*NOTE: AASPIM is for the “American Association for the Study and Prevention of Infant Mortality”. This was a professional organization of obstetricians and other MDs and public health officials that met annually from 1910 to 1923. It was originally organized, financed, and backed by the AMA.
The previous post — Part One — provided the necessary background of obstetrics in America as it was crafted by Dr. J. Whitridge Williams (the single most influential American obstetrician of the 20th century) and his politically-active contemporaries. A uniquely Americanized form of obstetrics that was different and distinct from the classical discipline began in 1910, with the first annual meetings of the AASPIM (arranged and financially backed by the American Medical Association).
Over the next ten years, a plan was implemented that simultaneously dismantled the historical maternity care system in the United States by making it a crime (illegal practice of medicine) for midwives to attend births and launching a hospital-based obstetrical system that would conduct normal childbirth in healthy women as series of medical and surgical procedures.
Instead of normal childbirth in essentially healthy women being attended by experienced midwives and general practice physicians in the family’s home, all laboring women would be electively hospitalized as soon as they were in labor, medicated with morphine and the Twilight Sleep drug scopolamine, and delivered under general anesthesia. This included the routine use of episiotomy, forceps extraction of the baby, and manual removal of the placenta.
Bad News gets a whole lot worse!
The idea of having virtually 100% of all childbearing women
The bad news is that the
Since this was several decades before antibiotic drugs were discovered (sulfa 1937, penicillin 1945), the maternal mortality rate went through the roof, with a MMR as high as 25,000 annually. Ten thousand of those deaths were the direct result of postpartum infections, the majority of were a consequence of the invasive “manual removal” of the placenta.
.
Their definition of “obstetrics” was the polar opposite of the historical form of maternity care provided in Western Europe.
For the previous 2 centuries, European countries had a maternity care system in which professionally-trained midwives attended normal childbirth in essentially healthy women, backed up by general practice physicians., who in turn called in an obstetrician to treat complications that required obstetrical expertise.
However, in the United States the new “American obstetrics” insisted that childbirth was actually a very dangerous quasi-pathological condition that regularly required medical interventions and surgical procedures, and therefore, childbirth itself was the ‘property’ of the obstetrical profession as a new surgical specialty.
This included an organized and ultimately successful campaign to eliminate the practice of midwives. With the political and economic help of the AMA, obstetricians lobbied to pass state laws that made it a crime for a midwife to addend a birth.
of beginning in 1910 in conjunction with the annual meetings of the AASPIM which were arranged and financially backed by the American Medical Association. The bad news is that the
this post will be
Editor’s note-2-self: this post should be divided and made into a 3rd section
Part 2: The Dark Side of the Moon ~ the false promise of “Painless Childbirth”
During this period — 1910 to the late 1970s, an average of 2 million) gave birth in the United States — approximately 120 million women during that 60-year period of dysfunctional obstetrics. Due to the interventionist nature of our obstetrical system, many hundreds of thousands of childbearing women were harmed by the routine use of medically-unnecessary obstetrical interventions – general anesthesia, forceps, and particularly the manual removal of the placenta.
Having the doctor reach his gloved hand up through the mother’s vagina and into her uterus in order to peel the placenta of the uterine way is doubly dangerous. The first danger is triggering a torrential postpartum hemorrhage and the second is having introduced bacteria from the mother’s vagina that do not cause disease when restricted to the lower part of the birth canal but become are pathological when carried up into the material cavity of the mother’s uterus. The resulting fatal infection was responsible for a very high rate of maternal deaths before antibiotic drugs became available.
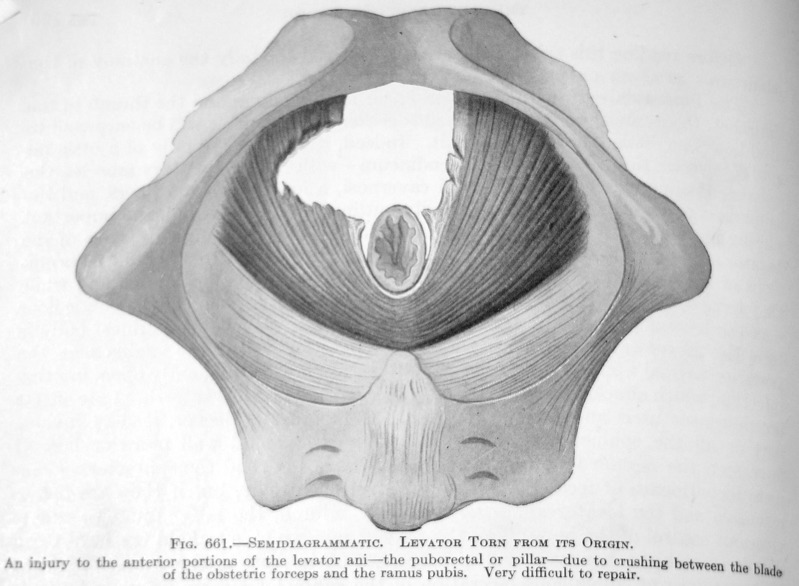
Illustration from an obstetrical textbook showing damage to the pelvic flow muscle when the blade of a forceps cut the muscle, leaving a big hole
The routine use of forceps routinely damaged the nerves and muscles of the childbearing woman’s pelvic floor. This often resulted in lifelong incontinence of urine and/or stool, making these women into social pariahs, unable to leave their homes lest they have an “accident” in polite society. This was happening a hundred years before convenient disposable incontinence products such as “Depends” were available.
As many as 10,000 thousand died every year from the fatal infection septicemia (often described as “blood poisoning”) in the decades before the discovery of antibiotics. Another ten to fifteen thousand newly delivered mothers died from other causes, many of them preventable deaths due to the aggressive use of invasive obstetrical procedures that went amok.
We know this to be the case because the MMR in Western European countries was often as much two or three times better than in the US.
For example, at the same time, the MMR in the US was 700 per 100,00, it was only 232 per 100 in Sweden. At that time neither country had either sulfa drugs or antibiotics. What was different was that normal births in Sweden were attended by professionally-trained midwives who did not use any kind of anesthesia, obstetrical intervention, or invasive procedures. However, childbirth in the US was night-and-day different, as general anesthesia, obstetrical interventions and invasive surgical procedures were “business as usual”.
The Brilliant Execution of a really Terrible Idea!
Dr. J. W. Williams’ search for non-governmental funding for a badly needed nationwide system of general hospitals was a virtuous goal that would save lives and reduce suffering. In 1914, the vast majority of the population of the United States lived on farms and small towns, more than a hundred miles from a general hospital. The entire population of these regions — men, women, and children — who became critically ill or injured would suffer greatly and in many instances, either die or be permanently disabiled.
While the United States had 8,000 or small (2-to-10 bed) hospitals but only a couple dozen large hospitals capable of providing comprehensive medical and surgical services. Compared Western Europe, America was a third world country in regard to state-of-the-art hospital care. During the early 20th century, the US Congress had not addressed the issue of access to comprehensive hospital services. No doubt lobbying efforts by the AMA to protect the private ownership of hospitals and clinics by medical doctors as a profitable business venture. That trapped the United States in a very dangerous status quo.
Dr. J. Whitridge Williams stepped into that void. Opposisition by the AMA took federal financing off the table. The profit margin for many small hospitals was to small qualify for a bank loan. With no other obvious options, Dr. JWW concluded that selectively hospitalizing healthy middle and upper class white maternity patients would generate a large, dependend profitable revenue stream in perpetuity for any and all hospitals that already had or put in a “lying-in” ward and began to diligently seek the patronage of the this healthy and relatively well-off demographic of middle and upper class white pregnant women.
Every hospital a would be able to use this revenue to self-fund the modernization and upgrading of their facility that depended on. and given the nature of the female reproductive system in an era in which 75 % of all adult women were married and before effective contraceptive products were available and/or legal. that would be self-p
The purpose of turning Maternity patients into a gaggle of geese, who laid golden eggs on a daily basis. Considering that CB women were in the prime of life, had an average of had six children so were a dependable source of,
repeat business was astounding, especially when you take into consideration that these are all healthy women who really do not need much in the way of medical or nursing care. They just need a back up you know a bed clean linens three meals a day Little bit of help with getting the mother to the bathroom or figuring out how to take care of breast-feed, a cranky baby to lay the golden egg, so to speak, was to fund the modernization of small and medium size, privately owned hospitals, which basically were the only kind that that existed in any numerically important number. The best estimate being 8000 or so hospitals of which 95% of them were were small 2 to 10 bed private, Dr. Owned and run hospitals.
The goal of Dr. William’s goal was the modernization of small and medium size hospitals, until some substantial proportion of those became big enough to become GENERAL HOSP‘s. So that was that’s what they were trying to achieve and to do the funding so that it did not include any kind of federal funds. If you continue to note that these are privately owned for-profit hospitals and the AMA and the medical profession in general, did not want the federal government messing in their entrepreneurial adventures
plan was the modernization the goal of doctors
However, Part Two of his plan for raising those funds was unethical, harmful in many ways and at many levels, and resulted in a large number of preventable deaths of new mothers and babies.
The most critical element of Dr. JWW’s plan — the elective hospitalization of well-off white women as paying customers. Without any “informed consent, these women were forced to labor under the influence of Twilight Sleep drugs, and as perfectly healthy women, were nonetheless given general anesthesia and subjected to a series of invasive surgical procedures that included the use of obstetrical forceps for what otherwise would have been, should have been simply a normal (i.e. spontaneous) birth.
At the heart of this brilliantly executed but very terrible plan was a very big and very black lie by Dr. JWW. His financial “scheme” (his word, not mine!) to promote and fund a nationwide system of privately-owned general hospitals was based on a specifically targeted demographic of maternity patients as paying customers — i.e. healthy, wealthy, and white childbearing women in the prime of life whose families could easily afford a hospital birth and the traditional 14-day “lying-in” stay in the hospital maternity ward.
To seduce this well-off to have a hospital birth, Dr. Williams simply lied by inventing a story about a non-existent danger that only affected this demographic of well-off white women. The goal was to trick members of this particular demographic into thinking they suffered from a rare “evolutionary fluke” that made the normal biology of labor and birth particularly dangerous for them. Dr. JWW described this pathology as a biological “error” or “genetic fluke” that only affected this particular demographic by putting these particular women, and only them. It put them at high risk for having an abnormal reaction to the “normal” pain of active labor. For some women, this reaction could trigger a mental breakdown so severe that it would require the family would have to commit the new mother to a mental institution for weeks or months.
If you are looking for a way to scare a particular demographic of women into giving birth in the hospital, this certainly was an effective way to do it!
The Many Lives of “nervous breakdowns” and Other convenient lies
The whole story that Dr. Williams told about the normal pain of labor being pathological in upper-class women was actually non-existent, what today we might describe as a “jive and a humbug“. But the mere idea of it functioned very well for Dr. Williams. He simply admitted that this labor-related nervous break was rare, but since there was no way for him or other obstetricians to know which women would be affected; to be “on the safe side”, all white well-off women would have to be “prophylactically” hospitalized as soon as they went into labor.
From an economic standpoint, maternity patients became the goose that laid golden eggs — healthy paying customers who (a) were not sick and (b) providing care to this healthy population was very inexpensive and (c) represented frequent repeated business!
ensuring a steady stream of electively hospitalized healthy childbearing women who would over the course of their life have an average of six children. characteristics of who were healthy And just like that, hospitals in America created a became
The birth rate in the US during the first half of the 20th century was two million annually.
The programmed destruction of normal childbirth as a developmental stage of a pregnant woman’s life and her transitions into motherhood
social isolation from her family, depersonalization as a laboring woman, and the extreme level of fear as the still unmedicated new patient is being edited to a busy ward with 5 or 10 other labor patients under the influence of the Twilight Sleep drug scopolamine who are moaning, yelling out, swearing, or screaming at the top of their lungs with every contraction. Scopolamine provides NO relief; it only effect is to induce a temporary state of psychosis and a permanent state of amnesia
What Dr. Williams didn’t reveal was the magnitude of this supposed “simple” intervention from the perspective of
Under these circumstances, these laboring women would be heavily medicated with Twilight Sleep drugs, and the birth conducted under general anesthesia in an operating room by an obstetrically-trained surgeon as a surgical procedure. “Delivery” included a series of surgical interventions — episiotomy, extraction of the baby with obstetrics forceps, and manual removal of the placenta.
This last intervention — inserting a gloved hand into the new mother’s vagina and up into her uterus to peel the placenta off the uterine wall — was the very most dangerous intervention during this pre-antibiotic period of history. Before sulfa drugs and penicillin became available (1937 and 1945 respectively) 40% of all maternal deaths (15,000 to 25,000 annually) were the result of fatal infections known as septicemia or “blood poisoning”.
Reaching into an organ in the new mother’s body contaminated the doctor’s glove with the “normal” bacteria of the mother’s vagina. As he reaches into the uterus and tries to pry the placenta off the uterine wall, these bacteria find their way into the mother’s bloodstream. In a high percentage of cases, the body had no immunity to these new and blood-borne pathogens. Far too often, the result is a potentially-fatal infection of a type called “iatrogenic” — that is, an infection that traces back to something the doctor did that resulted in a complication that otherwise would not have occurred.
Propaganda Campaigns identifying “modern women” with “hospital birth”
In the first decades of the 20th century organized medicine (i.e. the AMA) launched a well-financed and decades-long propaganda campaign promoting the idea that what it meant to be a “modern woman” was to have your baby in the hospital.
This aspect of Dr. Williams’ two-part “plan” not only influenced many middle- and upper-class families to have planned hospital births but its “talking points” launched a decades-long propaganda campaign. Articles published in newspapers, women’s magazines, and radio programs promoted hospital births while simultaneously denigrating the care of midwives. This PR campaign circulated articles in women’s magazines claiming that what it meant to be a “modern woman” was to have their babies in the hospital.
EDIT LINE >> Dr. Williams Aug 03, 2023
That story continued as the obstetrical profession turned healthy childbearing women into the patients of a surgical specialty and normal childbirth into a surgical “procedure” performed by doctors on healthy women rendered unconscious by general anesthesia
And the desire to see economically successful white m&uclass women be the nature choice for propagating the European race in the US — opposite of ‘anchor babies of immigrants and high birth rate among women of color
@@@End of “Mission Impossible” @@@
@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@
**Forensics examination of information refers to published documents as a body of evidence that can be traced back to the originating individuals, similar to the legal process known as a “chain of custody”
The purpose is to assemble a body of information based on documentary evidence that truthfully describes the issues presented, discussed and the conclusions subsequently drawn from this evidentiary body of information that is capable of documenting such finding in a court of law.
________________________________________________________________________________
Dr. J. Whitridge Williams was the Dean of John Hopkins School of Medicine when he co-authored Twilight Sleep: Simple Discoveries in Painless Childbirth with a well-known and respected science-writer, Dr. Henry Smith Williams (no apparent relation).
Compelling circumstances in Dr. Williams’ life molded him into an unexpected, even accidental visionary. He saw a ‘big picture’ that was invisible to the previous generation of doctors and to his contemporaries. Having identified a huge problem with hospitals in the US, he boldly took action by calling for the creation of a nationwide system of general (acute-care) hospitals. At that time, the US had approximately 8,000 hospitals, but only a couple dozen of them were well-equipped general hospitals and all of those were in big metropolitan areas.
To accomplish this, he introduced a new economic model for privately-owned hospitals, and a practical but lengthy and multi-stage ‘business plan’. This consisted of creating a system of lying in hospitals or lying-in wards in existing hospital so there would be at least on small lying in hospital in every population center over 3,000 that he described “…as ubiquitous if not as numerous as schoolhouses and libraries”. @@ need citation
Simultaneously with these new facilities, his plan called for electively hospitalizing healthy middle and upper-class maternity patients as paying customers and the dependable profits that generated would provide a steady source of revenue to finance a new nationwide system of privately-owned general hospitals over the next two or three decades.
Dr. JWW’s book “Twilight Sleep: Simple Discoveries in Painless Childbirth” was in essence the blueprint for his economic plan and associated public relations campaign aimed at influential men of means (especially wealthy philanthropists), state and local officials, and husbands who decided how the family money would be spent.
Dr J. Whitridge Williams is the most famous obstetrician of the 20th century and also author of the classic obstetrical textbook Williams Obstetrics. He was at the very top of a truly remarkable career when he partnered with science writer Dr. Henry Smith Williams in 1913 to write his book: Twilight Sleep: Simple Discoveries in Painless Childbirth.
His book was not intended for women, nor was it meant to be read by women; instead it was designed to inform and persuade wealthy philanthropists, influential or wealthy men, husbands and other men who might become be willing to assist Dr. J.W. Williams in promoting his ideas and achieving certain goals.
But the backstory of how this book came about, how its major themes were developed, trace back to a profound sense of angst by Dr. J. W. Williams – that he had intimate knowledge of a wrong that badly needed to be righted. The vast majority of American hospitals were tiny 2-to-10 bed for-profit facilities in small towns privately owned and operated by the local doctor. They only accepted patients who could paid up front and only provided ‘supportive’ care and minor surgeries. That meant that most Americans were a hundred miles or more from an acute-care hospital capable of providing emergency care to people who’d been seriously hurt or became acutely ill.
In spite of his many professional achievements, this monumental problem kept gnawing at him to “do somethings”, take some kind of definitive action. But how could he effectively address this vast nationwide issue?
His answer was to write a book that defined the ‘problem’ and acknowledged its magnitude. Then he laid out a plan that provided a new economic model, a theoretical blueprint with strategies and tactics for bringing this about, and a business plan for how small and medium-sized community hospitals all across the US could easily and forever change the economic foundation and function of acute-care hospitals in the United States.
As a patriotic American and the single most influential physician-leader of his generation, his private dream and public passion was a nation-wide system of general hospitals to rival the nationalized system used in Western Europe for more than two centuries. Western European countries began systematically developing a program of government-sponsored general hospitals in the 17th century, with a dozen or more institutions in the different regions based on population of the country. All the hospital services were available to the public, irrespective of ability to pay.
An additional advantage of a nationwide system of general hospitals is the many opportunities it can provide to advance medical education and surgical techniques as a result of clinical training programs for medical students in these busy and well-equipped hospitals.
Medical and nursing staff of London hospital, circa 1912
By the early 20th century, these general hospitals were typically staffed by well-trained professionals, had the up-to-date medical equipment and were able to provide comprehensive services to all ages and for all types of medical and surgical problems.
Typical one-room, 8-bed private, doctor-owned and run hospital of the late 19th and early 20th century
By comparison, the US in the late 19th and early 20th century had plenty of hospitals — 8,000 by one count — but they were very small, private 2-to-10 bed hospitals owned and operated by one or more local doctors. These overnight clinics and one-room hospitals were only able to provide ‘supportive’ care and perform minor surgeries. They often restricted their services to patients that were all suffering from the same medical condition such as TB. But they couldn’t afford to state-of-the-art medical equipment such as x-ray machines, microscopes, autoclaves and those large iconic operating room spotlights, nor did they have an emergency room available to the public. As a for-profit business, their policy was not to provide care to anyone who couldn’t pay out of pocket at the time of service.
@@@@@@
Beginnings
Dr J. Whitridge Williams was from a wealthy New England family of lawyers and doctors that four generations ago had emigrated from London to the American Colonies. He had an excellent formal education and graduated from medical school with distinction. Then he went to Europe to get clinical training in obstetrics and pathology and spent two years studying in some of the most famous hospitals.
After returning to the US, he decided to specialize in gynecological surgery and finished his training in 1893. Shortly afterwards he was hired by the new and very prestigious Johns Hopkins University Hospital in Baltimore, Maryland to set up their gynecological surgery department. His meteoric climb to the very pinacol of medical prominence began in earnest in the early 1900s when he was appointed chief of obstetrics for Johns Hopkins; his landmark obstetrical textbook was published in 1904, and in 1911 he was appointed Dean of its School of Medicine. This made him the most socially, politically and economically-influential obstetrician in America.
However, he was still profoundly disappointed in the American healthcare system and particularly disturbed over our lack of a comprehensive or ‘general’ hospital system when compared to western Europe. Most European countries had long ago developed a nation-wide system of general hospitals that provided state-of-the-art care to the public at large. Many of the biggest general hospitals in Europe were charity institutions started in the 16th and 17th century (or earlier) by the Catholic Church and staffed by monks or nuns. The most famous is the Hotel-Dieu in Paris on the river Seine, founded in 600 CE and still going strong today.
The distinguishing feature of a ‘general’ hospital is its ability to provide acute care to everyone in its geographical area regardless of age, gender or type of health problem. Whether it’s a medical or surgical problem, a pediatric or geriatric patient, or anyone in between, the well-equipped and trained staff of a general hospital can provide effective care to any kind of patient. This includes setting a broken bone or stitching up a cut, as well as appendectomies, treating serious accidents, heart attacks, pneumonia, complicated childbirth or caring for a premature baby.
These big public hospitals also played a critical role in advancing the process of medical education. Beginning in the 1500s, regional general hospitals began partnering with medical schools to develope clinical training programs that provided valuable hands-on education to thousands of medical students across Europe each year. At the same time students were educationally benefiting from their clinical training program, its cadre of interns and residents were also providing free medical care to poor and homeless hospital patients in exchange for their willingness to become ‘teaching cases’. This was an amazingly positive situation for all the parties – hospitals, medical schools, med students, indigent hospital patients and medical science.
How different on the other side of the “Pond”
Unfortunately for Dr. JWW (as well as the entire population of the United States) America had no system of general hospitals, or anything vaguely close to it. One reason for this were laws against the presence of Roman Catholic churches, priests and even individuals. It was illegal for a professed Roman Catholic individual to own property in many states, so the “Church” didn’t found charity hospitals in the US as they’d traditionally done in Europe. However, there were other charity organizations, universities and state and local government that funded the building and running of general hospitals. However, there were only a couple dozen of these in the entire country.
The lack of big general hospital also meant no clinical training for the vast majority of the thousands of medical students that graduated each year. Even though their medical school education did not include clinical experience, every newly minted MDs in the US was legally authorized to perform life-threatening medical procedures and surgical operations that they’d never practiced, never performed before, or in many cases, never even seen done, including complicated forceps deliveries. This is why Dr. JWW, as a new graduate MD, had to “go abroad” to receive his clinical training.
Instead of big regional hospital like Europe, the US had, by one estimate, an astonishing 8,000 ‘for-profit’ private hospitals owned and run by the town’s doctor. The majority these were tiny one-room hospitals with 2-to-10 beds, and except for a telephone, they had little or no “modern” medical equipment. They offered no emergency services and generally only admitted people who could pay up-front.
Dr JWW was also acutely aware that travel time to a general hospital for a majority of Americans was not measured in hours but in days. Americans were suffering unnecessary, preventable and painful deaths from accidents and treatable illness because they lived so far from a general hospital that they were unable to get timely and life-saving medical care. What stood between astonishing scientific discoveries and the patients desperately in need of a medical miracle were miles and miles of roads and dark of night.
Having seen Paris (as the saying goes), it was clear to Dr JWW that not having a nationwide system of general hospitals was something the United States should hide its collective head and something he needed to fix. He envisioned a coast-to-coast network of small-to-medium full-service general hospitals in every community over 3000 people. He described his vision of these hospitals being “as ubiquitous, if not as numerous, as libraries and schoolhouses”. The expectation for these fully-equipped and staffed general hospitals was for them to provide the same 20th-century state-of-the-art medical services (in quality if not quantity) as his own alma mater, Johns Hopkins.
As a well-endowed general hospital, Johns Hopkins University Hospital was able to provide the same high level of comprehensive medical and surgical services as was available in Western Europe. But there were so very few general hospitals in the US and all of those were in big metropolitan areas such as New York, Chicago, New Orleans, Denver and the biggest cities on the West Coast. They couldn’t begin to meet the daily medical needs of a population of a large county like our that reached “from sea to shining sea” and everywhere in between, including rural farming communities, remote mountain regions and unmeasurable miles of “back country” with barely passible roads.
In a thought-provoking way, Dr. JWW was promoting the essence of democratic equality, demonstrated as equal access to life-saving medical care regardless of where you live – crowed city or wide-open country, high up a mountain or rural fishing village. If we accept this premise (which we did), can “equal access to life-saving medical care” regardless of ability to pay be far behind?
Acknowledging universal access to all the treatment modalities commonly available in the 20th century general hospital is actually the most a profound “socializing” of medicine one can imagine, and something I wish to bring to the attention of the AMA.
Dr. J. Whitridge Williams’ Vision Expressed as an Economic Model and Business Plan
In his own strange way, Dr. JWW’s was as much of a pioneer as Danial Boone or Davey Crocket, except that Dr. JWW’s goal was not conquering wilderness but developing a nationwide system of general hospitals. That was going to require a lot money over a very long time; he assumed it would take at least 20 or 30 years, even longer, to match to the European model he espoused.
The only thing he knew for absolute sure was that the kind of funding that financed the general hospital system in Europe – generous quantities of government money — was not an option in the US because organized medicine would never allow it. Since being incorporated in 1847, the American Medical Association has fought against the slightest whiff of anything they thought of as “socialized medicine”.
The reason for this was simple: Physician-politicians saw the private practice of medicine in the US as an unlimited entrepreneurial opportunity – the right to be in business for yourself and not have to share the profits. Every private doctor’s office was its own independent business, and there were nearly 8,000 doctor-owned hospitals in the US – the “sky’s the limit” capitalism at its very best! Nobody could tell doctors what to do because they were their own boss, in charge of how they practiced medicine, never a “mere” employee of an institution or government agency that would have the legal right to interfere in the so-called “sacred doctor-patient” relationship.
From the AMA’s point of view, government funding for medical care of any kind was permanently off the table, whether it was paying hospital construction costs, administrative costs, or (God forbid!) the salaries of physician-employees who worked for these institutions. If the AMA prevailed, not a single penny of public money would ever be used to finance hospitals.
This put Dr. JWW back where he started and meant that he had to keep thinking “outside the box”. This was not all bad, as he saw his role as the propagating of (something outrageous) ideas, responsible for turning the best of them into an action plan and then to figuring out how finance his grand scheme. Since robbing a bank was not an option, he had to figure out how to make this intergenerational project become self-funding and thus pay for itself.
Dr. J. Whitridge Williams — A Committee of One
Knowing he was totally on his own, Dr JWW would have to be “inventive” and “think outside the box” – way outside the box – to find or create a way to finance this new system of general hospitals to rival those of Europe and depending on your perspective, he didn’t disappoint!
Dr. JWW’s “plan”, as he referred to it, was purely economic. It began with a brilliant but ethically dubious idea – a self-funding “work-around” that would make use the system in creative ways the ultimately made it pay for itself. His scheme (his word, not mine) began with a two-part idea married together like the two sides of a coin.
First he invented a brand-new category of ‘hospital patient’ based purely on economics — the electively hospitalized healthy patient who was (a) not sick (b) and could clearly afford to pay for whatever hospital services he or she wanted or received.
Dr. JWW identified the first candidate for this new category of ‘elective hospitalization’ as healthy middle- and upper-class maternity patients. Unlike typical hospital patients who were gravely ill or injured, these healthy maternity patients would be paying customers from families that, in addition to paying their private doctor, could also afford to pay a significant hospital bill for the standard 14-day “lying-in” period for mother and baby (a total of 28 ‘patient days’).
Electively hospitalized maternity patient as paying customers was the first side of the coin. Step two of his plan was to urge small private medical facilities to immediately turn themselves into “lying-in” hospitals, while encouraging larger hospitals to turn any empty room or unused space into a new and profitable maternity ward.
This part of Dr. JWW’s financial “scheme” worked because young healthy childbearing women aren’t really “patients”, in the since of being sick or disabled or otherwise expensive to care for. Compared to the usual critically ill or injured hospital patient that required extensive nursing care and other hospital service, maternity care was very profitable for hospitals.
Caring for new mothers and their babies was more like running a mother-baby hotel than an acute-care hospital. What these healthy new mothers mostly needed was a dry bed, clean linens, a fresh pitcher of water on their bedside table and 3 nutritious meals a day. What new mothers did most of the day was to lay around while breastfeeding their babies (the origin of the concept a “lying-in” ward) while chatting with the other new mothers in their ward, changing diapers or bathing their new baby and dressed him or her in clean clothes.
Just as Dr. JWW had anticipated, revenue generated by lying-in wards had an unusually high profit margin. One modern publication noted that on average hospital maternity wards make 38 cents profit was every dollar, which the profit margin for cardiac care units only is only cents on the dollar.
Part two of Dr. JWW’s plan, which was to use the profitable revenue stream from small lying-in hospitals and lying-in wards in larger hospitals to modernize their facilities, upgrade medical equipment and purchase new capital-intensive such as a new x-ray machine, autoclaves (industrial-sized sterilizers), microscopes for their new clinical lab and new operating rooms with ceramic-tiled walls easy and quick to disinfect between operations and big electric lights to illuminate the surgeon’s operating field.
In person and via publication of his book, Dr JWW made appeals to wealthy philanthropists to help finance the first stage of his self-generating plan — the lying-in wards soon to become the “cash cows” of the hospital business. Dr JWW also appealed to “the husbands of America”. He said if husbands were able to convince just half of the two millions American women that gave birth every year to have a hospital birth, the profits that generated would provide a steady revenue stream that would allow those tiny 2-10 bed hospitals to gradually upgrade their medical equipment and remodel their facility until they finally turned into a fully-equipped and well-staffed general hospital.
This process would slowly create general hospitals all across America, equipped and staffed to provide out-patient emergency services and in-patient medical and surgical care to everyone living in near-by communities. These is no doubt that providing timely access to a well-equipped general hospital to millions of Americans over the course of the 20th century dramatically reduced suffering, prevented permanent disabilities and saved lives. From that perspective, whatever trade-offs were involved seemed well worth it.
However, childbirth as experienced by those healthy maternity patients who got targeted for “elective hospitalization” as a part of Dr. JWW’s revenue generating plan was a very different story, one that had nothing to do with making childbirth safer or better and everything to do with making hospital-based childbirth services into the hospital’s “cash cow” or ATM machine with no limits.
In addition to upgrading its facilities into general hospital status, this dependably profitable revenue stream from its maternity wards turned the failing economic model of hospitals upside down and re-wrote the book, newly titled “How to get rich quick in the hospital business”. Traditionally hospitals were virtually all charities, since the terms “sick people” and “paying customers” are a natural antithesis. Unless a hospital is part of a publicly finances national healthcare system, they are always drowning in red ink because critically sick and injured patients run up big hospital bills, then die or otherwise can’t pay for the cost of their care. But profits from these new “lying-in” wards more than made up for the hospital’s losses on uncollectable debits.
The Less Patriotic Aspects of Dr. JWW’s “Scheme”
Dr. Williams’s “plan” did not simply focus on build up a network of general hospitals. He also spent a lot of time and energy trying to convince public officials and wealthy philanthropist (also all male) that midwives and home birth were unspeakably “old-fashioned” and the medical profession had an ethical obligation to drive midwives out of business, to be replaced by with hospital maternity departments that were staffed by nurses.
@@@@@@@@@@@@@@@@@@ stopped here at 6:15 pm Nov 22 @@@@@@@@@@@@@@@@@@@@@
It is a story about the decades-long propaganda campaign that denigrated the care of midwives general practice doctors while circulating articles in women’s magazines claiming that the “modern women’ had their baby in a hospital.
That story continued as the obstetrical profession turned healthy childbearing women into the patients of a surgical specialty and normal childbirth into a surgical “procedure” performed by doctors on healthy women rendered unconscious by general anesthesia
1911 ~ Dr. Emmons, MD: “Obstetrics Care in the Congested Districts of our Large American Cities”
“For the sake of the lay members who may not be familiar with modern obstetric procedures, it may be informing to say that care furnished during childbirth is now considered, in intelligent communities, a surgical procedure.” [1911-D, TAASPIM, p. 214]
It’s a story in which middle and upper class husbands were misinformed about the nature of labor pains in healthy, educated, intellectual and delicate’ (white) women from the middle and upper classes, being wrongly informed that these women suffered from an evolutionary fluke caused by civilization that made the ‘normal’ pain of labor abnormal – so excruciating and intolerable pain, making these women high risk for a mental breakdown that might one wife to be being permanently institutionalized.
It’s a story in which obstetricians tell husbands this can all be avoided by simply hospitalizing their wives, where they will labor under the influence of Twilight Sleep drugs and give birth after being rendered unconscious under general anesthesia.
It’s also the story of millions of women between 1910 and the 1970s being forced to labor under the influence of narcotics and the Twilight Sleep amnesic and hallucinogenic drug scopolamine,
It’s a story about the uncritical acceptances of unscientific idea that childbirth was fundamental pathological and the science saved women certain damage or death by routinely using unnecessary and invasive obstetrical and surgical interventions in normal childbirth; these included the routine use of general anesthesia, episiotomy, the use of forceps and manual removal of the placenta by a doctor who reach his hand and lower arm up into the newly delivered mother’s uterus to pull out the placenta.
This is a story in about babies that never breathed due to the depressive effect of drugs given to their mothers during labor, or who died from unnecessary obstetrical intervention.
It’s story about hundreds of thousands of pregnant women of whom childbirth didn’t have a happy ending.
Dr. Williams’ book was a blueprint for convincing husbands that their educated and upper-crust (i.e. white) wives risked permanent mental breakdown from the pains of normal labor unless they were hospitalized and given Twilight sleep drugs and had a forceps-assisted birth under general anesthesia.
“…. the cultured woman of to-day has a nervous system that makes her far more susceptible to pain and to resultant shock than was her more lethargical ancestors of remote generations.
… women of primitive and barbaric tribes appear to suffer comparatively little in labor, coupled with the fact that it is civilized women of the most highly developed nervous or intellectual type who suffer most.
Such a woman not unnaturally shrinks from the dangers and pains incident to child-bearing; yet such cultured women are precisely the individuals who should propagate the species and thus promote the interests of the race.
This seems to suggest that the excessive pains of childbirth are not a strictly a ‘natural’ concomitant of motherhood, but rather that they are an extraneous and in a sense an abnormal product of civilization.
Is there not fair warrant for the assumption that the pains which civilized women—and in particular the most delicately organized women –suffer in childbirth may be classed in this category?
Abnormal pain as an evolutionary threat to the (white, European) race ~
Considered from an evolutionary standpoint, the pains of labor appear not only uncalled for, but positively menacing to the race.
…… any trait or habit may be directly detrimental to the individual and to the race and they may be preserved, generation after generation, through the fostering influence of the hot-house conditions of civilized existence.
Evolutionary pain in white women as a Darwinian
segue to a perverse form of eugenics
Everyone knows that the law of natural selection through survival of the fittest, which as Darwin taught us … does not fully apply to human beings living under the artificial conditions of civilization. These artificial conditions often determine that the less fit, rather than the most fit, individuals shall have progeny and that undesirable rather than the desirable qualities shall be perpetuated.”
The problem of making child-bearing a less hazardous ordeal and a far less painful one for these nervous and sensitive women is a problem that concerns not merely the women themselves, but the coming generations.
Let the robust, phlegmatic, nerveless woman continue to have her children without seeking the solace of narcotics or the special attendance of expert obstetricians, if she prefers. But let her not stand in the way of securing such solace and safety for her more sensitive sisters.
… every patient who goes to the hospital may have full assurance that she will pass through what would otherwise be a dreaded ordeal in a state of blissful unconsciousness.
