word count ~ 3860 Jan 17, 2025
Chapter Seven
The Seventies – paradigm shift par excellence!
To make it easier to follow the events of this 30-year era, lets considered the story decade-by-decade, beginning with 1970s.
In the early 1970s there were no less than three new kids on the block — electronic fetal monitoring, epidural anesthesia and the malpractice “crisis”. The biggest and most obstetrically influential was continuous electronic fetal monitoring (EFM), which was tightly paired with that familiar obstetrical staple – surgical birth as either forceps or Cesarean section. However, women were most impressed with epidural anesthesia, which permitted they to be “awake and aware” and have their husband with them. As for the malpractice crisis, lawyers and hospital administrators were zoned in on that.
Electronic Fetal Monitoring

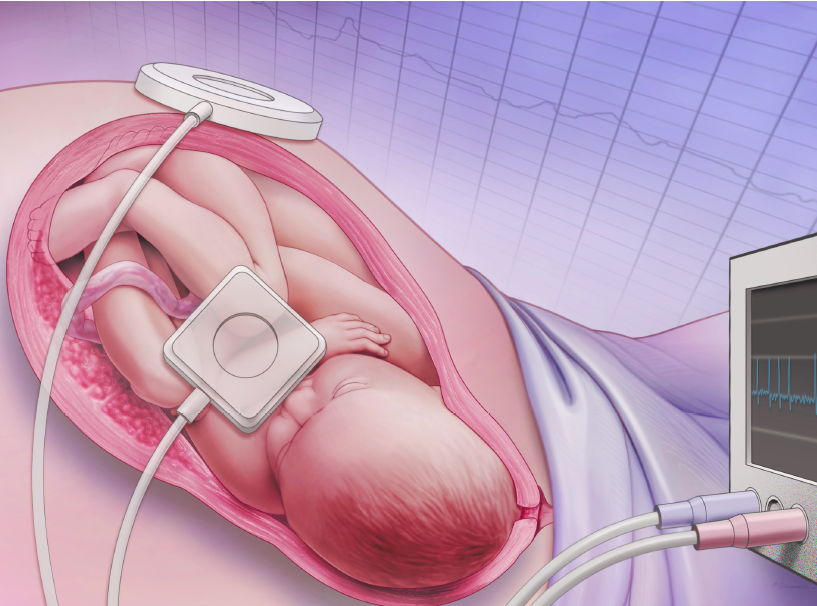
Continuious EFM was billed as the answer to every obstetrician (and every family’s) prayer – the magic bullet, the ‘cure’ for birth-related brain injuries. It was believed that the use of continuous EFM could detect fetal distress before it caused any permanent damage.
The nifty trick was to catch potential brain damage before it happened and rescue the baby via emergency CS. Its promise was simple but profound – the marriage of EFM and liberal use of CS was to virtually eliminate birth-related brain damage and cerebral palsy. EFM made maternity care out side of the acute care hospital unthinkable.
As the use of EFM became more common, there was increasing pressure for Cesareans to be employed whenever continuous EFM indicated a possible abnormality or fetal distress. It was this idea that gave rise to the obstetrical slogan of “When it doubt, cut it out”.
Very quickly the obstetrical standard of care expanded to include the routine use of continuous EFM, in combination with immediate access to and liberal use of Cesarean surgery. It was suppose to be so easy – just hook every mother up continuously electronic fetal monitoring and sit back and watch the strip scroll by. However there were a few unexpected problems, which doctors, for the most part, kept to themselves.
 As with any new technology, there were bugs and unintended consequences. Interpreting EFM tracing was not as straight forward as first assumed. There were many widely differing opinions on just what was and was not a ‘normal’ versus ‘abnormal’ as recorded on the EFM printout. As a result, the emergency CS rate shot thru the roof as obstetricians mistook the many normal variations of FHR pattern as potentially “ominous”.
As with any new technology, there were bugs and unintended consequences. Interpreting EFM tracing was not as straight forward as first assumed. There were many widely differing opinions on just what was and was not a ‘normal’ versus ‘abnormal’ as recorded on the EFM printout. As a result, the emergency CS rate shot thru the roof as obstetricians mistook the many normal variations of FHR pattern as potentially “ominous”.
For the first 20 years, the EFM machines were very finicky and the mother had to lie real still, preferably on her back, to get a good reading. It was not widely recognized at the time or, at least not admitted to, but the technology to detect fetal distress also created or contributed to fetal distress.
 But still it seem that EFM was the beginning of something great. After a futile search by generations of obstetricians for a way to prevent brain damage and cerebral palsy, obstetricians were convinced that they had finally achieved this most admirable goal. EFM would, finally, categorically and for all time, eliminate these newborn tragedies and the obstetrician’s anxiety of being wrongly accused by the parents or the hospital for some perceived mismanagement of the labor or birth. Unfortunately, celebration over this perceived victory of the brutish forces of nature was muted by the gathering storm and long-term fallout of the 1976 malpractice crisis.
But still it seem that EFM was the beginning of something great. After a futile search by generations of obstetricians for a way to prevent brain damage and cerebral palsy, obstetricians were convinced that they had finally achieved this most admirable goal. EFM would, finally, categorically and for all time, eliminate these newborn tragedies and the obstetrician’s anxiety of being wrongly accused by the parents or the hospital for some perceived mismanagement of the labor or birth. Unfortunately, celebration over this perceived victory of the brutish forces of nature was muted by the gathering storm and long-term fallout of the 1976 malpractice crisis.
Epidural Anesthesia
Women and their families were not as impressed with EFM as they were the change to “awake and aware” labor and birth practices and the ability to have their loved ones present during the birth. There were two specific reasons for relaxed hospital policies. Fear of puerperal sepsis had been cured by access to effective antibiotics, so the isolation of maternity patients no longer legally mandated by state laws. Second, the use of spinal and epidural (instead of general) anesthesia made it more sensible for fathers to be present. Both of these substantive changes happily coincided with the non-obstetrical phenomenon of childbirth education classes and the resulting demand of childbearing women to have their husbands involved in their labor. A very small number of women even managed to have a ‘natural’ birth in this medicalized environment, but this rare oddity did little to influence obstetrical customs.
Malpractice Litigation
Last in our trilogy is the ‘bad humbre’ — the malpractice crisis of 1976. Over the last three decades, the issue of ‘risk reduction’ had begun to organize all medical care around preventing malpractice litigation.
Characterizing EFM as the “big gun” of obstetrics is more metaphorically accurate than one might suppose, as EFM and the malpractice crisis both landed right in the middle of the 1970s. EFM, marketed as the cure-all, made obstetricians uniquely vulnerable to litigation as it left a paper trail that could be subpoenaed and argued over in court by competing and diametrically-opposed ‘expert witnesses’. The combination of hard-copy ‘evidence’ and the wide variation of professional interpretation was a particularly deadly mix. EFM became like a double-barreled shoot gun with one barrel cocked at the culprit of brain damage and cerebral palsy, ready to shoot to kill, and the other barrel twisted backwards, with the obstetrician dead center in his own sight. The very thing that was seen to ‘save’ the reputation of the obstetrician was also capable of killing it off.
Labor and Birth, 1970-style
Unfortunately, the experience of the ‘awake and aware’ labor patient was not as different as people imagined. Aside from the change to epidural anesthesia and the presence of father (and if they were lucky, maybe one or two other family members) obstetrical management by the end of the 1970s was pretty much the same as the 1930s. Even though infection was no longer the central and organizing problem in hospital childbirth, labor was still organized around its cure, which was to say that birth was still being conducted as a surgical procedure.
Pregnant women were still admitted to hospitals to have their labors managed by nurses as a medical condition. Mothers were still kept in bed, still had no control over what happened to them, still had their water broken, still shaved and given enemas, still required to be NPO (no food or drink), with the exception of ice chips. Only now, in addition to the already substitive list, they also had IVs going, an epidural catheter in their back, blood pressure cuffs permanently affixed to their arm, and the ubiquitous EFM leads wrapped around their middle. All this was accompanied by the beep-beep of the electronic fetal monitor, which is the first thing everyone looked at when they entered the room and the last thing they glanced at as the left. In fact, the EFM got far more attention than the mother. Right use of gravity was not a part of this picture.
More of an issue was that these ‘improvements’ were not as dramatically effective as obstetricians first imagined. The decade of the 1970s ended with a whimper rather than a roar. In spite of having the best control and manipulation of labor, birth and unborn baby in the history of the world, obstetricians at the end of that decade still could not predict or prevent labors that failed to progress, babies that developed ‘fetal distress’ with no explanation and women who continued to have massive hemorrhages after an apparently normal delivery. New mothers sometimes got infections, which were quickly treated by antibiotics, but occasionally there still was a maternal death. The same long-term gynecological complications such as pelvic floor damage and incontinence persisted. The only good news was that the stillbirth rate continued to drop. But the unexpected bad news was that the stubborn problem of ‘birth injuries – brain damage and cerebral palsy – continued to plague them even with intrapartum use of continuous EFM.
The Eighties
The most remarkable characteristic of the 1980s was the inventive combining and clustering of the newer or upgraded technologies – genetic testing, EFM & ultrasound, improved techniques and equipment for epidural anesthesia, a big increase in labor induction and augmentation, prostaglandins for cervical ripening, accompanied by an ever expanding list of reasons to induce labor and a CS rate around 25 %, primarily due to false-positive reading from the EFM.
Induction – Baby on Demand
Inducting or speeding up labor with Pitocin became much more popular in the late 1970s and early 1980s. A big contributor to this was the development and aggressive marketing of the easier to use angio-cath, which was a replacement for the metal IV needle. This plastic catheter meant the patients no loner had to have their arms tied down to an “IV board” for fear that if they accidently bent their elbow, the IV needle would go straith thru their arm. This was a creepy enough thought that patients and nurses alike were far happier with the new none-needle needles. This made the IV administration of Pitocin more acceptable.
In the 1980s the development of the IV pumps, which help to ‘titrate’ or carefully measure out an exact dose, make the use of Pitocin a bit less risky, at least from the standpoint of hospital staff error. However, Pitocin is a powerful drug and there is no way to tell ahead of time if a laboring women is overly sensitive to it. The product insert by Parke-Davis pharmaceutical company that ships with every package of Pitocin lists no less than 11 serious or fatal “adverse reactions” (i.e., complications or death) for mothers and 7 for unborn or newborn babies, including a tetonic contraction lasting up to 10 minutes, fetal distress, amniotic fluid embolism, placental abruption, uterine rupture, death and permanent neurological damage for either mother or baby.
VBAC – A Long Over-due Reversal of an Outdated Policy
The high Cesarean rate triggered the reversal of a long-standing obstetrical tradition – the idea that ‘once a Cesarean, always a Cesarean’ came under questions after 50 years of automatic repeat CSs. With a CS rate of 25 %, about 20% of women were having a second pregnancy after a Cesarean. A modest number of these women were so disturbed by the original CS, or so distraught at the thought of another one and/or so committed to having a normal vaginal birth, that they refuse to sign up for a repeat CS and convinced midwives to let them give birth at home. That got the attention of the obstetrical profession. After these doctors regained consciousness (many fainted when they heard the news!), there was a long-overdue reassessment. After publishing a few positive studies on VBAC (vaginal birth after cesarean), it was determined that the risk was relatively minor and so hospital VBAC became the standard of care for the obstetrical profession.
“For the first time, the technology of ultrasound allows the fetus to be the primary patient of the obstetrician” Preface of Williams obstetrical textbook, published in early 1980s [emphasis added]
However, the hot new technology of the eighties was prenatal evaluation and genetic testing. Before the decade was over, the combination of ultrasound and genetic testing (such as alpha-feto-protein and amniocentesis) had become the new standard for prenatal care. This made targeted termination of pregnancy possible when it was clear the baby had a serious congenital anomaly. A side effect of genetic testing was that the number of fragile fetuses who would have became distressed in labor or would have been stillborn was significantly reduced, which improved outcome statistics for live births in all industrialized countries.
Another major area of change was hospital economics. During the 1970s and 80s old charity hospitals were rapidly being improved and converting to ‘for profit’ institutions. A concerted effort to liberalize the social aspect of hospitalization was brought on by economic competition with other hospitals (and the threat of home birth!). Improvements included new LDRs (labor-delivery-recovery rooms), which architecturally healed the artificial split between ‘labor’ and ‘delivery’. An LDR is basically a controlled and equipped surgical environment (same as a delivery room) that has been modified to accommodate the pre-birth activities of labor, the surgical procedure of ‘delivery and immediate recovery for both new mom and new baby. LDR standards are the same as any OR and so the bed, floors, ceiling height were all built to surgical specifications and all surfaces were scrubbed and disinfected between each patient.
The normal delivery room equipment and surgical instruments were hidden in cupboards with attractive wooden doors. Equally important was a special (and especially expensive) motorized labor bed that quickly turns, at the press of a button, into a waist-high delivery “table”, complete with stirrups. Instead of putting women on stretchers and moving them down the hall to the delivery room (which left dad behind), they brought the delivery room and OR table to both mom and dad. This was part of an industry-wide effort by the hospital PR folks to be perceived as family friendly, which included a sprucing up the LDR with flowered bedspreads and other window dressings, moving in a rocking chair and maybe a daybed for dad. This was not an idea that obstetricians had much affection for, but the public really embraced them whole heartedly.
Labor and Birth, Eighties-style:
As for what the fashion conscious, ‘awake and aware’ labor patient of the 80s should wear to have a baby, it was still an ugly and immodest hospital gown. Proper accessories for an UHG (ugly hospital gown), were EFM straps in attractive shades of baby pink and power blue. The medical management in 1980 was, well, even more medical than before. By 1980s threat of malpractice litigation had heated up and was making everyone paranoid. Risk reduction was ‘hot’, physiological management was definitely not.
In fact obstetrical interventions were on an ascending course — ever-increasing in number and invasiveness, with ever widening and relaxed criteria for surgical interventions. Mothers were still required to be NPO (no food or drink) with the exception of ice chips. On a brighter note, many hospitals changed the full public shave to the less invasive “Poodle clip” and exchanged the big soapsuds enema for a small disposable “Fleets” enema. Obviously the idea that the rectum should properly be an ‘exit-only orifice’ had not yet come into its time.
In theory laboring women were ‘allowed’ to walk around, but in practice, as labor progressed they were eventually hooked up to a half dozen medical devices – two electronic fetal monitoring leads, IV and Pitocin administration equipment, epidural anesthesia catheter and administration pump, automatic blood pressure cuff, pulse oximetry, Foley catheter with urine bag hanging on the bed rail. Needless to say, all this ‘stuff’ held them hostage in bed for at least 98% of the total labor.
As if they was not already wired for sound, another ‘refinement’ of the period was the increasing use of the internal fetal monitor lead (which screwed into the unborn baby’s head with a tiny little medal corkscrew) and the intrauterine pressure catheter or ‘IUP’. The IUP required a water-filled tube to be inserted up into the laboring uterus, with the other end hooked up to a complicated hydraulic pressure gauge mounted to the bed at exactly the same height as the mother’s uterus when she was lying down (and cautioned to stay still so as not to screw up the equipment!). Of course both these invasive forms of EFM required the mother’s membranes to be artificially broken, so these leads and tubes could be inserted up inside them. And sadly, for many, this tangle of tubes and wires was topped of by an oxygen mask when the inevitable signs of fetal distress were noted, a frequent result of a supine position (lying on the back) and the depressive effect of multiple doses of narcotic drugs.
Obviously maternal mobility, right use of gravity and other aspects of physiological management were still not a recognized part of obstetrical care. Nor were meeting the social and psychological needs of the mother acknowledged to be important or contribute to safe, satisfying and non-surgical outcomes.
More than a century had pasted since obstetricians recommended that childbearing be conducted as a surgical procedure to protect women from the epidemic infections of hospitalized childbirth. A hundred years later, that custom that continued to be the organizing principle of obstetrics and the central billing unit of maternity care. Forceps were being used less and less, primarily due to concerns of malpractice liability. Of course, this meant that Cesareans were being done far more often and with less good reason. Induction of labor and scheduled or ‘elective’ Cesareans were now being recommended with increasing frequency for unusual or “risky” situations: Breech, twins, big baby, premie baby, older mom, hypertension, diabetic, etc.
By now the background rate of CS was about 20%, with some years going as high as 25%. Episiotomy was about 75% for first time mothers and about 50% for multips. Forceps were used in about 30% of births. Unfortunately, many of the problems that strict obstetrical management was suppose to prevent – brain damage, cerebral palsy, pelvic floor damage – continued to occur, in spite of ultrasound evaluation of fetal position and size, NSTs and increasing inductions of labor, continuous EFM, internal EFM leads and expanded reasons for Cesarean delivery.
Obstetricians despaired.
The Nineties
1990 – 2000 ~ The nineties were discouraging to many who had spent the previous decades working towards the liberalization of obstetrical policies and reduction of surgical births. For those who longed for a reversal of the run-away medicalization, it was depressing to see that virtually every healthy labor woman was being harpooned to the bed in a tangled twisted web of electronic wires, tubes and catheters, with the ubiquitous machine that goes “bing” droning on and on in the corner, the center of everyone’s attention.
However, there seemed to be a confluence of patient anxiety with obstetrician anxiety. Women stopped complaining about the restrictions of medicalization and started asking for more – more tests, more inductions, more assurance their baby was OK, even if it meant twice weekly trips to the doctor for NSTs during pregnancy and being arc-welded to the electronic fetal monitor during labor. But the biggest difference was that more women were asking for more and earlier epidural anesthesia. It was now ‘in’ to have an epidural, so much so that women who voiced a desire for a ‘natural’ birth were told by other women that they would be nuts to even try. The advice was blunt “Get your epidural in the parking lot”. By the end of the decade, many hospitals had a 95% epidural rate. In fact, the obstetrical profession had been so successful at marketing epidural anesthesia as the “Cadillac of childbirth”, that a new medical profession arose to meet the growing need – OB anesthesia is now a separate sub-specialty for anesthesiologists.
The pernicious influence of run-away malpractice litigation, increasing in number and in amount of jury awards, thoroughly poisoned the water that obstetrician swam in. Psychologically-speaking, the operative words were tight, tighter and tightest – everything in OB was tightly organized around malpractice risk reduction. The astute reader will no doubt be able to predict what comes next – MORE of everything, with a few new bells and whistles. Obstetrical technology was still king, but for the most part, the ‘cutting’ edge’ was still refining machines and methodologies already in use – color and 3-D ultrasound, telemetry leads for continuous EFM and toward the end of the decade, the first prototype of a fetal pulse oximetry, which is an electronic devise that monitors the oxygen saturation of the unborn baby’s blood. Like the intrauterine pressure catheter, it is yet another tube that is pushed up into the laboring uterus and hooked to a read-out devise.
Between 1990 and the year 2000, greater medical scrutiny was focused on prenatal testing for Group B Strep (GBS) and Gestational Diabetes (GDM) and treatment for these conditions became the ‘standard of care’. Routinely stripping membranes weekly to prevent post-dates became popular as well as the regular induction of labor for all women who had not delivered by 41 weeks. In addition to prostaglandin gels to ripen the cervix for induction, the off-label use of Cytotec (a drug manufactured for stomach ulcers which caused miscarriages in pregnant women) was considered by many obstetricians to be a miracle drug to kick-start an induction. Some women delivered in an hour after it was inserted into their vagina and it only cost 27 cents a pill (it was described by one OB as “ungodly cheap”).
Reversal of a Reversal
And another unusual reversal occurred – a reversal of a reversal if you will. The VBAC issue was turned on its head by the end of the millennium and the hot new policy for the year 2000 was the same old policy of “once a Cesarean, always a Cesarean” of the 1930s. This was a curious turn of events, with a ‘multi-factorial basis’, as the say in scientific circles. There was one part the hubris of more than a decade of treating post cesarean labors as “no different” than any other labor, which was to say, the same extreme medicalization with the same misuse of Cytotec, induction, lack of physiological process, counter-productive management, wrong use of gravity, etc and (no surprise!), there were more uterine ruptures (up to 15 times as many) than spontaneous labors.
Another factor was a totally unjustified change from the classical two-layer suturing technique for cesarean incisions to a single layer technique that was suppose to be faster, use less suture material (cheaper) and reduce the risk to the doctor of finger sticks (an issue if the mother was HIV positive). However, rupture rates are 2 to 5 times greater with single layer closure. Then there was the malpractice crisis – according to lawyers, a VBAC rupture case is a lawsuit on steroids. And in 1998 ACOG changed its official policy so that doctors were required to actually be in the hospital during the entire labor. This was a real disincentive and began to slowly reverse the engines, reducing the number of VBACs and increasing the number of repeat CS.
As for cutting edge techy-toys in the 1990s, many of the new idea were embarrassingly low tech. Amnio-infusion was to prevent respiratory problems for babies associated with meconium. It used a tube to run warm water up into the uterus to wash out the meconium (the sterile contents of the unborn baby’s intestine which is irritating to the lungs and can cause a chemical pneumonia). IV antibiotics were routinely given to GBS+ mothers during labor. Perhaps the only bright spot was that many hospital stopped shaving off the pubic hair of women in labor and dropped the compulsory labor enema. But in every other way, it was more and more and more intervention. The CS rate was about 24 %, forceps about 12%, episiotomy somewhere between 35 and 75%, induction about 20%.
And so we ended the 20th century where we began – labor as a medical condition, birth as a surgical procedure, the classical promise of obstetrics unfulfilled. The total elimination of all childbirth-related complications and the guarantee of a perfect baby every time did not come about as hoped. In spite of having the best level of control over labor, birth and the unborn baby ever to occur in the history of the human species, obstetricians at the end of the 20th century still could not predict or prevent labors that failed to progress, babies that developed ‘fetal distress’ with no explanation and women who continued to have massive hemorrhages after an apparently normal delivery. New mothers sometimes got infections, which were quickly treated by antibiotics, but occasionally there still was a maternal death. The same long-term gynecological complications such as pelvic floor damage and incontinence persisted.
When your best still isn’t good enough ….
And that old nemesis – the triade of brain damage, cerebral palsy, pelvic floor damage – all continued to happen in spite of the ability of ultrasound to evaluation of fetal size and position, non-stress testing, increased inductions of labor, intrapartum IV antibiotics, amnio-infusion, continuous EFM, internal EFM leads, fetal pulse oximetry and massively expanded reasons for Cesarean delivery.
Despair was an inadequate concept to describe the frustration of the obstetrical profession.
