Reading time ~ 10 minutes

==============================
The last and most important UNTOLD story of the 20th century!
The perfect storm that turned healthy women into the patients of a surgical specialty and normal childbirth into a surgical procedure
This was the most profound change in childbirth practices in the history of the human species.
==============================
Part 2
Like those lacquered Russians dolls that nestle one inside of another, each smaller than the previous one, there is a small but vital piece of information found at the center of the many-layered history of American obstetrics in the 20th century.
The ‘what’ and the ‘how’ are important and informative, but the real heart of the matter is ‘why’. The answer to that question turned out to be much broader and deeper than I ever could have imagined.
The story starts in 1910, which was the end of the pre-scientific medicine and the beginning of what we now talk about as “medical science”. Everything about the practice of medicine was changing, including obstetrics. Up to that point in history, “catching babies” was just a minor part of the general practice of medicine. That all changed as the new hospital-based surgical speciality displaced virtually everything that went before.
Before medicine became a science, all birth-related care was described as a “midwifery”, whether birth attendants was an MD or midwife. The word historical term “midwifery” referred a set of medical (i.e non-surgical) skills that were taught to all students in medical school — “catching” babies and dealing with common problems such as a breech baby, a twin birth or a retained placenta.
 General practice physicians (GPs) who attended births described themselves as “man-midwives”. However, GPs were not trained in surgical procedures, so if a laboring woman needed a forceps delivery, a Cesarean or manual removal of the placenta, both midwives and GPs had to call a gynecological surgeon take over the case.
General practice physicians (GPs) who attended births described themselves as “man-midwives”. However, GPs were not trained in surgical procedures, so if a laboring woman needed a forceps delivery, a Cesarean or manual removal of the placenta, both midwives and GPs had to call a gynecological surgeon take over the case.
However, this sometimes caused hard feelings between GPs and gynecological surgeons, who were often dismissive or critical of the GP’s handling of the case, complaining that they really were needed or that they should have been called sooner and therefore any bad outcome was to be blamed on the GP.
The much lauded the new “American Obstetrics”
as a new hospital-based surgical speciality
~ 1910 ~

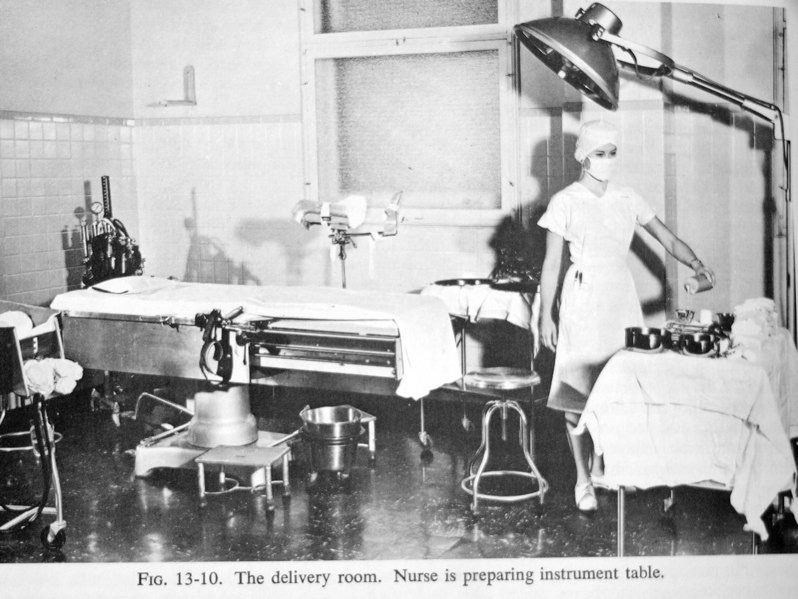
Conduct of “delivery” as a surgical procedure organized around the preservation of sterility, which required that doctors and nurse be masked and gowned and non-hospital personnel were allowed to be in the OR-style delivery room.
During the last decade of the 19th and first of the 20th century (1890 to 1910), a small number of very influential American doctors who “specialized” in complicated childbirth cases began to call themselves “obstetricians”, and started talking about the new “American obstetrics” as a hospital-based surgical speciality.
This fit perfectly with how these obstetricians described pregnancy and birth when talking to the American public. In newspaper articles, women’s magazines and radio interviews, these doctors defined pregnancy as a “nine-month disease” that required a “surgical cure“.
And as luck would have it, the newest crop of American obstetricians just happened to be very good childbirth surgery!
How this affected childbirth
in healthy women
An extraordinarily young labor patient under the influence of Twilight Sleep (morphine & the hallucinogenic drug scopolamine). To keep her from trying to get out of bed or falling out, the nurses put her into a straight-jacket that ties her arms across her chest and then ties the jacket to the sides of the bed.
Having defined obstetrical medicine to be a surgically-based form of care meant that all childbearing women — those in the bloom of good health as well as those with serious medical conditions and high-risk pregnancies — were thought of as surgical patients, referred to as surgical patients, and treated as surgical patients! That mean a hospital birth under protocols that insured absolute “surgical” sterility
So hospital L&D wards were all surgical units with the classic sign on the door that said “No Admittance – Authorized Personnel Only” in big black letters. The protocols required doctors, nurses and others to change out of their street clothes and work in hospital scrub suits, caps and masks.
As surgical patients, laboring women were immediately isolated from their families after arriving at the hospital. Husbands and mothers were usually told to go home, and wait for the nurse to call and tell them that his wife had given birth, if the baby was a girl or a boy, and tell the family when they could see their new boby and he could visit with his newly-delivered wife.
At the double swinging doors to the labor ward, new obstetrical patients were told to “Kiss your husband good-bye”. Then they were told to undress and put in a hospital gown, while the nurse put all their personal belonging — clothes, watches, earrings, wedding rings, eye glasses, hearing aids, an artificial limb — everything was put into a brown paper bag and sent home with her family. Then the mother-to-be had all her pubic hair shaved off, was given a large soapsuds enema, and then given a bath or shower to be sure the new mother was not harboring any germs.

When Twilight Sleep was first introduced in the US, the protocols included keeping the labor pt. in a darkened and quite room. But most hospitals didn’t have quiet rooms, so they put hoods or blindfolds over the mother’s head or put them in a big crib with a hood over the top.
the new labor patient was put in a hospital bed, the side-rails raised, and given the first of many injections of Twilight Sleep drugs. The use of these drugs was mandated obstetrical department protocols, she would given these drugs whether was wanted them or not!
From 1910 to the 1970s, laboring women spent the entirety of their labor lying in bed, which could be as long as two or even three days. Since they were not permitted to get out of bed or walk to the bathroom they also had to use a bedpan.
The effects and consequences of Twilight Sleep Drugs
given to laboring women
 The typical medicated labor patients get progressively groggy, them falls asleep and only wakes when they have a painful contraction. During the contraction they moaned, move around in the bed and displayed the typical signs of being in pain.
The typical medicated labor patients get progressively groggy, them falls asleep and only wakes when they have a painful contraction. During the contraction they moaned, move around in the bed and displayed the typical signs of being in pain.
It’s important to understand that scopolamine has NO effect on the pain. It doesn’t eliminate or even reduce the pain of labor, but it does erase the memory of it. These new mothers have absolutely no memory of anything that happened after they were given that first dose of Twilight Sleep drugs.
But lack of memory isn’t the only problem with the use of Twilight Sleep drugs. Under their influence, a small proportion of laboring women will have a “paradoxical reaction“. This reaction is the polar opposite of what a specific drug is supposed to do, like sleeping pill having the effect dexedrine.

An extraordinarily young labor patient under the influence of Twilight Sleep (morphine & the hallucinogenic drug scopolamine). To keep her from trying to get out of bed or falling out, the nurses put her into a straight-jacket that ties her arms across her chest and then ties the jacket to the sides of the bed.
About five percent (1 of 20) of labor patients given the Twilight Sleep drug scopolamine have a paradoxical reaction. They get very agitated, yell, swear, scream, stand up in their bed and try to climb over the rails, as well as hitting and biting the nurses. Unfortunately. As a result, it was necessary to physically restrain these patients.
The role of four-point restraints in the L&D
As a new new graduate working in L&D unit at the hospital where I trained (ie. low woman on the totem pole!) it often fell to me to put women having this paradoxical reaction into four point restraints. This required using the heavy leather wrist and ankle restraints also used on the psychiatric ward to pin the mother’s arms and legs to the four corners of her labor bed, thus forcing her to labor while laying flat on her back.
For a laboring woman, this is the most painful of all positions; to make her lay there like that for hours and hours while waiting for her to deliver was unmitigated cruelty. But that isn’t the end of this awful story. When laboring women lay flat on their backs, it dramatically interfere with blood circulation to the placenta, which means it’s the very worst position for keeping the fetus well oxygenated.
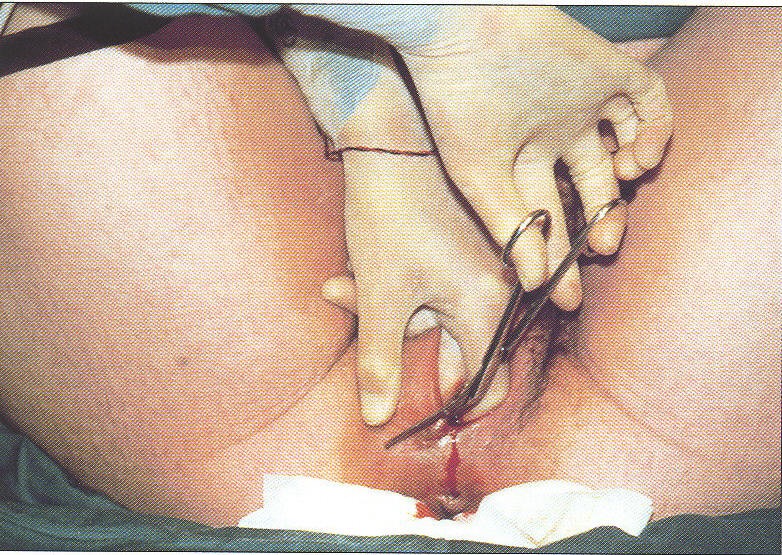
Obviously, the next chapter in this account of the the new American obstetrics as surgical speciality is to describe childbirth as something done to the woman by the doctors. Other posts on this topic are very detailed and describe exactly what is done and how. But for now, I’m only going to provide an overview.
When a laboring woman started to push and one of the nurses decide it was likely that she would give birth within the next 20-30 minutes, the patient’s obstetrician was notified to come. If she didn’t have a private doctor, OB resident was notified. Then the laboring woman was moved by stretcher to the PR-style delivelry toom,
by the depisiotomy, forceps, manually removing the placenta, suturing the perineal incision — was not merely “business as usual”, but the standard of care for normal childbirth in perfectly healthy pregnant.
This started out with the best of intentions, but unfortunately is quickly derailed by the classic “hubris” of the medical profession that assumes superior abilities and infallibly best described the MD version of “father know best” .
was accompanied by the standard cultural misogyny of the era that generally regard women in as an inferior class a deep prejudice against “female practitioners of midwifery” and fueled their on-going efforts to eliminate
This was followed by a series of seriously wrong assumptions about childbearing women and that nature of childbirth, and a(i.e. midwives), dominating that was normal for the early 20th century includes both heights of
What follows is a much abbreviated synopsis of the complex social and economic situation and the gender politics that weave the what, the how and the why into a compelling political saga that cries out for reform. The ideas may seem startling or even fanciful at first, but they all reflect information from thoroughly documented sources (references and bibliography available).
Cognitive Dissidence – Off to a bad start . . .
Against all logic and evidence to the contrary, physiological maternity care was replaced in 1910 by obstetrical interventions universally applied to a healthy population. This was, in large part, a reactionary effort by obstetricians in the earliest years of the 20th century to distance themselves as fast and far as possible from the shame and public humiliation of the infamous hand-washing scandal of the 1800s the iatrogenic practices of the previous century –. Even after Dr. Semmelweis’ discovery in 1847 that ‘childbed fever’ was a contagious disease carried on the unwashed hands of obstetrical professors and medical students, epidemics of maternal deaths continued to occur all over Europe in repeating waves. Obstetricians en masse ignored the indisputable proof and dismissed hand-washing as absurd, something they were too busy and too important to be bothered with.
By the early 1900s, the science of bacteriology had become an important part of mainstream medicine and obstetricians were embarrassed over the collective folly of the ‘bad old ways’. They jumped at the opportunity to replace a tarnished reputation with a brand new status as 20th century medical scientists who were experts in the high art of sterile technique.
But in their haste to protect themselves from the merest suspicion that their care might be the source of childbirth-related infections, they inadvertently replaced one specific and limited danger with a more global and far-reaching source of iatrogenic harm – the universal medicalization of normal childbirth and all that went with it. Most pernicious of all was redefining normal childbirth as ‘the delivery’, to be conducted as a sterile surgical procedure in a sterile operating room and performed by a physician-surgeon on an unconscious woman. Of course, fathers and other family members could not be present.
A textbook of that era described its ideal for the ‘new obstetrics’, which redefined both normal birth and the role of the obstetrician:
“If obstetrics is ever to attain the dignity of surgery, — and it should, — if the parturient woman is ever to enjoy the same benefits as the surgical patient, — and she deserves them – …. the make-shift policies of obstetric practice must be abolished. [ p. 290]
“The conduct of labor is not a simple matter, safely in trusted to everyone. Let the people know that having a child is an important affair, deserving of the deepest solicitation on the part of the friends, needs the watchful attention of a qualified practitioner and that the care of even a normal confinement is worthy the dignity of the greatest surgeon.” [p. 341, emphasis added]
But no matter how dignified or great the surgeon was, the problem for healthy mothers and babies in 1910 was that obstetricians took over the practice of normal childbirth (previously provided by midwives and family practice physicians) without knowledge of the philosophy, principles or techniques of physiological management.
Another part of the problem with the ‘new obstetrics’ is that it also did not take into account the psychological or the social needs of laboring women. What the loss of physiological and psycho-socially appropriate care meant to the well-being of mothers and babies was recorded in testimony presented in 1931 to the White House Conference on Child Health and Protection by the Committee on Prenatal and Maternal Care, who documented the efficacy of physiological care provided by midwives in the early decades of the 20th century:
“…that untrained midwives approach and trained midwives surpass the record of physicians in normal deliveries has been ascribed to several factors. Chief among these is the fact that the circumstances of modern practice induce many physicians to employ procedures which are calculated to hasten delivery, but which sometimes result in harm to mother and child. On her part, the midwife is not permitted to and does not employ such procedures. She waits patiently and lets nature take its course.”
Unfortunately, obstetricians had no appreciation for the greater safety afforded by strict adherence to physiological principles, were not content to wait patiently for ‘nature to take her course’ and had little respect for the dangers introduced by medical interference and surgical interventions. Obstetrics of that era was primarily about obstetricians trying to reinvent themselves, a task that also required them to deconstruct normal childbirth.
The Central Role of Medical Education in the ‘New Obstetrics’
Leaders in the obstetrical profession viewed the medical care of healthy childbearing women primarily as a source of teaching cases for the clinical training of medical students. Nearly all the early hospitals on the East Coast were associated with medical schools and this was the standard educational method. To provide medical students with adequate opportunities to develop the skills of interventive obstetrics, chloroform or ether, episiotomy, forceps and manual removal of the placenta and suturing of the perineal wound were routinely using at every normal birth.
This experience was an important part of preparing interns to manage the various obstetrical complications they might encounter later on as practicing physicians. Medical students and graduate physicians both needed to maintain their proficiency in the technical skill of forceps delivery, so this educational custom, which included birth as a surgical procedure, became the ipso facto standard of care.
A 1911 comment by Dr. J. Whitridge Williams’ on birth as a surgical procedure:
“For the sake of lay members who may not be familiar with modern obstetric procedures, it may be informing to say that care furnished during childbirth is now considered, in intelligent communities, a surgical procedure.” [emphasis added]
The Anatomy of Normal Childbearing & its relationship with Obstetrical Forceps
What most people don’t appreciate is how hard it is to use any mechanical force in the “J” shaped birth canal of a childbearing woman. Since babies don’t come straight out, like a train coming out of a tunnel, you can’t just pull them out with the medical equivalent of salad tongs or a toilet plunger. Learning how to artificially circumvent that 60-degree angle, the “parturient axis” officially called the “curve of Carus” (after anatomy professor Gustav Carus in 1789), is difficult.
The childbearing pelvis – that is, the internal bones that form the passage the baby must pass through — is a hollow space shaped like the lower-case letter “j”. People erroneously think of the birth canal as a straight chute (like a lower-case ‘l’), going straight down thru the lower half of the mother’s body. In other words, if the mother was lying down and you were watching from the side, people wrongly assume that her baby would pass through the pelvis and out of her body the same way a train comes out of a tunnel – a straight cylindrical object passing thru a straight cylindrical container. But this is not anatomically accurate for our human anatomy.
Black line traces the “J” of birth canal
Imagine instead that you are looking at an upright pregnant woman from the side as she labors and gives birth while still in an upright posture. If you had x-ray vision, you would see that the long stem of the ‘j’ tracks with the mother’s lower spine and the curved foot of the letter bends forward with the lower half of the birth canal. What this means is the pelvic outlet — last 1/3 of the journey – bends forward at a 60-degree angle.
This requires the baby to go around a ‘corner’ (an acute angle). If the mother is standing, her baby will emerge into the world going forward into her waiting hands. This is very different from going straight down towards the floor, where it would be hard for her to reach and might be injured as it fell to the ground. Not doubt “frontal delivery” is an important survival characteristic, as 99.99% of human history predates hospital obstetrics, which meant it was the mother herself who was responsible for ‘catching’ her baby.
Were you to look down into the pelvis from the top, you would notice that the big triangle-shaped bone at the very end of the spine — the sacrum and coccyx — encroaches into the pelvic outlet about half an inch. In this regard, the pelvis is like a hollow bowl with smooth walls on three sides but slightly bent in on the fourth side, making it impossible for anything that is the same size and shape as its upper circumference to pass through and out the bottom without seriously banging into this encroaching bony mass and perhaps being stopped by it.
However, in the second stage of labor, after the baby is squeezed out of the uterus thru the cervix and begins its trek down into the birth canal, you would see something remarkable. The place where sacrum affixes to the lower end of the spine is itself a joint – that is, motion is technically possible – and the effects of pregnancy hormones makes this and other pelvic joints slightly movable.
Figure #??
The triangular sacrum (at left), the public bone (at right) and the relationship of the baby’s head to both bones as it travels down thru the birth canal.
The baby’s head makes a 60 degree arc down thru the birth canal and rotates
under the pubic bone.
When the mother is upright, the baby is born going forward, into the hands of the mother or birth attendant.
=================================
As the baby’s head descends deeper into the birth canal, the sacrum and coccyx are pressed back out of the way, the same way a small pet door is bumped back out of the way when a dog or cat passes thru them.
In addition, the hormones of pregnancy have softened the cartilage that holds the two sides of the pubic bone together, so this pelvic joint also become unusually elastic, permitting the pelvic diameter to widen slightly side to side.
The everyday miracle of normal biology, in combination with the right use of gravity, gives the baby an extra couple of centimeters of room to negotiate its passage into the world. These ‘silly little centimeters’ are frequently the difference between a safe and spontaneous normal birth and one that requires the use of artificial, forcible or mechanical interventions (such as forceps) or Cesarean section.
Wrong Use of Gravity
“There is no alibi for not knowing what is known”
J. Rovinsky, MD — foreword of Davis Obstetrics (1966):
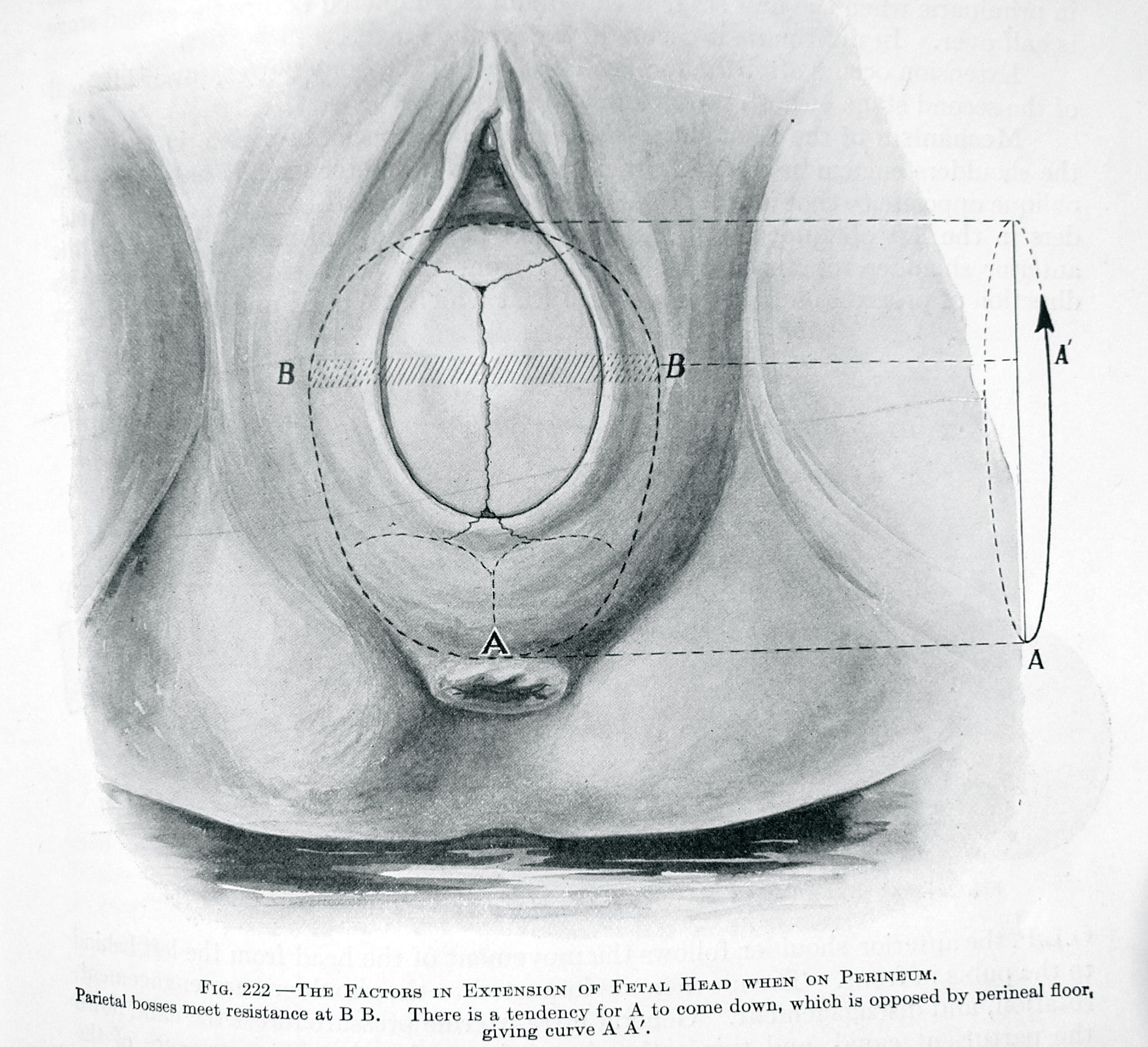
For a laboring mother, lying down is an anti-gravitational position that can reduce the pelvic size by almost a third, while simultaneously requiring the mother to push her baby up hill. Not only must her efforts defy gravity, but in this unnatural position, the passage is partially blocked. When the mother is bearing her own weight on her lower spine, such as lying on her back with her legs held up by the nurse or put in obstetrical stirrups, the aperture of her pelvis is reduced, as the sacrum cannot move back out of the baby’s way.
If the baby is small or the mother’s pelvis is big, the normal forces of labor and extra effort by the mother can overcome this impediment. However, when the mother is lying on her back, the baby must still head upward, towards the ceiling. Obviously this is a lot harder and takes a lot longer than it would if gravity were being used to the benefit of mother and baby.
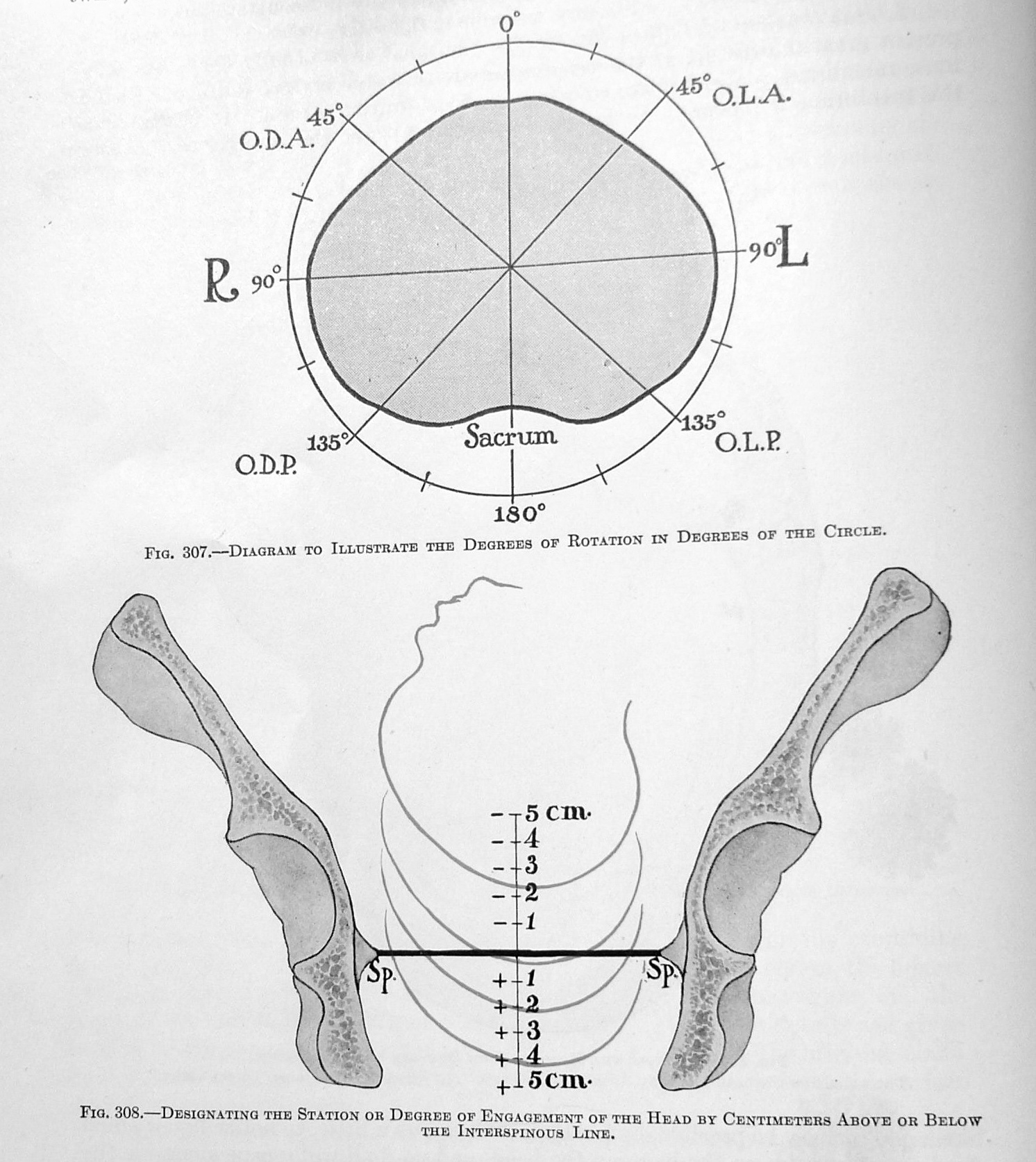
The Parturient Axis – giving birth without the added benefit of gravity, while mother lying on her back.
The baby must first negotiate its way under the pubic bone by rotating its head from sideways to an up / down orientation. (head position #1 & 2)
Then the crown of the baby’s head spins under the public arch (#2) will be born pointing up, towards the ceiling. (#3)
Head position #4 is after the baby’s head has already delivered upward, restitutes as the body rotates to deliver the shoulders
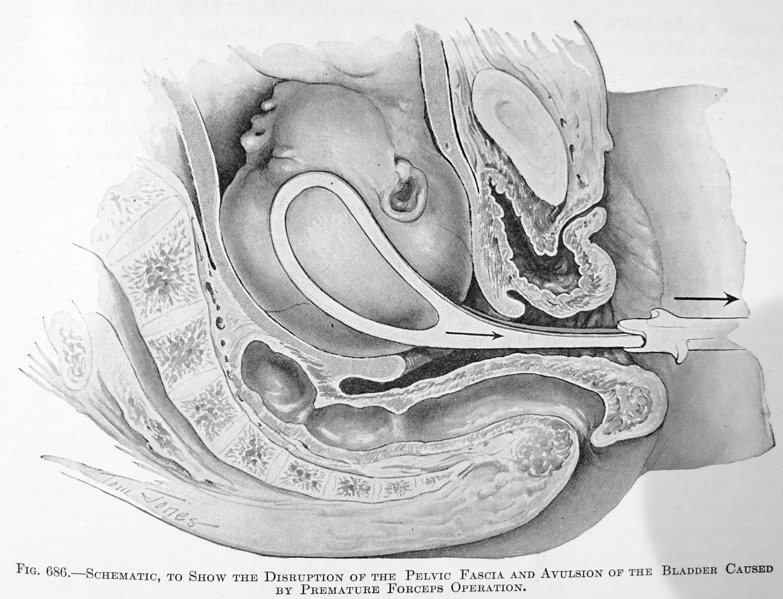
Unfortunately, if the baby is unusually big or the mother’s pelvis unusually small, the baby can get stuck. This describes what was historically known as ‘obstructed labor’. After 4 to 6 days of useless labor, the baby would eventually die and very often the mother would develop a fistula (opening) between her vaginal and her bladder or rectum – a horrific life-long disability. In the modern world, a Cesarean section would be done after some hours of good pushing without any subsequent progress.
Obstetrics and the Hard Job of Fooling Mother Nature
Much  of obstetrics is the story of how hard it is to fool with ‘Mother Nature’. The history of obstetrical forceps is the record of the various ways the medical profession has tried to “work around” the problems caused by that 60-degree angle of the parturient axis. When forceps are being used, the anti-gravitational position of the mother, who must be laying on her back with her legs in stirrups, works directly against the natural and necessary mobility of the childbearing pelvis. It is hard to get an undamaged baby out of the unconscious, anesthetized (or numbed) body of a laboring woman who can no longer push effectively or get her baby out by her own efforts.
of obstetrics is the story of how hard it is to fool with ‘Mother Nature’. The history of obstetrical forceps is the record of the various ways the medical profession has tried to “work around” the problems caused by that 60-degree angle of the parturient axis. When forceps are being used, the anti-gravitational position of the mother, who must be laying on her back with her legs in stirrups, works directly against the natural and necessary mobility of the childbearing pelvis. It is hard to get an undamaged baby out of the unconscious, anesthetized (or numbed) body of a laboring woman who can no longer push effectively or get her baby out by her own efforts.
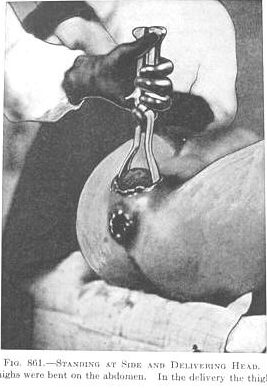
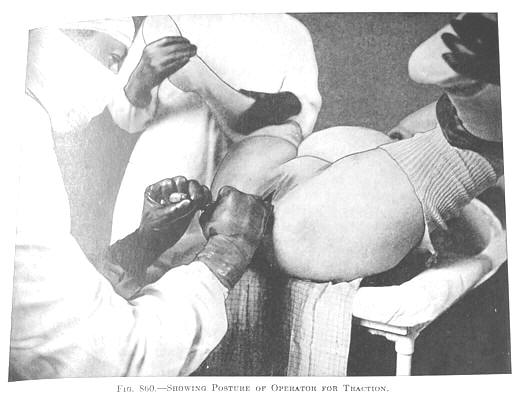
Hard as it is for a mother lying on her back to push her baby uphill against gravity, it is even more difficult for the doctor to pull on the fragile skull of an unborn baby “from below”. He must stand on the floor (directly in front of her pelvis) and pull with enough force to get the baby to go around the corner and emerge at an uphill angle (baby’s head pointing towards the ceiling).
An instrument called a ‘Bill’s axis traction handle’ was invented to transfer some of the force from the lateral pull of the handles, so the direction of the energy force would be diagonally upward, as if the obstetrician was suspended from the ceiling.
But no matter how clever the mechanical devices, obstetrical forceps still depended on the use of force and resulted in many ‘adverse events’. The maternal-infant outcome statistics reflected a high percentage of poor outcomes that were the result of extracting heavily narcotized babies out of the inert bodies of their anesthetized mothers.
The vast improvements in maternity care that were hoped for and eagerly promised by the obstetrical profession in the earliest decade of the 20th century failed to materialize. Instead, scientific studies evaluating the maternal-infant mortality rate associated with the new and improved version of obstetrical care (i.e., after having eliminated physiologic care), revealed a 15% annual increase in maternal deaths for more than a decade (1910-1920+) and 44% increase in neonatal birth injuries over the same period. In 1934, the Committee on Maternal Welfare of the Philadelphia County Medical Society expressed concern that the rate of deaths of infants from birth injuries had increased 62% from 1920 to 1929.
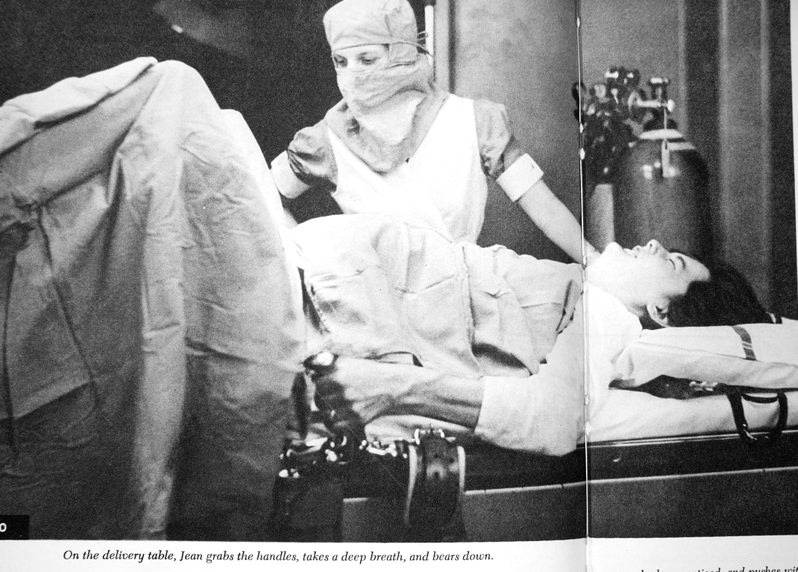
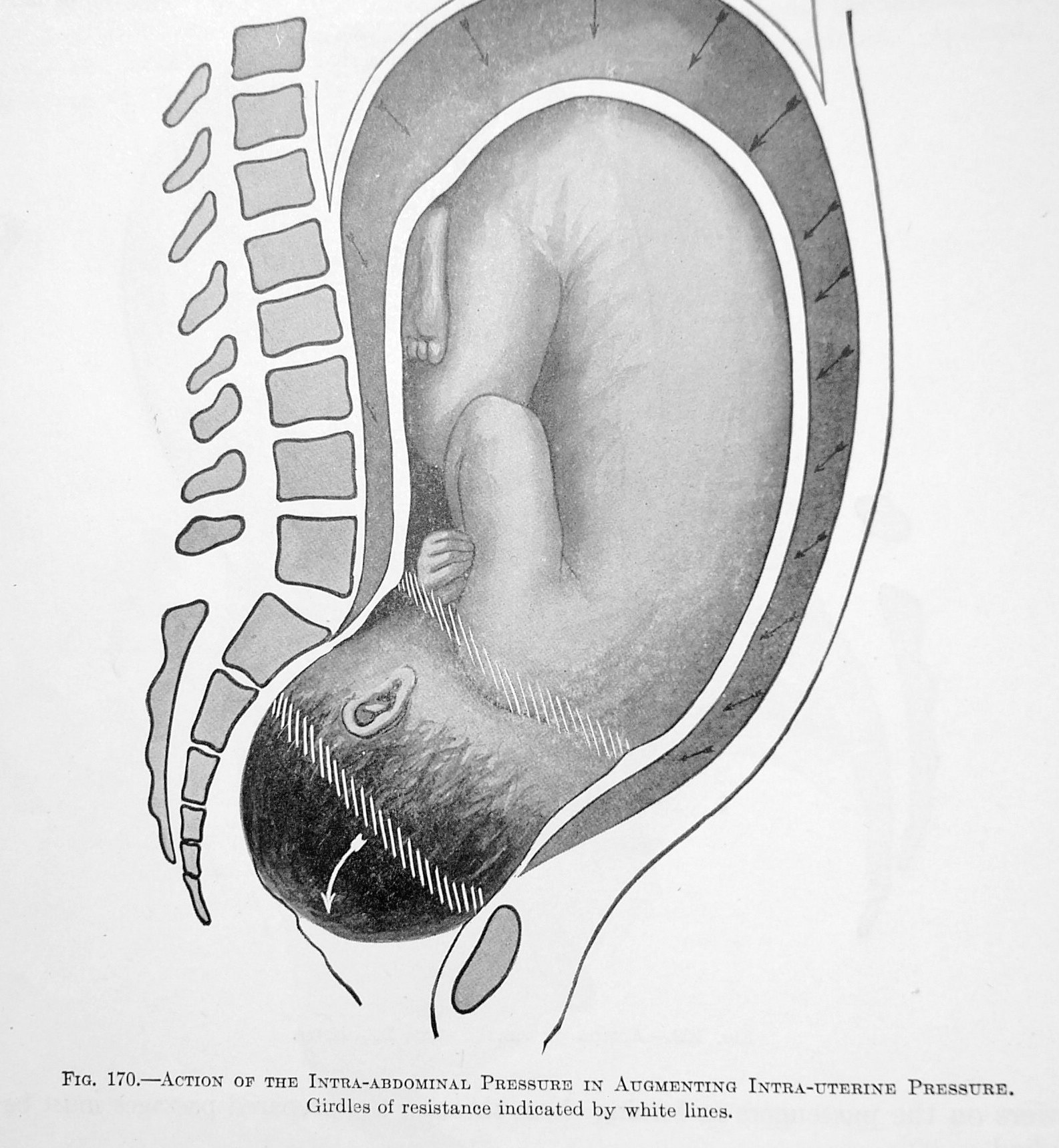
A major reason for the big jump in maternal mortality was the many complications of general anesthesia, such as aspiration pneumonia. This is associated with the loss of the normal gag reflex that occurs when anyone is under the influence of general anesthesia. This potentially fatal complication was much more frequent for obstetrical patients due to the frequent use fundal pressure during the delivery, in which external pressure is applied to the top of uterus.
To make up for the mother’s inability to push effectively while under anesthesia, the obstetrician would instruct the delivery room nurse to stand on a footstool at the side of the delivery table next to the mother’s mid-section, with the mother’s head to the nurse’s left and the mother’s lower body to the nurse’s right. Then the nurse would press the long bone of her right forearm flat against the top edge of the uterus and grasped the handle on the far side of the delivery table with her right hand to anchor her body weight over the mother’s abdomen.
Then the nurse would use the knuckle-side of her left hand, balled up into a fist, to push with all her might against her right forearm. Combined with her own body weight, this wedged her arm down against the upper end (or fundus) of the mother’s contracted uterus. This created a powerful downward force simultaneously with the doctor’s pull from below with forceps, in order to help deliver the baby. Unfortunately, fundal pressure also can cause unconscious patients to vomit and breathe stomach contents into their lungs, which produces a vicious and potentially fatal chemical pneumonia.
The stress of general anesthesia, added blood loss associated with episiotomy, operative delivery and manual removal of the placenta all weakened the mother’s immune system. Invasive procedures, such forceps and inserting the surgeon’s gloved hand up into the uterus to manually remove the placenta, provided unnatural opportunities to introduce infection. All of this made the newly delivered woman more vulnerable to lethal infection. In all too many cases, the lack of effective antibiotics sealed her fate — 23,000 maternal deaths in 1918 — the majority of them caused by a fatal streptococcal septicemia.
“As to maternal mortality, …during 1913 about 16,000 women died..; in 1918, about 23,000…and with the 15% increase estimated by [Dr.] Bolt, the number during 1921 will exceed 26,000.” [Dr. Ziegler, M.D.1922-A]
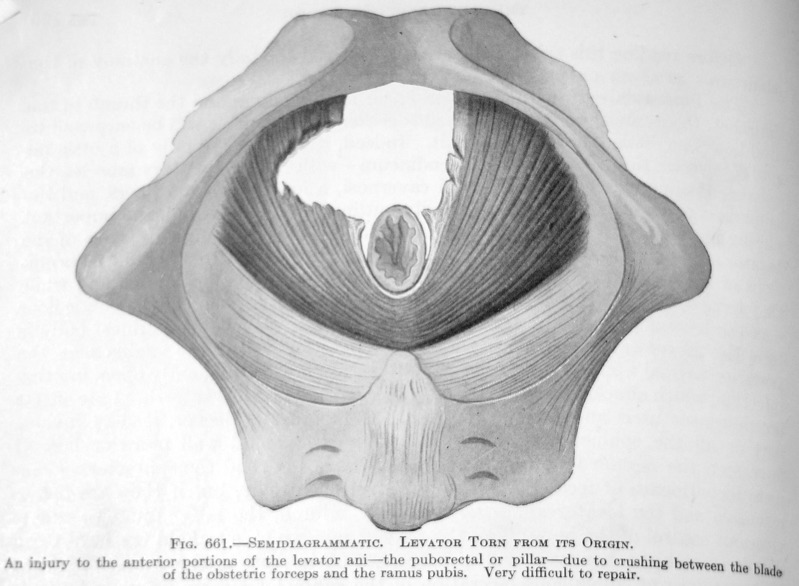
Original caption from 1924 textbook: Fig. 661.
Levator Torn from its Origin.
An injury ….due to crushing between the blade
of the obstetrical forceps…. Very difficult to repair.
This high rate of morbidity and mortality created a false association between birth and bad outcomes, which reinforced the idea that normal childbirth itself was dangerous – so dangerous that women died even when delivered by doctors and surrounded by the gleaming stainless steel and surgical sterility of an operating room. In the minds of both the lay public and the medical profession, this was interpreted as indisputable proof that normal childbirth was inherently pathological.
Ironically, the complications from medical interventions fueled the campaign to further medicalize childbirth, a move that the public and the medical profession both saw as a modern improvement. Without realizing it, obstetrics had become bound by the very laws that governed the error it aimed to correct, that is, efforts by obstetricians to make childbirth safer were themselves adding unnatural risks and resulting in unnecessary complications.
As with the hand-washing issue of the 1840s, the obstetrical profession of the early 20th century largely ignored facts that challenged their assumptions or required them to change course. Obstetricians were very happy with their system, but it continued to be a dangerous time for mothers and babies.
3.
@@@@@@@@@@@@@@@@Temporary photo vault @@@@@@@@@@@@@@@@@@@











How the new American obstetrics, as a surgical specialty, turned healthy laboring women into surgical patients and normal childbirth into a series of surgical procedures
