 Editor’s Note: Slight changes in formatting to make reading easier.
Editor’s Note: Slight changes in formatting to make reading easier.
Summary of the Publication, “Neonatal Encephalopathy and Cerebral Palsy: Defining the Pathogenesis and Pathophysiology,” by the ACOG Task Force on Neonatal Encephalopathy and Cerebral Palsy ~ 2003 ~ Medscape
Peter Van Eerden, MD; Peter S. Bernstein, MD, MPH
July 03, 2003
Introduction
In January 2003, the American College of Obstetricians and Gynecologists (ACOG) and the American Academy of Pediatrics (AAP) released a publication entitled Neonatal Encephalopathy and Cerebral Palsy: Defining the Pathogenesis and Pathophysiology.[1]
The Task Force met over a period of 3 years and worked with expert consultants, conducted a literature review, and received input and endorsements from professional societies and organizations.
It is the most extensive peer-reviewed document on this subject published to date.
The crux of this report is that:
- the majority of newborn brain injury does not occur during labor and delivery.
- …. most instances of neonatal encephalopathy and cerebral palsy are attributed to events that occur prior to the onset of labor.
The report is important for a number of reasons.
 First, it lists criteria to define whether neonatal encephalopathy and cerebral palsy are the results of actions during labor, and it facilitates the understanding of the causes of neonatal encephalopathy and cerebral palsy.
First, it lists criteria to define whether neonatal encephalopathy and cerebral palsy are the results of actions during labor, and it facilitates the understanding of the causes of neonatal encephalopathy and cerebral palsy.
Second, it will hopefully help to reduce future occurrences of these disorders.
Finally, it serves as an invaluable resource to healthcare professionals and the legal system for a better understanding of the events leading to neonatal encephalopathy and cerebral palsy, especially in the face of a bad outcome.
This document is important because failure to adequately educate all of those parties involved in such cases have resulted in substantial financial and emotional cost [Ed. note i.e. malpractice claims)
The endorsements and support that this report has received come from 6 major federal agencies and professional organizations. They include the:
- Centers for Disease Control and Prevention
- Child Neurology Society
- March of Dimes Birth Defects Foundation
- National Institute of Child Health and Human Development
- Royal Australian and New Zealand College of Obstetricians & Gynaecologists
- Society for Maternal-Fetal Medicine
- Society of Obstetricians and Gynaecologists of Canada
This article will serve to review and summarize the findings of this important publication.
 Briefly, neonatal encephalopathy is defined clinically on the basis of a constellation of findings, including a combination of abnormal consciousness, tone, and reflexes, feeding, respirations, or seizures, which can result from many conditions.
Briefly, neonatal encephalopathy is defined clinically on the basis of a constellation of findings, including a combination of abnormal consciousness, tone, and reflexes, feeding, respirations, or seizures, which can result from many conditions.
It may or may not result in permanent neurologic impairment and is not necessarily caused by intrapartum asphyxia.
However, the pathway from intrapartum hypoxic-ischemic injury to subsequent cerebral palsy must progress through neonatal encephalopathy. Hypoxic-ischemic encephalopathy (HIE) is defined as neonatal encephalopathy with intrapartum hypoxia in the absence of any other abnormality.
Cerebral palsy is a chronic disability of central nervous system origin characterized by aberrant control of movement and posture, which appears in early life and is not a result of progressive neurologic disease. Spastic diplegia is the only type of cerebral palsy associated with an acute interruption of blood flow.
The historical factors used to define perinatal asphyxia (ie, meconium, Apgar scores) are not specific to the disease process leading to the neurologic damage. Using these nonspecific markers incorrectly identifies individuals as being exposed to “perinatal asphyxia.”
The criteria to define an acute intrapartum event sufficient to cause cerebral palsy are listed in the report as follows:
Essential criteria (must meet all 4):
- Evidence of a metabolic acidosis in fetal umbilical cord arterial blood obtained at delivery (pH < 7 and base deficit ≥ 12 mmol/L)
- Early onset of severe or moderate neonatal encephalopathy in infants born at ≥ 34 weeks gestation
- Cerebral palsy of the spastic quadriplegia or dyskinetic type
- Exclusion of other identifiable etiologies, such as trauma, coagulation disorders, infectious conditions, or genetic disorders
Criteria that collectively suggest an intrapartum timing (within close proximity to labor and delivery, eg, 0-48 hours) but are nonspecific to asphyxial insults:
- A sentinel (signal) hypoxic event occurring immediately before or during labor
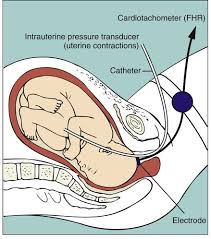
- A sudden and sustained fetal bradycardia or the absence of fetal heart rate variability in the presence of persistent, late, or variable decelerations, usually after a hypoxic sentinel event when the pattern was previously normal
- Apgar scores of 0-3 beyond 5 minutes
- Onset of multisystem involvement within 72 hours of birth
- Early imaging study showing evidence of acute no-focal cerebral abnormality
These criteria are described in detail at the end of the Task Force’s report.
Background
 Term and near-term infants are at relatively low risk for cerebral palsy; however, they still make up at least one-half of all cases of cerebral palsy. Infants weighing less than 1500 grams at birth are a tiny proportion of the birth population, but they experience higher morbidity and mortality, accounting for approximately 25% of all cases of cerebral palsy.
Term and near-term infants are at relatively low risk for cerebral palsy; however, they still make up at least one-half of all cases of cerebral palsy. Infants weighing less than 1500 grams at birth are a tiny proportion of the birth population, but they experience higher morbidity and mortality, accounting for approximately 25% of all cases of cerebral palsy.
Because term and near-term infants make up the majority of all births, the document focuses on neonatal encephalopathy and HIE and later outcome in this group of infants.
Historically, the term “hypoxic-ischemic encephalopathy” arose on the basis of assumptions about the etiology behind an array of adverse neurologic outcomes in infants. Actually defining intrapartum asphyxia was a problem because of lack of direct and sensitive measures.
The criteria used included the words “birth asphyxia” written in the medical record, meconium-stained amniotic fluid, abnormal fetal heart rate during labor, umbilical cord pH and base excess, and Apgar scores. Many reports have subsequently shown that these markers are poorly associated with adverse neurologic outcome.
Some individuals with these exposures have poor neurologic outcome; however, the majority of neurologically impaired individuals were not exposed to these markers. Using a combination of these nonspecific signs may be misleading and may misclassify an infant as having sustained intrapartum asphyxia.
Neurologic damage cannot be attributed to birth asphyxia in the absence of neonatal encephalopathy, and cerebral palsy cannot be attributed to intrapartum events in the absence of neonatal encephalopathy. However, HIE is only a small subset of the causes of neonatal encephalopathy.
 The best available evidence suggests an incidence rate for pure HIE (ie, neonatal encephalopathy with intrapartum hypoxia in the absence of any other abnormality) of approximately 1.6 per 10,000 births.
The best available evidence suggests an incidence rate for pure HIE (ie, neonatal encephalopathy with intrapartum hypoxia in the absence of any other abnormality) of approximately 1.6 per 10,000 births.
Historically, the incorrect assumption that all cases of neonatal encephalopathy resulted from intrapartum asphyxia impeded the search for other causes.
A retrospective case-control study involving 164 cases of neonatal encephalopathy and 400 controls was performed in Perth, Western Australia, from June 1993 through September 1995.
The following conclusions were noted:
- 69% had only antepartum risk factors
- 25% had both antepartum risk factors and evidence for intrapartum hypoxia
- 4% had evidence of intrapartum hypoxia in the absence of pre-conceptional or antepartum factors
- 2% had no recognized risk factors
The strongest antepartum risk factor for neonatal encephalopathy was fetal growth restriction.
- Neonatal encephalopathy of any etiology occurs in approximately 2-8 births per 1000 term infants. It has been shown that most infants with mild to moderate neonatal encephalopathy develop normally.
- Most infants thought to have birth asphyxia do not develop motor or cognitive disabilities unless the event was severe and prolonged.
- Data from the prospective National Collaborative Perinatal Project study have shown that approximately 9% of cases of cerebral palsy are due to possible birth asphyxia.
Cerebral palsy is a chronic neuromuscular disability characterized by abnormal movement or posture appearing early in life and not the result of a recognized progressive disease. Causes {CP} include
- developmental malformations
- coagulation disorders
- metabolic defects
- autoimmune
- infections
- hypoxia in the fetus or newborn.
Circulatory responses to asphyxia include:
(1) redistribution of cardiac output
(2) loss of cerebral vascular auto-regulation
(3) eventual decrease in cardiac output, hypotension, and a decrease in cerebral blood flow
Other non-circulatory factors and unknown factors contribute to neuronal preservation, and so, even when asphyxia is prolonged and severe, most newborns recover with minimal or no neurologic sequelae.
Para-sagittal brain injury is the principal lesion in fetuses older than 34 weeks gestation and manifests as spastic quadriplegia.
Maternal Conditions
The report comments on the association between maternal conditions and neonatal HIE. Third-trimester bleeding caused by placenta previa and placental abruption is often associated with a chronic, long-standing underlying condition that may have resulted in fetal injury prior to any clinical bleeding, and it is seldom associated with neonatal HIE.
 Maternal trauma is seldom a predecessor of HIE. Observational studies have shown an association between hypothyroidism and abnormal neurodevelopment in the neonate; however, evidence that thyroid disorders are related to cerebral palsy are conflicting.
Maternal trauma is seldom a predecessor of HIE. Observational studies have shown an association between hypothyroidism and abnormal neurodevelopment in the neonate; however, evidence that thyroid disorders are related to cerebral palsy are conflicting.
The report concluded that the relationship between maternal epilepsy and mental retardation and the ultimate development of cerebral palsy is likely more of an association than directly causal.
Data are limited with regard to exposure to environmental agents, chemicals, alcohol, and drugs. The report does state that there may be a relationship between cerebral palsy and organic mercury exposure.
Because alcohol and cocaine use may affect neurologic function, it is recommended that these substances be avoided.
There is a link between inflammation, infection, and coagulation disorders, and the development of neonatal encephalopathy and cerebral palsy.
Intrauterine infection (ie, maternal or placental) and inflammation are linked to intraventricular hemorrhage, white-matter damage, periventricular leukomalacia, and cerebral palsy.
It is hypothesized that intrauterine exposure to infection causes fetal production of cytokines, which leads to cellular damage to the fetal brain.
Very-low-birth-weight infants are at a significantly increased risk when exposed to intrauterine infection.
The report proposes several biologic pathways of intrauterine infection and inflammation that lead to fetal and perinatal brain damage:
- Inflammatory responses are mediated by both the maternal and fetal genetically controlled inflammatory process.
- Intrauterine infection may be established either prior to pregnancy or very early in pregnancy and may remain clinically unrecognized.
- The end result of infection and inflammation is revealed by damage from reactive oxygen species and other damaging molecules, altered immune recognition, and apoptosis (programmed cell death).
- Non-infectious causes of inflammation may also play roles in fetal outcome.
 The fetal response to infection and inflammation is analogous to the adult systemic inflammatory response, which occurs during sepsis.
The fetal response to infection and inflammation is analogous to the adult systemic inflammatory response, which occurs during sepsis.
The presence of clinical chorioamnionitis and inflammatory cytokines is associated with an increased risk for the development of cerebral palsy.
In addition to infection and inflammation, the report suggests that maternal coagulation disorders, such as factor V Leiden mutation and deficiencies of antithrombin III and protein C and S, may predispose the fetus to the ultimate development of cerebral palsy.
Also, fetal coagulation disorders may have the same predisposition, perhaps due to thrombosis at the level of the fetal-placental unit causing limitation of oxygen exchange.
Antepartum and Intrapartum Considerations and Assessment
As most cases of cerebral palsy are associated with antepartum factors, rather than intrapartum events, it is important to consider these factors.
Most of these factors are seldom amenable to intervention by the healthcare provider.
These factors include:
- preterm birth
- intrauterine infection
- intrauterine growth restriction (IUGR)
- multifetal pregnancies
- coagulation disorders
- antepartum bleeding
- congenital or genetic anomalies
- infertility treatment

Many infants with cerebral palsy do not have evidence of neonatal encephalopathy, even though these conditions are sometimes considered together.
Risk factors for neonatal encephalopathy include:
- older maternal age
- family history
- maternal thyroid disease
- maternal hypertension
- vaginal bleeding
- Infertility
- fetal growth restriction
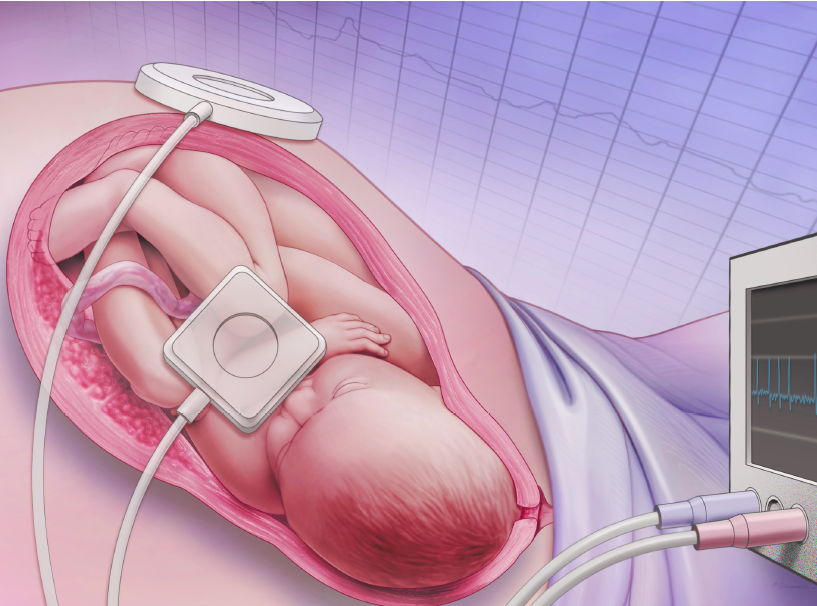
Since the advent of electronic fetal heart rate monitoring, there has been no change in the incidence of cerebral palsy.
Abnormal fetal heart rate patterns have a high false-positive rate and are poor predictors of the subsequent development of cerebral palsy.
For intrapartum asphyxia to develop in a previously normal fetus, an acute sentinel event must occur.
Most fetuses with abnormal fetal heart tracings that present to the hospital may have already experienced damage, and prompt delivery by cesarean section may not improve the outcome.
Examples of episodes of acute interruption of blood flow to the fetus include:
- cord prolapse,
- uterine rupture
- maternal cardiopulmonary arrest
Most severe forms of these situations result in fetal death.
 Of those fetuses that survive, very few develop cerebral palsy. In other words, most neonates that survive an acute catastrophic hypoxic event usually have normal neurologic outcome. The results of these insults likely depend on many other poorly understood factors.
Of those fetuses that survive, very few develop cerebral palsy. In other words, most neonates that survive an acute catastrophic hypoxic event usually have normal neurologic outcome. The results of these insults likely depend on many other poorly understood factors.
Fetal Considerations
Multiple gestation is a risk factor for cerebral palsy. This risk is significantly higher for monochorionic twins, likely due to increased vascular connection and other factors
For example:
- IUGR
- complications of velamentous cord insertion
- premature rupture of membranes [PROM])
There is also a risk of neurologic compromise in the case of fetal death of 1 twin, which is particularly high in monochorionic twin gestations. Even cases in which the twins were delivered immediately by abdominal delivery, the surviving twin still suffered neurologic damage.
There are no identified strategies to reduce these outcomes in twin gestations.
- Most IUGR or small-for-gestational age fetuses do not develop cerebral palsy.
- Most newborns destined to develop cerebral palsy are of normal birth weight.
- Cerebral palsy is more common in preterm infants than in IUGR infants.
The precise linkage between cerebral palsy and IUGR fetuses is incompletely established. Many causes can give rise to IUGR in the fetus, and it is important to take this into account when trying to make an association between neonatal encephalopathy and cerebral palsy.
With respect to meconium, the report states that it is a poor predictor of long-term neurologic outcome, and passage of meconium basically is a known normal physiologic function.
In post-term infants, the underlying condition of the fetus is more important than simply being post-term.
Neonatal Assessment
 Clinical signs in the delivery room of a seriously depressed infant should prompt an immediate effort to gather information to understand the etiology, especially after an uncomplicated delivery.
Clinical signs in the delivery room of a seriously depressed infant should prompt an immediate effort to gather information to understand the etiology, especially after an uncomplicated delivery.
This evaluation should include:
- Examination of the placenta, membranes, and umbilical cord
- Samples of umbilical artery blood for pH and base deficit
- Culture between the membranes, after splitting the amnion from the chorion
- Close review of the maternal and family history
- Newborn blood cultures and C-reactive protein
- Evaluation for maternal and fetal thrombophilia
A low 5-minute Apgar score is a poor predictor of later neurologic dysfunction and cerebral palsy.
Approximately 75% of children with cerebral palsy have normal Apgar scores at birth.
A low Apgar score was originally used as a criterion for defining birth asphyxia. This inaccuracy led to the publication of “Use and Misuse of the Apgar Score” (1986) and “Use and Abuse of the Apgar Score” (1996) by the AAP and ACOG. These documents are supported by the current report.
It does note that an Apgar score of 0-3 after 5 minutes remains an appropriate potential marker of intrapartum asphyxia.
Neuroimaging techniques such as ultrasonography, computed tomography, and magnetic resonance imaging reveal specific findings over a period of time, which may be helpful in determining the timing and severity of the injury. However, they can only serve to approximate a window in time for the injury, rather than determine the precise moment the injury occurred.
Electroencephalography (EEG) does not indicate the cause of encephalopathy, and a normal EEG in the first 7 days is evidence against an acute intrapartum event.
Placental pathology may be helpful in suggesting an infectious cause and is essential in determining chorionicity in multifetal gestations.
The clinical utility of nucleated red blood cells and lymphocytes is still considered investigational.

Genetic, Anatomic, and Metabolic Etiologies of Neonatal Encephalopathy
There are many genetic, metabolic, and anatomic factors that may contribute to the etiology of neonatal encephalopathy. Because many of these conditions likely overlap, they may be difficult to differentiate.
Many of these abnormalities are important to consider because they are amenable to treatment if diagnosis is made before irreversible damage.
Many of these disorders are associated with neonatal hypoglycemia and hyperammonemia. There are many disorders of amino acid metabolism that will manifest themselves in the first 4 weeks of life, most of which are autosomal recessive.
In addition,
- degenerative disorders
- disorders of lower motor neurons
- primary anatomic abnormalities
- chromosome abnormalities
need to be considered.
Finally, it is important to recognize that there are different degrees of genetic resistance and susceptibility to external forces.
With a better understanding of the pathophysiology and genetic susceptibility, it may be possible to understand why certain fetuses are more susceptible to toxic agents than others.
Obstetric Pharmacologic Approaches to the Prevention of Neonatal Hypoxic-Ischemic Encephalopathy:
Current Status and Future Direction
 There is no evidence to support that neonatal encephalopathy or its subtype, hypoxic-ischemic encephalopathy, can be prevented by maternal pharmacologic treatment. Maternal phenobarbitol has been evaluated in clinical trials and found to be ineffective. Glucocorticoids have been found to protect against neonatal intraventricular hemorrhage.
There is no evidence to support that neonatal encephalopathy or its subtype, hypoxic-ischemic encephalopathy, can be prevented by maternal pharmacologic treatment. Maternal phenobarbitol has been evaluated in clinical trials and found to be ineffective. Glucocorticoids have been found to protect against neonatal intraventricular hemorrhage.
Betamethasone specifically has been associated with decreased incidence of periventricular leukomalacia in very preterm infants.
Some data also suggest that exposure to magnesium sulfate is associated with a decreased incidence of cerebral palsy, and trials are underway looking at this association.
However, because of the low incidence of neonatal encephalopathy, and particularly that being secondary to intrapartum asphyxia, it would be difficult to perform a controlled trial if there was a promising pharmacologic agent.
Conclusions
The task force concludes by providing a list of potential studies that would be helpful in elucidating more clearly some of the concepts discussed in the report.
Hopefully, this important report will shed light on this confusing area of maternal, fetal and neonatal medicine and help to better characterize the etiologies of neonatal brain injury.
Through better research in this area, we may be able to prevent some of the high costs of cerebral palsy to patients, their families, and to society.
To purchase copies of the complete report, contact the ACOG Distribution Center at 800-762-2264 ext. 277 and ask for item #AA432, or order online at sales.acog.org.
Follow the path from the ACOG Bookstore to “Professional Publications” to “ACOG Guidelines.”
 References
References
- Task Force on Neonatal Encephalopathy and Cerebral Palsy Staff American College of Obstetricians and Gynecologists with the American Academy of Pediatrics Staff. Neonatal Encephalopathy and Cerebral Palsy: Defining the Pathogenesis and Pathophysiology. The American College of Obstetricians and Gynecologists. Washington, DC; 2003.
Medscape Ob/Gyn. 2003;8(2) © 2003
Medscape Cite this article: Summary of the Publication, “Neonatal Encephalopathy and Cerebral Palsy: Defining the Pathogenesis and Pathophysiology,” by the ACOG Task Force on Neonatal Encephalopathy and Cerebral Palsy – Medscape – Jul 07, 2003.
