1A ~ Fetal Monitoring: Historic beginnings of America’s obstetrical conundrum — focus on the labor patient or stare at the EFM screen?
My husband, 7-year old daughter, me with my daughter newborn in my lap and my 5 yers old son, on a bench in front of Florida Hospital (Winter Park after the birth of my 3rd child on September 16, 1970
This series is dedicated to fixing a problem that wastes millions of healthcare dollars every year and results in preventable maternal death.
Continuous EFM has no benefit to mother or baby when routinely used on healthy women with low-risk pregnancies.
However, this expensive and yet ineffective obstetrical intervention has a very serious side-effect. EFM is associated with a significant increase in the C-section rate. Unfortunately, Cesarean surgery results in many more serious complications and a higher rate of maternal mortality than vaginal birth.
Based on the scientific literature, the acknowledged “best practice” and better choice for healthy childbearing women with normal pregnancies is ‘hands-on listening”, also known as auscultation. This means the L&D nurse or midwife personally monitors the unborn baby by listening to its heart rate on a regular schedule during active labor.
word count 2.500
The historic backdrop of our current conundrum
 For centuries, the obstetrical profession diligently searched for reliable ways to eliminate cerebral palsy (CP) and all similar neurological pathologies affecting newborn babies. In spite of many ‘miracles’ and ‘wonder drugs’ in other areas of modern medicine, and the successful launch of missiles into outer space carrying our astronauts, American doctors delivering babies in 1960s were no more able to predict or prevent babies being born with cerebral palsy or other permanent neurological disabilities than their counterparts in 1860.
For centuries, the obstetrical profession diligently searched for reliable ways to eliminate cerebral palsy (CP) and all similar neurological pathologies affecting newborn babies. In spite of many ‘miracles’ and ‘wonder drugs’ in other areas of modern medicine, and the successful launch of missiles into outer space carrying our astronauts, American doctors delivering babies in 1960s were no more able to predict or prevent babies being born with cerebral palsy or other permanent neurological disabilities than their counterparts in 1860.
When news of the first electronic fetal monitor was invented in 1958, American obstetricians were heartened, as they finally a good reason to believe they would soon get a nearly-perfect tool for preventing these birth-related tragedies. Unfortunately, it was more than a decade before the first continuous electronic monitor was ready for the real world.
In the meantime, the social distress for doctors that followed the birth of neurologically-damaged baby continued to depress obstetricians. As if that was not stressful enough, obstetricians were increasingly being named in malpractice lawsuit by its unfortunate parents. Worse yet, this trickle of litigation slowly turned into a flood after a US Supreme Court decision redefined the idea of a “community standard”.
1968 and much more than you ever wanted to know about the “Locality Rule”
For almost a century, the law that defined who was or was not allowed to give expert medical testimony in a malpractice case was defined by the “locality rule”, the result of an 1880 opinion in a Massachusetts case {Small v. Howard}. The locality rule required a physician to provide the same degree of skill and care as required of other physicians practicing in the same or similar community.
In medical negligence litigation, this placed a geographical dimension on the professional standard, since it limited the pool of medical experts to the same geographical area. This was a group of doctors often practiced at the same hospital, belonged to the county medical association, same country club, lived in the same neighborhood, had kids that went to the same schools.
When called to testify against their colleagues in malpractice cases, most physicians either declined to testify altogether or put an unbelievably positive spin on what in many cases was obviously negligent and incompetent actions or omissions. This made it really hard to win medical malpractice suits and most attorneys were not willing to waste their time on a “bad bet”.
 But in 1968, the Supreme Court overturned the locality rule in a landmark decision that recognized the entire medical profession as non-geographical entity of like-minded, similarly trained doctors.
But in 1968, the Supreme Court overturned the locality rule in a landmark decision that recognized the entire medical profession as non-geographical entity of like-minded, similarly trained doctors.
No matter where they lived in the country, the medical profession has, in legalese, become its own “community”. Now, plaintiff attorneys in New York could hire specialist doctors from as far away as California to serve as an expert medical witness.
Almost overnight, these new rules gave rise to a newly aggressive world of attorneys that could almost always find an MD somewhere in the United States that could and would (for a fee) testify that the doctor being sued had indeed violated the “community standard” for the competent practice of medicine. This usually meant winning their case and getting their one-third share of a big fat settlement from the malpractice carrier.
For obstetricians, this was devastating development, as they suddenly found themselves in the cross-hairs of an entire industry that was “out to get them” and yet, when the phone rang in the middle of the night, they had no choice but to get up and, ignoring the obvious the legal risks to themselves, trudge off to the hospital to attend a birth that might well be a ticking time bomb.
And in deed, the greater success of medical malpractice suit — greater in number and greater monetary awards — quickly got the attention of professional med-mal carriers, who turned around and started raising the premiums of doctors, particularly anesthesiology, orthopedists and obstetricians. This mounting crisis would boil over in the 1975 medical malpractice “crisis” in California and other parts of the country. American medicine would never be the same!
Obstetrics in the Post-Medical Malpractice Crisis World
By the 1970s, the obstetricians and their professional groups were looking to defend themselves from the obstetrical version of “ambulance chasing” lawyers. Their main strategy was do whatever was necessary to prevent malpractice lawsuits against them and the hospitals where they delivered babies. The idea of continuous electronic fetal monitoring, which provided a printed record of every minute of the mother’s labor — just in case they had to defend themselves — seemed to be an idea “whose time had come”.
New fetal monitoring technology & the plan to eliminate both cerebral palsy and malpractice suits

Officially, EFM is an obstetrical procedure that uses an electronic machine to continuously record the heartbeat of the fetus, matched with the frequency and length of the laboring mother’s contractions for the same period of time.
These two streams of data are simultaneously displayed on the monitor screen. Of course, this data is also recorded on moving graph paper, which creates a permanent legal record of the minute-by-minute status of the unborn baby’s health throughout the hours of labor and birth.
In the United State, the obstetrical protocol for c-EFM is to monitor every laboring woman continuously during the entire length of the labor and birth, no matter how healthy the mother or normal the pregnancy.
Greatly expanded use of Cesarean surgery ~ the 2nd half of this new obstetrical “miracle”
Electronic fetal monitoring itself was only half the answer the obstetrical profession was searching for. The equally critical second half was expedited operative delivery — the immediate use of forceps, vacuum extraction, or Cesarean surgery to rescue the unborn baby at the slightest hint of fetal distress as indicated by the EFM tracing.
 Continuous EFM, with its ability to gather critical information about the wellbeing of the fetus, was now paired with the ability of obstetrical surgeons to quickly extract the baby from the mother’s body, most usually via Cesarean surgery. This combination of electronic monitoring and expeditiously-performed Cesareans was considered by most of the obstetrical profession to be the answer to their prayer, a marriage made in heaven.
Continuous EFM, with its ability to gather critical information about the wellbeing of the fetus, was now paired with the ability of obstetrical surgeons to quickly extract the baby from the mother’s body, most usually via Cesarean surgery. This combination of electronic monitoring and expeditiously-performed Cesareans was considered by most of the obstetrical profession to be the answer to their prayer, a marriage made in heaven.
Educating the Public to Embrace the “brave new world” ~ and see continuous EFM as a miracle technology that eliminates newborn brain damage
Under these circumstances, it’s no surprise that the obstetrical profession aggressively and quite successfully promoted the combined use of these two complimentary obstetrical procedures. Obstetricians repeatedly assured the American public that the routine use of EFM, combined with the liberal use of Cesarean surgery at the slightest indication of any fetal distress, could and would eliminate neonatal brain-damaged during childbirth.
This was accompanied by the obstetrical profession’s assumption that all babies should be born in an acute-care hospital setting under obstetrical management. The sub-text of this — sometimes verbalized, sometimes not, but always present below the surface — was the not-at-subtle inference that failure to hospitalize all laboring women for whatever reason, no matter how healthy, or any failure of the institution (hospital or birth center) to electronically-monitor the entire labor, represented obstetrical neglect.

Mother admitted for induction, IV started
The historical context behind this modern phenomenon is instructive. The 20th century history of American obstetrics is paved with other frequently used obstetrical interventions that became the standard of care without any scientific evidence that their benefit far outweighed an harm associated with their use.
During this period of time, obstetrical textbooks published in the US actually defined normal childbirth as a ‘patho-physiology‘ — that is, a biologically natural process that was fundamentally harmful (i.e. pathological).
This includes routine use of episiotomies(1910) and forceps (1920), elective induction of labor (1950s) and the liberal and/or elective use of Cesarean section 1990s. These interventions were seen as making up for the design flaws believed by the obstetrical profession to be a normal facet of female reproductive biology.
Biology as “destiny” — deep history of gender bias as it influenced the thinking of obstetricians
For the past hundred-plus years, there has been a strong (but very wrong) assumption in the United States that normal childbirth inevitably risks the life of unborn babies and regularly damages the pelvic floor of childbearing women. In the first decades of the 20th century, this negative view of normal childbirth perfectly fit the perspective of the newly emerging obstetrical profession, who mainly dealt with unhealthy mothers and complicated situations.
As noted earlier, obstetrical professors of that era authoritatively described pregnancy as a nine-month disease that required a surgical cure. This referred to childbirth-related damage to the new mother and/or her newborn that were not uncommon, However, there were many reasons for these problem, including malnutritions, lack of appropriate care and often, iatrogenic harm caused by the poor obstetrical practices of the day.
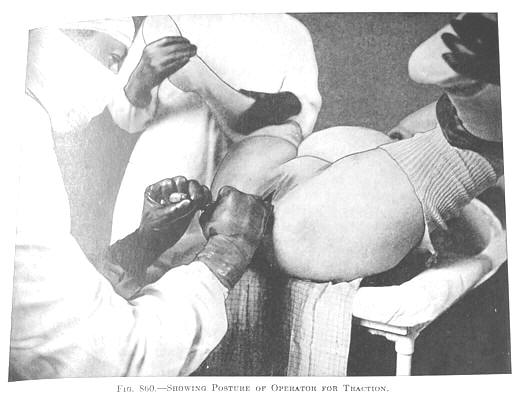
First-time mothers, in particular, had soft tissue bruising and what midwives describe as skid marks perineal laceration that required suturing. Dr. DeLee, one of the two Titans of American obstetrics in the early 20th century mocked the idea of childbirth as a normal aspect of biology, describing the ‘inevitable’ damage to the mother’s perineum to be a “normal as falling on a pitchfork”. Likewise, he believed that unborn babies suffered possible brain damage every time their mothers pushed, which repeatedly battered their delicate head against the unyielding obstruction of their mother’s intact, or as DeLee described it, her “iron perineum”.
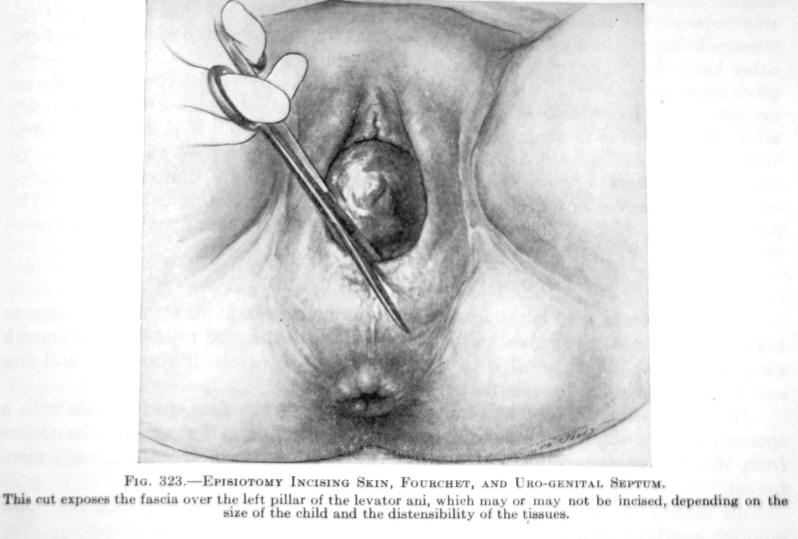 The obvious “cure” for the pernicious nature of Iron Perineums and Fetal Battering Rams was, of course, routine episiotomy, and in many cases,
The obvious “cure” for the pernicious nature of Iron Perineums and Fetal Battering Rams was, of course, routine episiotomy, and in many cases,
Female Troubles: Mother Nature or poor obstetrical practices or ?
In addition to the pain, mothers were assumed to suffer from to “falling on a pitchfork”, there was trauma inflicted on the unborn baby from battering its “head against its mother iron perineum”, there was the gnarly issue of the mother’s pelvic floor and pelvic organs.
 Obstetricians, we convinced this double-barreled assault on the mother’s pelvic floor was the origin of the ‘female troubles’ so many women complained of later in life. If questions about these assumptions I’m 99.44% sure they’d say:
Obstetricians, we convinced this double-barreled assault on the mother’s pelvic floor was the origin of the ‘female troubles’ so many women complained of later in life. If questions about these assumptions I’m 99.44% sure they’d say:
“I see this happening right before my eyes, how could I believe otherwise?”
To the mind of obstetrically-trained doctors in the US system (which purposefully excluded midwifery), this justified the use any or all obstetrical interventions that would rescue innocent mothers and babies from the horrific damage of vaginal birth.
Unfortunately, the medical profession did not see the connection in women btw injured during obstetrical managed births and development of “female troubles”, especially the many unnatural interventions used during a so-called ‘normal’ birth, most especially routine use of episiotomies and forceps.
Iatrogenic Harm: Unrecognized and Unacknowledged
 |
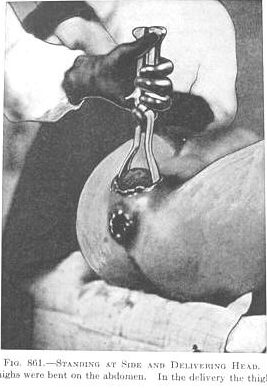 |
Fig 661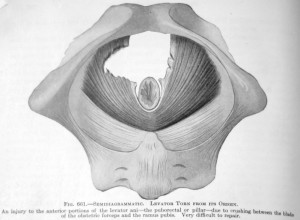 |
Fig. 661
1924 edition of DeLee’s Principles & Practice of Obstetrics: “An injury to the anterior position of the levator ani due to crushing from the blade of the obstetric forceps and the ramus pubis. Very difficult to repair”. |
Nature’s inadequacies vs. consequence of iatrogenic Interference
Few people — doctors, patients or the American public — realized that so-called “biological weakness” of the female gender in America was so very often the result of unwise or unnecessary iatrogenic interventions that, which intended to heap, were instead harmful.
As a result, deep pelvic and perineal nerves were frequently damaged and supporting ligaments torn when obstetrical forceps sliced through the musculature of the mother’s pelvic floor, as illustrated in the accompanying graphic above (Fig. 661). This left behind a host of other physical problems including fistulas and life-long incontinence. Nor does this take into account the same kind of damage to the baby‘s head, face, ears, and (of course), its brain.
But from the perspective of a late 19th and early 20th-century male physician, it seemed that a woman’s reproductive biology was God’s mistake when compared to the biology of a man. For the male of the species, sexual reproduction never resulted in his death (except being shot by a jealous lover!) or physical damage to the man’s sexual organs, whereas women could be harmed or die from the complications of pregnancy and childbirth.
This supposed biological inequality was just one more brick in the wall that divided the sexes and resulted in an assumption that men were the ‘perfected’ half of the human species, while the female gender was the biologically and psychologically inferior half — nature’s mistake.
As for the newborn baby, doctors saw the pathophysiology of the female gender as making childbirth so hard on the fetus that newborn babies were often too tired to breathe and so they died or suffered a variety of birth injuries that might leave them physically or mentally handicapped for life.
Given the facts of this obstetrical perspective, the much higher C-section rate associated with EFM is was seen an unexpected benefit for women, as Cesarean delivery was the only sure way to save new mothers from developing ‘female troubles’.
21st Century Interventionist Obstetrics seen as “normal” by the public
At this point in our history, the American public generally accepts our highly medicalized childbirth system as a welcome status quo — a wonderful use of the most modern and cutting edge technology to make life better for everyone. People don’t question our highly-medicalized obstetrical system any more than they wonder if telephones, personal computers, and air travel are a ‘good’ thing.
Are these assumptions about c-EFM & liberal use of C-section actually born out by the scientific literature?
- Does the research actually identify the routine use of continuous EFM as the universal standard of care and associated liberal use of Cesarean surgery as substantially reducing neurological problems in newborns when compared to simpler methods of intrapartum monitoring?
- Has medical science discovered reasons other than the management of the labor and birth that explain why some apparently normal birth result in CP and similar problems?
- As for preventing ‘female problems’, no one wants new mothers to become incontinent or suffer pelvic damage as a result of childbirth, but does the high rate of Cesarean surgery in the US reliably prevent those problems?
Since c-EFM and elective Cesarean delivery were both incorporated into the American standard of obstetrical care in the 1980s, one world assumes the answer is “yes”.
 Interestingly enough, the obstetrical profession’s own research, as published in its own peer-reviewed journals says “no” to both of the supposed ‘cures’ for CP and other imagined benefits of c-EFM and liberal use of Cesarean.
Interestingly enough, the obstetrical profession’s own research, as published in its own peer-reviewed journals says “no” to both of the supposed ‘cures’ for CP and other imagined benefits of c-EFM and liberal use of Cesarean.
In fact, scientific studies identify many of the routine obstetrical practices associated with our highly medicalized model of childbirth to make matters worse for families and society when the unproductive expense is taken into account and the increase in medically-unnecessary operative deliveries and their well-documented complications and increased maternal mortality rate.
