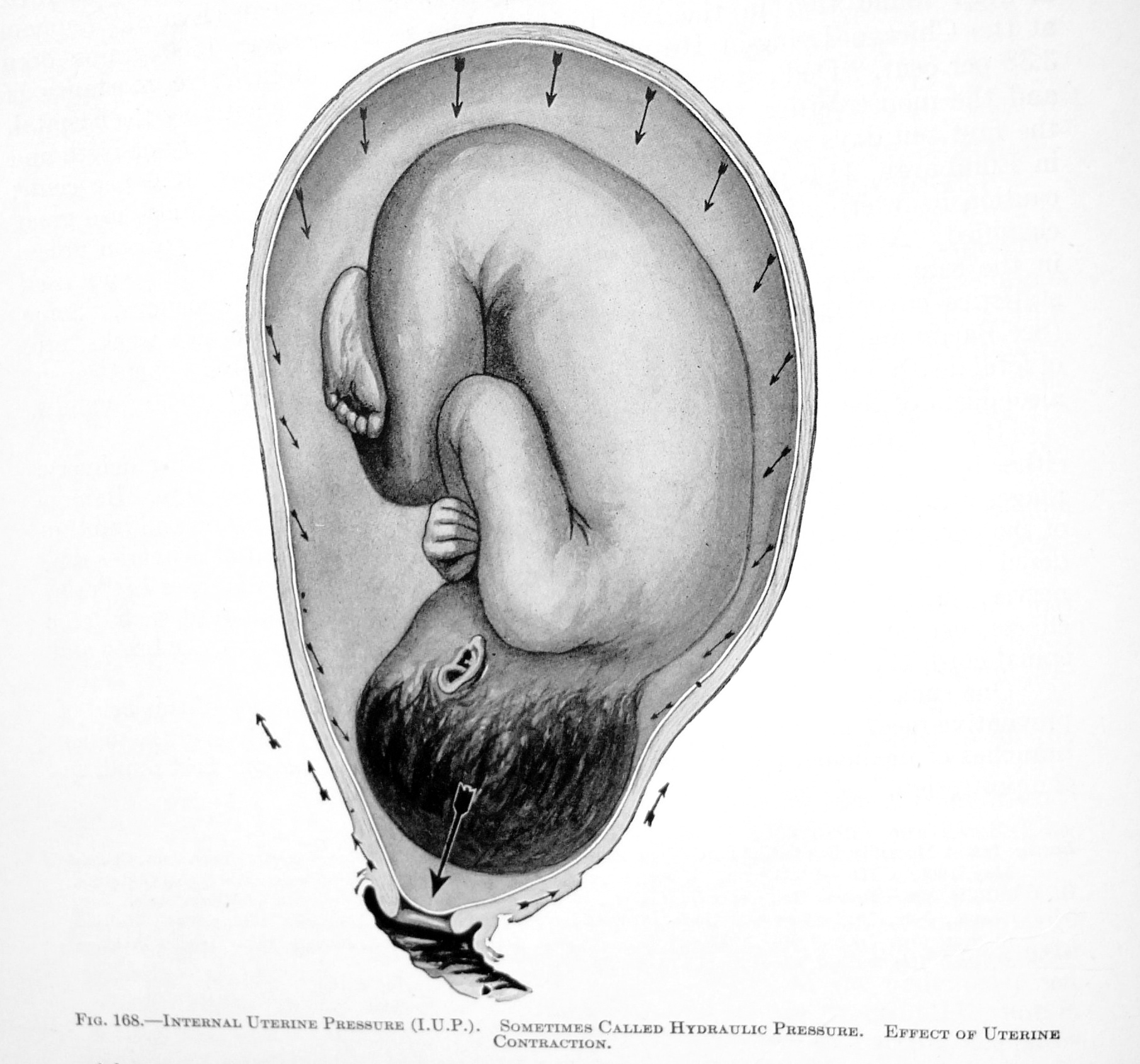
In the Beginning . . . .
 Let me begin this chapter by restating the obvious: My critique of the obstetrical profession is ONLY relative to historical and contemporary excesses and its institutionalized poor practices. Examples include the historical rejection of hand-washing by 19th-century doctors after aseptic principles were established to prevent maternal and neonatal deaths from childbed fever.
Let me begin this chapter by restating the obvious: My critique of the obstetrical profession is ONLY relative to historical and contemporary excesses and its institutionalized poor practices. Examples include the historical rejection of hand-washing by 19th-century doctors after aseptic principles were established to prevent maternal and neonatal deaths from childbed fever.
An issue closer to home is the decision made in the early 1900s to normalize a highly medicalized model of obstetrical interventions as the American standard of care for healthy women with normal pregnancies. The drugs, medical treatments and surgical techniques being used on healthy women were originally developed to treat women with serious complications. From the standpoint of evidence-based science, they were not meant to be used preemptively as a routine policy.
Treating complications and emergencies is the right use of obstetrical medicine — a ‘best practice’. This is also the most efficient and cost-effective use of healthcare resources. While iatrogenic or nosocomial complications can still occur as a result of any type of medical interventions (mistakes, drug reaction, a hospital-acquired infection, etc) these secondary complications are a reasonable price to pay when mother or baby (or both) would otherwise suffer life-threatening consequences.
The ‘right use’ of the surgical specialty of the obstetrics is one of the ‘modern miracles’ of 20th and 21st century, for which we are all appreciative. I wish that aspect of the story were the whole story but sadly, it is not. Nonetheless, I’m not suggesting (nor would I support) the notion of throwing the baby out with the bathwater.
Obstetrics is here to stay, which is how it should be. I and other midwives look forward to a time when the obstetrical profession can say the same thing about midwives. Developing cooperative, mutually complimentary relationships between our two professions will benefit all parties — especially childbearing women and their families.
 Returning to the topic ~ the history of obstetrics & its association with preventable maternal deaths:
Returning to the topic ~ the history of obstetrics & its association with preventable maternal deaths:
Maternal mortality in the United States was at its lowest point in 1982 – 8 deaths per 100,000 live births — where it remained stable for the next 14 years. Then in 1996, the MMR began to increased and within 11 years (2007 is the last year finalized statistics for MMR were published) the number of maternal death had increased to 14 new per 100 K.
A significant portion of the current increase in maternal mortality and morbidity in the US can be directly traced to the pattern of invasive and interventive obstetrical practices promoted and normalized by the obstetrical profession over the course of the twentieth century.
This way of thinking started with the infamous “knock’em out, drag’em out” obstetrics. Thankfully contemporary obstetrics quit using Twilight Sleep drugs and outlet forceps 30 years ago, but now the excess du jour is a hugely disproportionate increase in medically unnecessary inductions and the ‘liberal’ (therefore mounting!) use of Cesarean surgery.
While it is true that American mothers are giving birth for the first time at a slightly older age, and many are heavier, even obese, a statistical analysis of the percentage of these interventions for each individual age group shows a continuing and equally proportionate rise in the ratio of inductions, other interventions and cesarean sections — that is, the increased number of Cesarean sections is similar for younger women as it is for older women, which means the issue is the obstetrical system, not some imagined defect in the biology of childbearing women.
 The decisions made a hundred years ago that defined healthy women to be surgical patients, and normal childbirth to be a series of surgical procedures, were based on the ‘authority’ model of medicine (the opinion of ‘experts’) instead of today’s scientific model of research-validated evidence. What was the most profound change in childbirth practices in the history of the human species was universally adopted without any prior research?
The decisions made a hundred years ago that defined healthy women to be surgical patients, and normal childbirth to be a series of surgical procedures, were based on the ‘authority’ model of medicine (the opinion of ‘experts’) instead of today’s scientific model of research-validated evidence. What was the most profound change in childbirth practices in the history of the human species was universally adopted without any prior research?
No clinical studies were ever conducted by the medical profession or side-by-side comparisons of the daily or routine care provided by the two systems.
The first and traditional model is physiologic (i.e., non-medical, non-surgical) management of normal labor and birth in healthy women that included support by family members and the medically-appropriate transfer of care as indicated.
This is in contrast to the standard obstetrical model of labor and birth. Protocols for labor started with total social isolation (no family members allowed during the entire labor, birth, and recovery) and a host of routine medical interventions.
This started with the public prep — shaving the mother’s pubic hair — and admission enema, followed by sequential injections of narcotics and Twilight Sleep drug scopolamine every 2 – 3 hours. So-called “normal birth was a series of routine surgical procedures performed under general anesthesia on unconscious women.
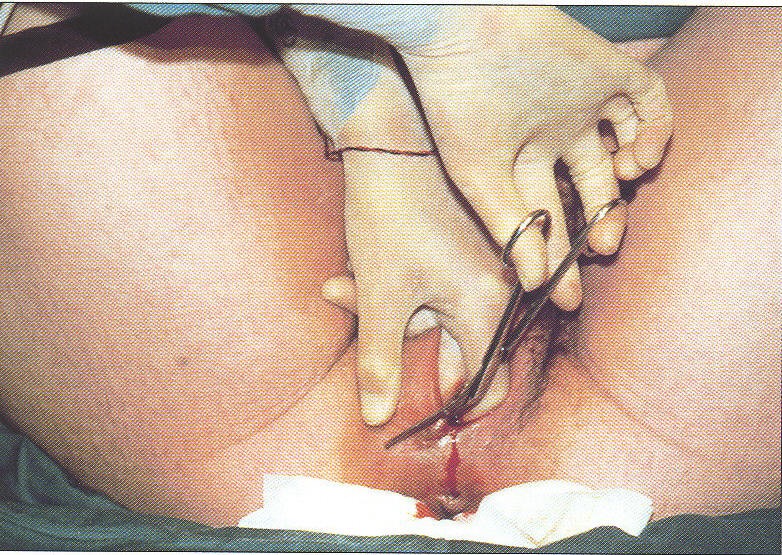
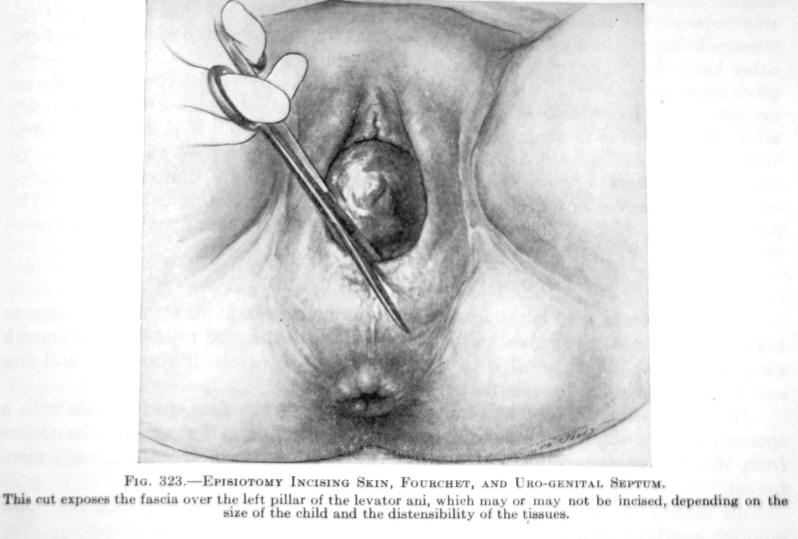 This included a ‘generous’ episiotomy, routine use of outlet forceps, manual removal of the placenta and suturing of episiotomy wound, including the famous “husband stitch”.
This included a ‘generous’ episiotomy, routine use of outlet forceps, manual removal of the placenta and suturing of episiotomy wound, including the famous “husband stitch”.
This was explained to me as a response by obstetricians to a complaint made in the distant past when a husband expressed sexual displeasure, saying “ever since my wife gave birth, having sex with her is like walking into a warm room”. The “husband stitch’ was to return the postpartum woman’s vagina to virtual virginity.
The intellectual leaders of the ‘new obstetrics’ did not draw on a statistical analysis of various types of maternity care from health records in the US or in Western Europe, where Scandinavian countries and the UK had very sophisticated maternity care systems, some with excellent records going back as far as the late 1700s.
Nonetheless, policies were implemented in hospitals all across America making the surgical specialty of obstetrics the standard for healthy women — a decision promoted with incredible enthusiasm by organized medicine. This propaganda campaign misrepresented the nature of normal childbirth as profoundly pathological — a “nine-month disease that requires a surgical cure”.
This ignored, or at least failed to appreciate, that the greatest source of pregnancy and childbirth-related dangers were associated with:
- extreme poverty
- nutritional deprivation
- unhealthy living or working conditions
- no access to family planning services
- lack of public sanitation.

For the childbearing population, this frequently included a large number of closely-spaced pregnancies in overworked and underfed women, unattended births and lack of access to emergent care when mother or baby needed it most. And this was taking place 30 years before antibiotic drugs were developed and became available in the US.
At the same time, the PR campaign by organized medicine inflated the abilities of the obstetrical profession to eliminate all childbirth-related problems as their system ignored the socio-economic and public health aspect of these problems. Instead of preventing problem pregnancies, they found themselves riding in like a knight on a white horse to rescue severely compromised women from life-threatening complications.
 More Intervention as ‘More Better’
More Intervention as ‘More Better’
The idea that more intervention was ‘more better’ originated in 1910, when obstetrics as a new surgical specialty formally declared that ‘modern’ childbirth should be conducted as a surgical procedure to be performed by doctors on anesthetized women, thus making healthy women into the patients of a hospital-based surgical specialty.
~ “For the sake of the lay members [attending this meeting] who may not be familiar with modern obstetric procedures, it may be informing to say that care furnished during childbirth is now considered, in intelligent communities, a surgical procedure.“ [1911-d, TASSPIM – page 214]
~ ” ….. the ideal obstetrician is not a man-midwife, but a broad scientific man, with a surgical training, who is prepared to cope with most serious clinical responsibilities, and at the same time is interested in extending our field of knowledge.
No longer would we hear physicians say that they cannot understand how an intelligent man can take up obstetrics, which they regard as about as serious an occupation as a terrier dog sitting before a rat hole waiting for the rat to escape.“1911-B; J. Whitridge Williams, M.D.
... The conduct of labor is not a simple matter, safely entrusted to everyone. Let the people know that having a child is an important affair, deserving of the deepest solicitation on the part of the friends, needs the watchful attention of a qualified practitioner and that the care of even a normal confinement is worthy the dignity of the greatest surgeon. [De Lee obstetrical textbook; 4th edition, 1924, p. 341]
 This campaign simultaneously included a holy war against physiologic childbirth and anyone (physician or midwife) who promoted spontaneous childbirth. Dr. J. Whitridge William, famous and influential American obstetrician and one of the founding fathers of 20th-century obstetrics, dismissed the normal biology of birth as a major nuisance to his plans to develop obstetrics as a surgical specialty, saying:
This campaign simultaneously included a holy war against physiologic childbirth and anyone (physician or midwife) who promoted spontaneous childbirth. Dr. J. Whitridge William, famous and influential American obstetrician and one of the founding fathers of 20th-century obstetrics, dismissed the normal biology of birth as a major nuisance to his plans to develop obstetrics as a surgical specialty, saying:
“That word ‘physiological‘ has all along stood as a barrier in the way of progress”.
Dr. De Lee, the other “Titian” and founding father of early 20th obstetrics in America, held a similar opinion. In the sentence below Dr. De Lee quotes a 19th-century physician-anthropologist by the name of Engelman, and scoffs at what both doctors considered to be the dangerous “prejudice” of childbirth as a normal biological act:
“Engelman says: ‘The parturient suffers under the old prejudice that labor is a physiologic act’ . . .
. . . the profession entertains the same prejudice, while as a matter of fact, obstetrics has great pathologic dignity —it is a major science, of the same rank as surgery“. [1915-C; DeLeeMD p. 116]
“If the profession would realize that parturition, viewed with modern eyes, is no longer a normal function, but that it has imposing pathologic dignity, the midwife would be impossible of mention.” [1915-C; DeLeeMD p.117]
As a result of the preferences and policies of influential obstetricians during this seminal period time in the development of ‘modern’ medicine, medical schools stopped teaching the physiological principles of normal childbirth early in the 20th century.
 Medical students, interns, and obstetrical residents have never been exposed to these biological norms for the entire 20th century, either to see for themselves as a part of their normal life experience, or as part of the medical school’s curriculum or their own clinical training.
Medical students, interns, and obstetrical residents have never been exposed to these biological norms for the entire 20th century, either to see for themselves as a part of their normal life experience, or as part of the medical school’s curriculum or their own clinical training.
The goal was universal acceptance of the obstetrical model as the standard of care for the entire childbearing population. However, this would remain elusive as long as a competing narrative was being kept alive by birth attendants who were still providing the vile ‘physiological’ form of care.
A vital prerequisite to the success of the ‘new obstetrics; was identifying a reliable way to rid the country of these competing ideas and its practitioners. In the quote below, Dr. De Lee addresses a question from a colleague on how to “elevate the public conscience”, as organized medicine preferred to call their public relations (i.e., propaganda) campaign:
“How can this be done? Let us begin with the Women’s Clubs in the United States. The Woman’s Clubs in the US are an enormous power, and they are growing more powerful in the civil and social betterment of this country.
If we can disseminate among the women of our land the facts regarding obstetrics, there will rise an undeniable clamor for good obstetrics. The public will be forced to furnish the materials, and the patients [i.e., teaching cases] for the proper instruction of the doctors. They will build maternity hospitals the equal, if not the superior of any surgical hospital.” [1911-B; Dr. De Lee, MD]
When public opinion has thus been raised and educated regarding obstetrics, the midwife question will solve itself. With an enlightened knowledge of the importance of obstetrical art, its high ideals, the midwife will disappear, she will have become intolerable and impossible.” [1911-B; R. De Lee, M.D.]
 In the 102 years since these policy decisions were implemented, many of the core beliefs and prejudice against physiologically-based care have never been officially reevaluated. Medical schools still don’t educate their students in physiologic principles. In general, hospital obstetrical departments still have not implemented policies that support physiological childbirth as the norm and eliminated the medically-unnecessary use of practices and protocols that disrupt the spontaneous processes of labor and birth.
In the 102 years since these policy decisions were implemented, many of the core beliefs and prejudice against physiologically-based care have never been officially reevaluated. Medical schools still don’t educate their students in physiologic principles. In general, hospital obstetrical departments still have not implemented policies that support physiological childbirth as the norm and eliminated the medically-unnecessary use of practices and protocols that disrupt the spontaneous processes of labor and birth.
Continuing medical education seminars do not teach physiological management as a normal part of updating medical knowledge. The medico-legal situation, which determines the ‘customary’ practice of obstetrics, functionally defines obstetricians who use physiological management as providing sub-standard care by virtue of his or her ‘failure’ to preemptively use the medical and surgical interventions that constitute the standard of care for a surgical discipline of obstetrics.
 In spite of continuing and on-going requests from healthy women to the obstetrical profession to offer normalized (non-medical) care for normal childbirth, the necessary elements to do that – access to physiologically-based management of normal labor and birth – have been uniformly eliminated from the picture. Non-medicalized childbirth practices are not even an option in most hospitals, while out-0f-hospitals choices are few, restrictive and controversial.
In spite of continuing and on-going requests from healthy women to the obstetrical profession to offer normalized (non-medical) care for normal childbirth, the necessary elements to do that – access to physiologically-based management of normal labor and birth – have been uniformly eliminated from the picture. Non-medicalized childbirth practices are not even an option in most hospitals, while out-0f-hospitals choices are few, restrictive and controversial.
Major Changes in the Wrong Direction:
The most startling part of the contemporary story is that each passing decade is marked by an ever-growing number of ‘must-have’ technologies and ‘must use’ procedures. New interventions are just piled on top of the older ones, and all of them are applied at an earlier stage of labor (or in pregnancy, such as scheduling routine induction of labor at 40 weeks) and to a larger proportion of childbearing women without ever re-evaluating any of these ideas, policies, protocols, technologies or interventions.
In the military, this is called ‘mission creep’, only for obstetrics the speed it’s more of a gallop!
 The 21st standard of care for a remarkably healthy (often wealthy) population of American women combines continuous electronic fetal monitor as routine for normal labor, epidurals for pain relief, the artificial hormone Pitocin to speed up labor, and the liberal use of Cesarean section anytime there is a worrisome blip on the EFM.
The 21st standard of care for a remarkably healthy (often wealthy) population of American women combines continuous electronic fetal monitor as routine for normal labor, epidurals for pain relief, the artificial hormone Pitocin to speed up labor, and the liberal use of Cesarean section anytime there is a worrisome blip on the EFM.
Many in the obstetrical profession continue to believe that C-section surgery is better and safer for babies (it isn’t) and that it prevents pelvic floor disorders in their mothers (it doesn’t). It does however increase maternal mortality.
The physician-journalist Dr. Atul Gawande, in his famous 2006 New Yorker article on the ‘industrialization’ of childbirth, glowingly describes the contemporary, super-sized model of medicalized practices as “the obstetrical package”. Then he goes on to define obstetrics for healthy women as medicine’s single most effective and important contribution to the history of the modern world.
Central to the ‘obstetrical package’ is the casual use of Cesarean. However, the association between sky-rocketing operative rates and nearly doubling of maternal mortality, plus a big spike in the rates of maternal morbidity (such as emergency hysterectomies to stop intra-operative or post-op maternal hemorrhage) is either ignored or attributed to (you guessed it) older, fatter, less healthy moms and teenage mothers on crack. Surely it couldn’t be anything that doctors are doing.
In the era of Dr. Semmelweis (1830-1860s), he fought to get physicians to take responsibility for the pathogens (germs) they were carrying from autopsy ward to the labor ward. He needed them to realize that the horrible fatal infection of childbed fever could be prevented if doctors and medical students would take hand-washing seriously and dip their ungloved hands in a germicide such as weak bleach water solution as they entered the labor ward and between doing vaginal exams of laboring women.
However, this simple request was flatly rejected by his obstetrician colleagues. In fact, they were incensed by the idea that they might somehow be held responsible for maternal-infant mortality from childbirth septicemia. For decades after this simple prophylactic protocol was known to be effective, the unified response of the medical profession was to say:
“Doctors are gentlemen and gentlemen’s hands are always clean.”
Apparently, the obstetrical profession favors the ostrich position, with its collective head in the sand whenever they are challenged by uncomfortable facts.
 Obstetrical accountability-responsibility for the perpetuation of unscientific practices
Obstetrical accountability-responsibility for the perpetuation of unscientific practices
Disturbing as this story is, it is not the first time that childbearing women and their infants have been victimized by the very process that was supposed to be protecting them. This current romance with intervention and operative delivery is the third prolonged episode of iatrogenic and nosocomial mortality in the obstetrical field during the last 170 years.
My personal goal is simply to be sure that history does not continue to repeat itself. My purpose in telling this sad story is the hope it will help bring the current episode to a close in the very immediate future. Without fully information and organized ‘push-back’, we remain at the mercy of obstetric’s slow-motion/no-motion time-frame.
That means 20, 30, 40 or more years AFTER obsolete obstetrical practices have been scientifically identified to be not-helpful, harmful or at best neutral but not-cost-efficient, this package of obsolesce will still be lawfully defined in the United States as ‘customary practice’ and will remain an obligatory part the obstetrical standard.
Equally outrageous is that any obstetrician who independently dares to diverge from these substandard practices (many of which are considered negligent or incompetent in other parts of the world) risks being sued for his ‘failure’ to abide by the irrational but nonetheless legally defined standard of care. This physician could easily lose his hospital privileges and thus his livelihood — all for doing the right thing.
We can’t let the obstetrical profession define glacial speeds (lack of alacrity!) as their professional norm. We can let that happen again.
@-@ -@-@
-@-@
To make reading easier, I posted an ‘aside’ about the 1950-1990s part of the story. If you want to ‘read more’, click on this link.
Otherwise, you can go straight to part 3, using the link below and the story will still make sense.
Continue part 3 – Three Strikes and You’re Out
