An exercise in pseudo-journalism
- Time-traveler’s Perspective on Normal Childbirth
~ Faith Gibson, LM; published in the BIRTH Journal, Sept 2011 - Historical and Contemporary Comments by Doctors about Midwives: 1820 to 2019
- How Normal Childbirth Was Trapped on the Wrong Side of History
- The Economic Story of American Hospitals
- The Story of Man-Midwives: The Historical Tension Between Midwifery and Obstetrics During the 20th century
- The Official Plan to Eliminate the Midwifery Profession – 1900-1930
- The Wrong Use of Obstetrics: a story I hate to tell and no one should ever have to hear
- Mayday, Mayday, Mayday! A Call to Americans to fix a problem wasting millions of healthcare dollars & results in preventable maternal deaths (routine use of EFM on healthy women with normal pregnancies)
- The Dream, the Motives, the Methods & Enduring Impact of Dr. Williams 1914 book
“Twilight Sleep ~ Simple Discoveries in Painless Childbirth ~ Part 1 ~ Overview (with links to the rest of the series)

My more socially acceptable and modernized version of Mennonite Plain Dress
Enjoy!
Tell-A-Vision for the 21st Century
Editor’s Note: This is a very long essay – you might want to save it for later.
 My goal was to “connects up all the dots” in the complex and intergenerational story of how the American healthcare system was shaped by organized medicine to the great detriment to taxpayers and the ill, injured and disabled who most need its services. While this essay has important information on the pervasive (and very negative) influence of organized medicine on the American healthcare system, such a a long read requires an unhurried mindset.
My goal was to “connects up all the dots” in the complex and intergenerational story of how the American healthcare system was shaped by organized medicine to the great detriment to taxpayers and the ill, injured and disabled who most need its services. While this essay has important information on the pervasive (and very negative) influence of organized medicine on the American healthcare system, such a a long read requires an unhurried mindset.
1. The Debate on Health Care Policy Reform:
An exercise in pseudo-journalism
PDF version to print, read on your smart phone or tablet
This is a comprehensive (thus lengthy) essay that I wrote it in 2009 while the Affordable Care Act was being debated in the US Congress.
My subtitle “an exercise in pseudo-journalism” reflects my personal distress and disappointment at mainstream media, since it consistently failed to provide the critical information required for the kind of ‘public discourse’ that was so vital to crafting federal legislation that would actually be able to provide good health care while not breaking the bank. The basic needs is not a bigger pot of money, but a much more transparent and cost-effective system that operates within its reasonable budget, such as enjoyed by virtually every other developed country except for the United States.
I don’t know if the corporate-owned newspapers and cable news channels sold us out or if reporters just don’t understand, but day after day, all the major news programs did was repeat old news while never once mentioning the great big yellow and green-striped elephant in the middle of the room — that health and medical services cannot simultaneously be an ethical and humanitarian service while at the same time being profit-driven. Health-related care can be either one, but it can’t be both at the very same time.
The exceedingly powerful, century-long political influence of the AMA over state and federal legislation, and its total control over the practice of allopathic medicine, combined with our corporate-owned for-profit hospital system, the financial interests of big pharma and for-profit health insurance companies fundamentally sabotaged all legitimate attempts to craft a national healthcare system that could and would be fair, affordable, and therapeutically-effective.
Why did they do this? Because they were in business to make as much money as possible and when it comes to health and medical services, making a profit means providing as few services as you can possibly get away with while charging as much as you can possibly get away with.
The combined lobbying budget for these healthcare giants in 2009 was one million per DAY — each and every day, doled out to elected officials for to finance their re-election campaigns. Are we surprised that what we got was more of the same, only now Uncle Sam would become the middle man, collecting taxes from us and then giving some proportion of that tax money back to us taxpayers as payments to doctors and hospital for services we received.
This would not have been a bad thing if 90% of that money was used to pay fair market prices for these goods and services, while providing a nice 10% profit to the businesses and the practitioners who provided these services. This is NOT what is happening, as you will fully understand after reading “The Price We Pay“, but it can, should, and WILL BE CHANGED, by midwives and all those we can influence to join us and many other organizations.
 2. Time-traveler’s Perspective on Normal Childbirth: from 1910 to now
2. Time-traveler’s Perspective on Normal Childbirth: from 1910 to now
~ Journal BIRTH, Sept 2011 ~
BIRTH-PracPerspective_MyArticle_Sept11_2011
by Faith Gibson, LM,
3. Historical and Contemporary Comments
by Doctors about Midwives: 1820 to 2019
4. How Normal Childbirth Got
Trapped on the Wrong Side of History:
The last and most important UNTOLD story of the 20th century ~

The Perfect Storm that turned
healthy childbearing women
into the patients of a surgical specialty
and normal childbirth
into a surgical procedure
5. The Economic Story of American Hospitals:
The invention of elective hospitalization in 1914 (starting with healthy
maternity patients as paying customers), which created the economic engine for
our private &corporate-owned American hospital system

Unpublished &
unfinished manuscript
6. Man-Midwives
The Historical Tension
Between Midwifery and Obstetrics
During the 20th century
The Official Medical Plan to
Eliminate the Midwife: — 1900 -1930Part 1

7. The Official Plan to Eliminate the Midwife: 1900 to 1930
Based on the medical school thesis of Dr. Neal Devitt, MD
by faith gibson, LM
Excerpt of particular interest, not to be missed!
How doctors divide up the profession of midwifery between physicians and nurses:
~ “Of the 3 professions—namely, the physician, the trained nurse and the midwife, there should be no attempt to perpetuate the last named (midwife), as a separate profession. The midwife should never be regarded as a practitioner, since her only legitimate functions are those of a nurse, plus the attendance on normal deliveries when necessary.” [1915-A; EdgarMD p. 104]
The profession of midwifery was divided up between physicians and nurses, like taking a piece of whole cloth from midwives and tearing it into two unequal pieces. The biggest piece and the independent and high-paying end went to doctors and the smaller, subservient and low paying piece went to nurses.
The medical profession came up with a scheme to maximize their income by minimizing the time and energy they spent caring for their patient. This was to be achieved by having nurses do most everything but catch the baby (and collect a representational share of the fee).This scheme systematically exploited nurses by requiring them to provide almost all of the direct care required by the doctor’s hospitalized patients.
~ “The doctor must be enabled to get his money from small fees received from a much larger number of patients cared for under time-saving and strength-conserving conditions; he must do his work at the minimum expense to himself, and he must not be asked to do any work for which he is not paid the stipulated fee.
This means … the doctors must be relieved of all work that can be done by others —… nurses, midwives, social workers, and others.” [1922-A; ZieglerMD, p. 412]
~ “… {N}urses should be trained to do all the antepartum and postpartum work from both the doctors’ and nurses’ standpoint, with the doctors always available as consultants when things go wrong; and
…. midwives should be trained to do the work of the so called “practical nurses,” acting as assistants to the regular nurses and under their immediate direction and supervision, and to act as assistant- attendants upon women in labor—conducting the labor during the waiting period or until the doctor arrives, and assisting him during the delivery.”
~ “In this plan the work of the doctors would be limited to the delivery of patients, to consultant with the nurses, and to making of complete physical and obstetrical examinations … Under this arrangements the doctors would have to work together in a cooperative association with an equitable distribution of the work and earnings.” [1922-A; Ziegler, MD, p. 413]
8. The Wrong Use of Obstetrics:
a story I hate to tell and
no one should ever have to hear
A seven-part series on the dark history of obstetrics
that describes how the wrong use of obstetrics
became the standard of care for
healthy women starting in 1910

9. Mayday, Mayday, Mayday!
A Call to all Americans to fix a problem (universal use of EFM) wasting millions of healthcare dollars & results in preventable maternal deaths ~
Synopsis ~ Chapter 1A
Easy way to share this link: https://tinyurl.com/y5ojmvue
The first study of electronic fetal monitoring was a peer-reviewed controlled trial by Dr. Haverkamp published in 1976. At this time, just 20% of hospital had purchased EFM machines and they were only being used on women with very high-risk pregnancies.
The conclusions of the Haverkamp trial stated:
“There were no differences in the infant outcomes in any measured category between the electronically monitored group and the auscultated group. The cesarean section rate was markedly increased in the monitored group (16.5 vs. 6.8 per cent in the auscultated patients). The presumptive benefits of electronic fetal monitoring for improving fetal outcome were not found in this study.”
Haverkamp A., Thompson H., McFee J., Certulo C. (1976). The evaluation of continuous
fetal heart rate monitoring in high risk pregnancy. American Journal of Obstetrics
& Gynecology, 125(3), 310–320 [PubMed] [Google Scholar]
In the 46 years since that first electronic fetal monitoring study was published, literally hundreds of additional studies have been done. Many of these obstetrician-authors questioned Haverkamp’s conclusions and hoped to prove that continuous electronic fetal monitoring during labor was able to eliminate or at least substantially reduce the newborn neurological pathologies that doctors assumed were responsible for cerebral palsy and permanent brain damage in small children.
 Unfortunately for obstetricians who believed that continuous electronic fetal monitoring was the magic bullet that doctors had long been hoping for, the consensus of the scientific literature was virtually unchanged from Haverkamp’s 1976 conclusion — no difference, no benefit, increase detriment to the childbearing woman.
Unfortunately for obstetricians who believed that continuous electronic fetal monitoring was the magic bullet that doctors had long been hoping for, the consensus of the scientific literature was virtually unchanged from Haverkamp’s 1976 conclusion — no difference, no benefit, increase detriment to the childbearing woman.
However, these additional studies also had to admit that the one and only difference between the control group that used auscultation to monitor labor patient and the EFM arm of the study was a statistically significant increase in the rate of Cesarean surgeries in the women who had electronic fetal monitoring.
A example of this scientific consensus was published in 2011 in a professional OB-GYN journal by an obstetrician-author who began by explaining that:
“Despite the widespread use of EFM, there has been no decrease in cerebral palsy.
… meta-analysis of randomized control trials has shown that EFM has no effect in perinatal mortality or pediatric neurologic morbidity.2
However, EFM is associated with an increase in the rate of operative vaginal and cesarean deliveries.1”
Although intermittent fetal auscultation may be a theoretical option in low-risk patients, nursing staffing limitations makes this impractical … ”
Fetal Heart Rate Monitoring Update; The Female Patient, April 2011
Acknowledging the important contribution of auscultation
and its central role as the “control group” in studies of EFM
Each of these many studies compared routine use EFM outcomes against the routine use of auscultation. The conclusion of these peer-reviewed studies was that routine use of EFM had NO benefit for essentially healthy women with normal pregnancies.
The routine use of EFM over the last 5 decades has not reduced the CP rate by a even teeny tiny 1/10th of 1 percent — zip, zero, zilch, nada!
The only statistically significantly difference between auscultation and continuous EFM for this healthy population was substantial increase in the rate of Cesarean surgeries. What that means is that the use of EFM on healthy women dramatically increases their risk for all the well-known complications associated with Cesarean — intra-operative, post-op, delayed and downstream.
These complications can be life-threatening, break-the-bank expensive, and for a small subset of these mothers, fatal. Childbearing women — mothers all — actually die as a result of Cesarean complications that trance back directly to the unnecessary and inappropriate use of EFM.
Citation:
- Haverkamp A., Thompson H., McFee J., Certulo C. (1976). The evaluation of continuous fetal heart rate monitoring in high risk pregnancy. American Journal of Obstetrics & Gynecology, 125(3), 310–320 [PubMed] [Google Scholar]
Dr. J. Whitridge Williams, Professor of Obstetrics, Johns Hopkins University Hospital, 1900-1910; Dean of the JH School of Medicine 1911-23; author of the 1914 book “Twilight Sleep: Simple Discoveries in Painless Childbirth”.
10. The Dream, the Motives, the Methods & Enduring Impact of 1914 book
“Twilight Sleep ~ Simple Discoveries in Painless Childbirth ~
by Dr. Williams, the famous American obstetrician:
Part 1 ~ Overview

Link to the original 128-page book “Twilight Sleep: Simple Discoveries in Painless Childbirth”
Synopsis
Dr. J. Whitridge Williams, Professor of Obstetrics, Johns Hopkins University Hospital, 1901-1910; author of “Williams’ Obstetrics“, 1904; Dean of the JH School of Medicine 1911-23; author of the popular book “Twilight Sleep: Simple Discoveries in Painless Childbirth”, 1914 and single most influential obstetrician in the US during the early 20th century.
Dr. J. W. Williams’s big dream was a new nationwide system of general hospitals like the large publicly-funded regional hospitals all over Western Europe. At the time he graduated by medical school (1880s), clinical training was not available in the US. Coming from a wealthy family, he just sail to Europe and took two years of clinical training in obstetrics and pathology in the most famous hospitals on the Continent.
That experience made Dr. JWW acutely aware of the deficiencies in medical care our own country, which was that the US didn’t have any kind of hospital ‘system’. His vision was to find or to create a way to finance a system of general hospitals, coast to coast and in every population center with 3,000 or more inhabitants.
However, Dr. JWW knew all too well that the American Medical Association (AMA) would never accept this or any other kind of government funding in the United States, which the AMA fiercely despised as ‘socialized medicine‘. So he had to develop an economic plan that (a) would not use or depend on government funding, but nonetheless (b) would dependably generate the very large amount of money needed over many decades.
Dr. JWW financial plan began by inventing “elective hospitalization” — hospitalizing healthy patients as paying customers, in this case, healthy middle- and upper-class maternity patients. Part “B” of this plan consisted of urging every small and medium-sized hospitals all across America to immediately create new “lying-in” wards, using any empty rooms or unused spaces or to remodel and expand their facility.
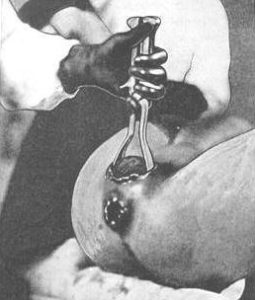
NOTE: ~ This baby is profoundly depressed — unconscious, totally flaccid and his umbilical cord that is no longer circulating oxygenated blood from the placenta — the effect of narcotics given to the mother during labor and general anesthesia for delivery
In conjunction with electively hospitalized maternity patients (the lying-in period for mother and baby was 14 days), this steady stream of healthy paying customers would generate a dependably profitable revenue stream that had no end, since women were always having babies. Thus was born step one of his economic plan for financing this massive, multi-generational undertaking that he hoped would outshine the centuries-old European system.
A new Economic Model for privately-owned hospitals specifically designed to be profitable
The implementation of Dr. Williams’ plan required a brand new economic model for hospitals that did not in any way depend on any government funding and yet could still provide a steady revenue stream. Up to this point, the typical hospital patient was very ill or injured, required a lot of nursing care, as well as supplies and medical or surgical procedures. After all this expensive care, some patients died without having paid their hospital bill. Imagine how the idea of “electively” hospitalize healthy patients (for x-rays, elective surgery or to have a baby) would dramatically change the financial status of hospital that previously were drowning in red ink.
Dr. Williams solution was to electively hospitalize healthy middle and upper-class white maternity patients as ‘paying customers’. Childbirth services for this demographic of healthy women were inexpensive to provide, since postpartum care mainly consisted of a clean bed, dry sheets and hot meals. In the early 1900s, “lying-in” patients were kept in the hospital for 14 days (i.e. the ‘lying-in period”), while their newly born babies were admitted to the hospital nursery. That meant the family of each maternity patient was billed for two daily room charges (one for mom, another for the baby) that generated 28 patient-census days.
Dr. Williams realized that the perfect type of patient to be electively hospitalized were healthy, middle & upper-class maternity patients whose family could afford to pay their doctor’s professional fee as well as a hospital bill. This reliably generated a profitable revenue stream for the hospital, a new income stream ear-marked for gradually expanding and upgrading the hospital’s facilities so five or ten years later the hospital to become a modern, full-equipped and well-staffed general hospital.
Formerly small hospitals (often with only 2 to 10 beds and very little medical equipment) were able to dramatically upgrade their status and standing in their community. As a general hospital, they could serve the full spectrum of medical and surgical needs for men and women of any age, babies and children, elderly adults, those that needed emergency care, x-rays, lab work, surgery, as well as childbirth services for women and nursery care for their newborns. It was an extra (but welcomed) bonus that each maternity patient convenient added another patient to the hospital daily census as her newborn baby was admitted to the hospital nursery
Dr. Williams’s plan began by encouraging small hospitals open new “lying-in”or expand their existing ward. Next they needed to join with other small hospitals in the area to finance a PR campaign promoting the idea that the new “modern” woman of means deserved to have the kind of “painless childbirth” and “blessed unconsciousness” only available in a hospital.
The goal and purpose in the elective hospitalization of healthy economically-enabled maternity patients was to create a new, profitable revenue stream was that would allowed tiny 2-to-10 bed hospitals all over the county expand their facilities by building a new surgical department with ceramic-tiled walls and big operating room lights, clinical labs, and a x-ray department, which also required the purchase of expensive, capital-intensive technological equipment like the newly invented x-ray machines, institutional sized autoclaves, microscopes and equipment and supplies required of the “modern” hospital.
This eventually turned those 8,000 one-room, 2-10 bed boutique hospitals formerly owned and run by one or two of the local doctors into a medium-sized ‘general’ hospital run by a hospital board. They quickly became part of a nationwide chain of medical institutions that were both equipped and staffed to meet the general medical, surgical, obstetrical, and pediatric needs of its citizens and to do so within reasonable driving time.
For the first time in our country’s history, the United States had the same kind of nationwide system of general hospitals as has been the standard for all most all European countries for more than a century.
Too bad that the cash cow for financing this system was (and to some extent remains) healthy maternity patients who were summarily narcotized with Twilight Sleep drugs for so-called “normal” labor, and then rendered unconscious by general anesthesia for a so-called “normal” birth that consisted of routine episiotomy, forceps delivery and manual removal of the placenta and suturing the perineal incision — all of this was done as an economic “work-around” to keep the AMA happy knowing that hospitals were not being contaminated by those nasty federal dollars.
God help us all!
