This link will make you laugh and then cry!
Check it out …
http://bornstroppy.com/bleeding-babies/
Backstory: How the routine use of general anesthesia triggered a race to ‘clamp-it-quick’ cord-cutting
For nearly a hundred years — most of the 20th century — the obstetrical profession has been in a ‘hair-on-fire’ hurry to clamp and cut the baby’s umbilical cord, lickity-split — 2 to 20 seconds — of the baby’s birth.
The reason for this lies in the early history of obstetrics in America, when the kind of traditional supportive care provided by midwives was defined as unscientific and old-fashioned. Between 1910 and 1920, doctors trained in the new ‘science’ of obstetrics as a surgical speciality took over the management of normal childbirth and moved all childbirth services into the labor and delivery wards of acute-care hospitals. Labor was defined as an potential medical emergency that was only be cured by the surgical procedure of operative delivery — a generous’ episiotomy, forceps, manual removal of the placenta, and lots of stitches to repair the episiotomy incision.
Knock’em-out, Drag-em-out Obstetrics ~ Laboring under the influence of narcotics, the amnesic-hallucinogenic drug scopolamine, chloroform anesthesia while flat on one’s back in an anti-gravitational position
Every laboring woman was routinely given Twilight Sleep drugs (sleeping pills, morphine and scopolamine) during labor; normal birth was conducted as a ‘surgical procedure’ to be ‘performed’ by a medical doctor after the mother was move to a special ‘delivery'(i.e. operating) room, put a special OR-type table, hands in leather wrist restraints, legs up in obstetrical stirrups, buried from the neck down under sterile sheets and then rendered unconscious under general anesthesia — ether or chloroform.
 Since the laboring mother was out cold, and also laying flat on her back, she couldn’t push very effectively, so forceps were routinely used to extract the baby from the mother’s inert body (what i often refer to as a ‘baby-ectomy’).
Since the laboring mother was out cold, and also laying flat on her back, she couldn’t push very effectively, so forceps were routinely used to extract the baby from the mother’s inert body (what i often refer to as a ‘baby-ectomy’).
Thus the apt description of “knock’em-out, drag’em-out” obstetrics.
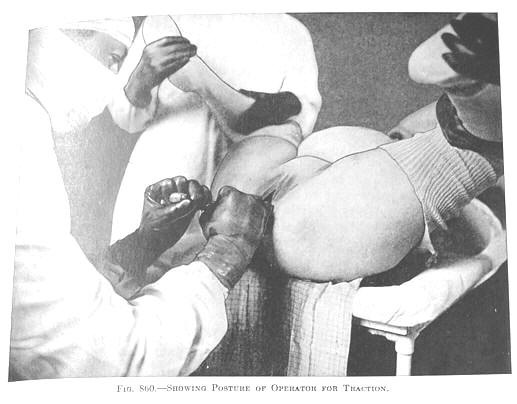
These doctors erroneously believed that forceps were safer and better for both mother and baby. They claimed that forceps sparred baby’s head from being used as a “battering-ram” being dashed against the mother’s “iron perineum”, while being delivered by forceps also sparring mother’s perineal floor from this assault.
Obstetrical books of the time (DeLee, 1924) describe ‘normal’ childbirth’ as so damaging to the mother’s perineum as to be equivalent of “falling on a pitch-fork“.
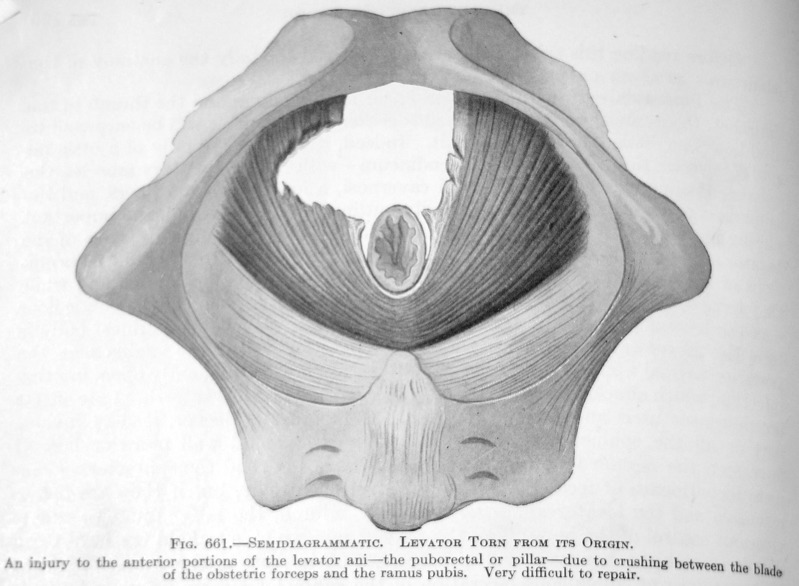
Tear in the muscular floor of the mother’s pelvis created by the misapplication of one of the blade’s of obstetrical forceps (photo & description from DeLee Principles of Obstetrics, 4th edition, 1924)
Unfortunate, neither imagined benefits turned out to be true, while the use of forceps often severely damaged the mother’s pelvic floor, resulting in organ prolapse and incontinence and often leading to a hysterectomy.
The routine use of forceps was also responsible for various types brain damage (such as cerebral palsy) in newborn babies.
One problem (apparently) solved, another created!
As the routine use of general anesthesia and forceps became the new standard for obstetrical care in the US, the profession found itself dealing with unexpected and unwanted side-effects of these highly medicalized births. The anesthesia given to the mother, especially when combined with the routine use of narcotics and scopolamine during labor, triggered a profound respiratory depression in her newborn — babies that were born limp, blue, not moving and didn’t begin to breathe spontaneously.
During this era of obstetrics (1900-1970s), OBs immediately held the newly-born baby upside down by the ankles and slapped him or her on backside to clear their airway and stimulate its first breath.
But on far too many occasions, intense resuscitative efforts by the doctor or nurse became necessary, such as briskly rubbing the baby’s body, providing oxygen, flicking the soles of its feet and in really desperate circumstances, inserting a finger into the baby’s rectum to shock the baby into breathing, etc. Unfortunately the efforts often proved futile, in which case the baby’s death was generally recorded as a ‘stillbirth’.
This was always an unpleasant experience for the doctor and nursing staff. But things got really upsetting when doctor had to tell family, who were all eagerly gathered in the waiting room to find if the baby had been born, and instead had to be told that the much-anticipated newborn son or daughter was dead. Worse yet was telling the mother when she awoke from the anesthesia and asked if she’d had a boy or a girl.

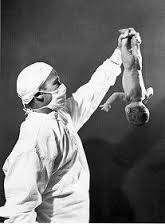
Severely-depressed, flaccid newborn being held by the obstetrician as the staff and anesthesiologist look on, while its mother is still unconscious under ether or chloroform
This emotionally-wrenching problem provided great incentive to reduce the amount of anesthetic gases transferred to the baby through its umbilical cord. Obviously, eliminating the routine use of general anesthesia during normal deliveries would have prevented this problem altogether, but at that time obstetricians did not see this as a desirable option.
Instead the raced to clamp and cut the cord, and fervently hoped they were quick enough that the baby would start breathing on its own and a potential catastrophe averted.
Newborn jaundice ~ the connection between immediate cord clamping and misguided efforts to reduce jaundice
I was an L&D nurse during the “Dark Ages of the Deep South, when ‘knock’em-out, drag’em-out obstetrics” was king-of-the hill. Standard hospital protocols required that we give all our patients Twilight Sleep drugs as soon as they were admitted to the labor room and general anesthesia was normally administered during childbirth, which was conducted as a the sterile surgical procedure.
When I quit working in the L&D of a big hospital Orlando, Florida in 1976, 95% of our labor patients were still giving birth under general anesthesia.
However a few lucky women — often those having a 6th, 7th or 8th baby — gave birth so quickly that the baby was born before the mother could be given the standard dose of narcotics drugs or anesthesia.
Long before I became a maternity nurse, doctors had already noticed that babies born ‘precipitously’ (i.e. umbilical cords were not immediately clamped) had more jaundice that those born under anesthesia, whose umbilical cords were quickly clamped and cut. We now know this normal jaundice of newborns is “physiologic” — that is, normal and to be expect but that was not the thinking in the 1920s. And now that knowing the blood type of pregnant women is part of routine prenatal care, we make a distinction between physiologic levels and newborns who have Rh incompatibility issue in which the mother’s blood type is negative and father’s is positive.
But in the 1920 and 1930, doctors believed that all newborn jaundice was a pathological condition that was the result of the baby having too much blood in its system. So they solved this ‘problem’ by declaring the standard of care to include immediately clamping and cutting of all umbilical cords during the first few seconds of the baby’s life.
This rapid clamping and cutting the newborn umbilical cords became a strategy with a dual purpose: First, it was to stop the transfer of anesthetic gases via the mother’s placenta into her baby, thus reducing the possibility that the neonate would suffer the most sever effects of respiratory depression – fatal suffocation at birth caused by the anesthetics given to its mother before and during the birth.
This was the original reason for “immediate” cord clamping. However, the benefits of this protocol was soon expanded to include reducing newborn jaundice in healthy neonates. This same quick clamping and cutting of the new baby’s umbilical cord was also to prevent the baby from having too much blood in its system and therefore becoming jaundiced.
What sad, maddening and convoluted story!
 Fix the “problem” by changing our minds and our vocabulary!
Fix the “problem” by changing our minds and our vocabulary!

“Immediate” clamping by hospital personnel is actually “premature” clamping; this is NOT a “best practice” except in those rare instances that the baby has untreated Rh incompatibility disease. Rh incompatibility is a mismatch between the blood of the mother and the blood of the fetus and occurs when the mother is Rh negative and the fetus is Rh positive.
What the mainstream medical profession pejoratively describes as “delayed” cord clamping, is the traditional standard of care for midwives and more properly described as “physiologic” cord clamping. Many family practice physicians and some obstetricians also practice ‘physiologic’ cord clamping and cutting.
The consequences of each
Immediate Cord Clamping:
The “immediate” clamping of umbilical cords is a preventable iatrogenic (medical-care related) complication that denies the baby from 20% to 50% of its own blood. That is like an adult being in an accident and suddenly loosing a couple pints of his or her blood. It causes physiological stress, which can become distress in many instance.
Babies with no medical issues usually cope OK with this and within 6 hours, and immediate effects of the blood lose/lower than normal blood volume become undetectable in scientifically-conducted studies.
 However, for premature babies and term newborns with fetal distress (such as a cord prolapse) or other medical complications, denying the baby approximately 1/3 of its own warm and oxygenated blood (100 cc out of a total of 240 cc), can result in physiological shock and death; for the luckier ones, it prevents weeks or even months in the NICU, which is extremely costly, both as stress for the family and economic expense to society.
However, for premature babies and term newborns with fetal distress (such as a cord prolapse) or other medical complications, denying the baby approximately 1/3 of its own warm and oxygenated blood (100 cc out of a total of 240 cc), can result in physiological shock and death; for the luckier ones, it prevents weeks or even months in the NICU, which is extremely costly, both as stress for the family and economic expense to society.
The “immediate” clamping of the newborn baby’s cord is an unnecessary intervention, one that unnecessary disrupts the normal transfer of the baby’s own oxygenated blood being carried back from the placenta via the baby intact umbilical cord with each beat of the baby’s heart. In this case, “immediate’ equals ‘premature’ and is a bad idea.
Birth attendants of all educational backgrounds and all birth setting should simply STOP prematurely clamping and cutting newborn cords and adopt physiologic clamping — hand off the cord until it becomes flaccid (smaller and paler) and stops pulsing (typically 3 to 6 minutes).
This is not hard to do. Its been many decades since laboring women were routinely given general anesthesia, so its very rare that quickly clamping the cord is needed to reduce the baby’s exposure to respiratory-depressing gases.
Likewise, the FDA approved RhoGAM in 1968, which has saved countless lives. Today, the standard of care is prophylactic or preventative: women who have negative blood types are given RhoGam early in the third trimester of pregnancy, so ‘premature’ clamping is rarely ever necessary for Rh negative mothers.
It’s such an easy and sensible (evidenced-based) change that I am mystified as to why the obstetrical profession continues to resist with such enthusiasm.
In conclusion, I say:
“Long live the ‘best practice‘ of leisurely clamping umbilical cords, here in the US and all around the world!