Word count 4121 Jan 17, 2025
Chapter Nine

Vagina By-pass Surgery:
What it actually means for the childbearing woman when her baby is delivered by Cesarean section
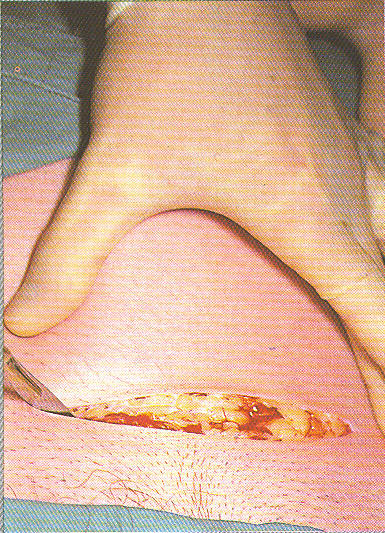
The first incision of Cesarean surgery into the skin of the mother’s abdomen
The last of our three areas of scrutiny is Cesarean section, reasons why such surgery would be performed and the immediate, delayed and downstream consequences of its use.
In the obstetrical community Cesareans are sometimes referred to as “vaginal by-pass surgery”. According to former ACOG president in 2000 the vaginal birth vs. Cesarean question has a simple answer:
Dr. Harer: “Yes, for the baby, the risks are far higher for vaginal delivery … than elective cesarean section at term.
For the mother, the immediate risks for a cesarean section are a little higher …. but the longer term … risks of pelvic dysfunction, incontinence … those risks are higher for vaginal birth.
Over the long term I think that the risks balance out, that there really is no big difference” (between vaginal by-pass surgery & normal birth).” [GMA interview / Dian Sawyer, 2000]
A Cesarean every 39 Seconds
There are 4 million births a year in the US. With a 26% Cesarean rate, it is the most frequently performed major surgery in the US. Or as an ad in obstetrical journal proclaimed: “a scar is born every 39 seconds”. [ReJuveness by RichMark International Corp – statistics based on 1995 CS rate]
This statistic was for 1995, which means that 10 years ago American obstetricians were already doing 80 Cesareans every hour, round the clock, 365 days a year. By 2005, a Cesarean scar is no doubt born every 25 seconds, which helps to explain how we can spend 20% of our entire healthcare budget on maternity services.
Obviously, an increasing number of obstetricians believe that elective cesarean is safer and better than vaginal birth and should become “standard”. This is the same recommendation first given fifteen years ago in the NEJM paper by Drs Feldmen and Friedman (“Prophylactic Cesarean Section at Term?”).
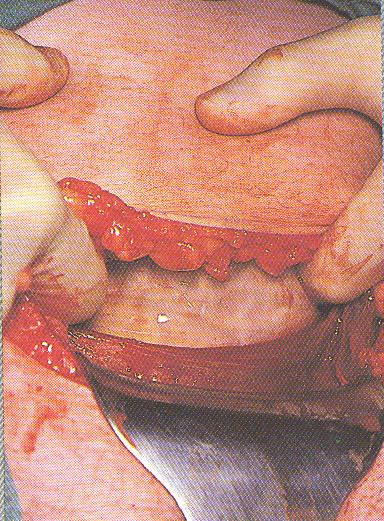
The obstetrical surgeon pulling back the layers of skin, muscle and fat tissue of the mother’s abdomen so he can make the incision into her uterus and extract the baby’s head with forceps and pull the baby out.
A mere three years later, the ACOG Ethics Committee validated this idea in a ruling that determined it to be ethical for obstetricians to perform ‘patient-choice’ cesareans.
This was explained, in part, by the dubious notion that it was impossible to make an informed choice between vaginal birth and elective CS because “the case is complicated by the lack of data on the risks and benefits of Cesarean vs. vaginal delivery”. [Ob.Gyn.News; “C-Section ‘On Demand’ Can Be Ethical: ACOG” Dec 1, 2003.
This reminds me of a statement made by a NASA spokesman after the manned space missile blew up:
“Organizational decisions detrimental to safety were allowed to develop” ~ NASA report on the Challenger disaster
From the standpoint of a scientist (or any other honest broker), this is an “Alice in Wonderland” statement.
Incontrovertible evidence for the danger of Cesarean section is wide, deep and historically universal. Contrary to ACOG’s caviler comments, the scientific evidence isn’t complicated or difficult to understand, it isn’t scientifically controversial, it isn’t a secret, it isn’t rare.
But it also isn’t what many obstetricians want to hear.
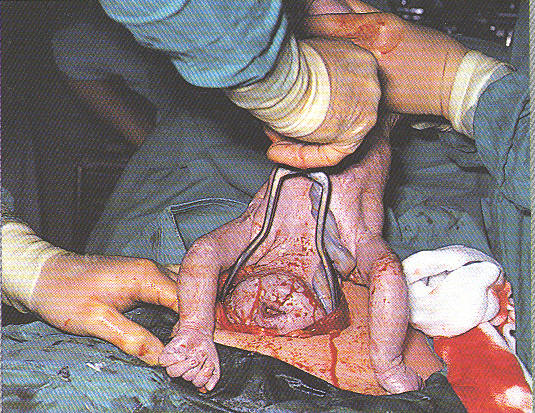
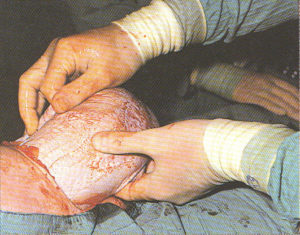
Use of obstetrical forceps to deliver the baby’s after-coming head.
Luckily there also are obstetricians who were willing to speak out honestly. One of those is Dr. Peter S. Bernstein, MD, MPH, Associate Professor of Clinical Obstetrics & Gynecology at the Albert Einstein College of Medicine.
Dr Bernstein took sharp exception to this romantic promotion of elective surgical delivery in an article published 9/16/02 Medscape — Ob/Gyn & Women’s Health, entitled “Elective Cesarean: An Acceptable Alternative to Vaginal Delivery?”
He also pointed out that current obstetrical management (which ignores physiological principles) is actually causing these problems and should be rectified:
“One argument often cited in favor of elective cesarean delivery is prevention of pelvic floor damage, which can occur with vaginal delivery. But these adverse side effects may be more the result of how current obstetrics manage the second stage of labor. Use of episiotomy and forceps has been demonstrated to be associated with … incontinence in numerous studies.
Perhaps also vaginal delivery in the dorsal lithotomy position [mother lying on her back] with encouragement from birth attendants to shorten the second stage with the Valsalva maneuver [prolonged breath-holding], as is commonly practiced in developed countries, contributes significantly to the problem.
Nonetheless, the prevention of pelvic floor injury by routine elective cesarean delivery is not an appropriate solution. Rather, more research into the management of the second stage of labor is clearly necessary. Moreover, cesarean delivery does not guarantee protection against pelvic floor dysfunction, given the reports of similar rates of urinary incontinence in nulliparous woman [no children] as in parous women…[those who have given birth]
As to the issue of Cesarean as a rescue operation to protect babies, Dr Berstein comments:
“To suggest that performing an elective cesarean delivery in a low-risk patient will avert intrapartum fetal injury is very misleading. These outcomes are rare, even in higher-risk women. Indeed, they are so rate in women without any identifiable risk factors that an absurd number of cesarean deliveries would need to be performed to avert even one of these poor outcomes. Thus, resorting to cesarean delivery would not be appropriate standard procedure.
The risks of Cesarean rise with each successive surgery as the operation becomes more technically difficult as a result of surgical adhesions.” [Elective Cesarean: An Acceptable Alternative to Vaginal Delivery? Peter Berstein, MD, MPH] (emphasis through added by editor)”
Lots of Collateral Damage
 Bottom-line is that childbearing women are two to four times more likely to die from the intra-operative, post-operative or downstream complications of Cesarean surgery than from normal vaginal birth.
Bottom-line is that childbearing women are two to four times more likely to die from the intra-operative, post-operative or downstream complications of Cesarean surgery than from normal vaginal birth.
More than a dozen operative and post-op complications for the mother are associated with Cesarean including maternal death, maternal brain damage, anesthetic accidents, drug reactions, infection, accidental surgical injury, hemorrhage, emergency hysterectomy, blood clots in the lungs, need to be admitted to ICU, need to be on life support, inability to breastfeed.
Unfortunately, these dangers don’t go away simply because the mother survived the surgery. Potentially-lethal complications and protracted difficulties extend into the postpartum period, post-cesarean, post-cesarean pregnancies and post-cesarean labors. Reproduction complications include secondary infertility, miscarriage, and tubal pregnancy.
 Delayed or downstream complications in future pregnancies include placental abruption, placenta previa, placenta percreta, uterine rupture, and maternal death or permanent neurological impairment.
Delayed or downstream complications in future pregnancies include placental abruption, placenta previa, placenta percreta, uterine rupture, and maternal death or permanent neurological impairment.
Risks to babies include accidental premature delivery, surgical injury during the CS, respiratory distress, increased rates of admission to NICU. Risk to babies in subsequent pregnancies include placenta abruption/stillbirth, death or permanent neurological disability (due to uterine rupture), lung disease and increased rates of both childhood and adult asthma.
The best documentation of these facts comes from Dr Harer’s contemporary colleagues. In an article entitled “Elective C-section Revisited” Dr. Elaine Waetjen (an obstetrician from UC Davis), takes sharp exception to Dr. Harer’s promotion of elective CS as protective of the pelvic floor. Her remarks were published in Ob.Gyn.News, August 1, 2002:
“The prophylactic use of elective cesarean section to prevent pelvic organ prolapse and urinary incontinence is gaining increased attention. Dr Benson Harer, Jr, past president of the American College of Obstetricians and Gynecologists, stated publicly last year that women should have the right to choose a cesarean delivery.
….why shouldn’t we offer prophylactic C-section to prevent this problem later in life?
The answer is that the evidence does not support this approach. Preventive strategies should cause no more harm than the disease or problem that they are trying to prevent. Ideally, they should incorporate some kind of screening to identify people at risk. They should be cost-effective and based on very good evidence of benefit. Elective C-section to preserve pelvic floor function fails on all three measures.
Cesarean surgery causes more maternal morbidity and mortality than vaginal birth. In the short term, C-Section doubles or triples the risk of maternal death, triples the risk for infection, hemorrhage and hysterectomy, increases the risk of serious blood clots 2 to 5 times and causes surgical injury in about 1% of operations.
In the long term, cesarean section increases the mother’s risk of a placenta previa, accreta or percreta, uterine rupture, surgical injury, spontaneous abortions and ectopic pregnancies while decreasing fecundity.”
…would have to do 23 C-sections to prevent one such surgery [for organ prolapse or incontinence) later in life. So instead of offering elective cesarean in an attempt to prevent future prolapse or incontinence, we should be examining what we can do in our management of vaginal deliveries to protect pelvic floor function”.
New mothers who were delivered by Cesarean experience an increased rate of serious postpartum depression, low self-esteem and breastfeeding failures and report post-operative pain lasting up to 6 months. Complications of post-cesarean reproduction include a higher rate of infertility, tubal pregnancies and miscarriage.” (Ob.Gyn.News ‘Elective C-Section Revisited’ Dr. L. Elaine Waetjen; August 1 2001 • Vol 36 • No 15)
More published comments by members of the obstetrical profession listing complications of Cesaren surgery:
“Mothers in post-cesarean pregnancies face a significant increase in placenta previa, placenta accreta and placenta percreta (types of abnormal growth of placenta into the wall of the uterus) as well as uterine rupture, emergency hysterectomy and the need for extensive blood transfusions..” (Ob.Gyn.News Vol 36, Aug 1, 02).
“The rate of emergency hysterectomy within 14 days of giving birth is 13 times higher for women delivered by Cesarean surgery.” (Obstet Gynecol. 2003 Jul;102 (1):141-5. Route of delivery as a risk factor for emergent peripartum hysterectomy)
“These delayed and down-stream complications elevate mortality in post-cesarean pregnancies for both mothers and babies — up to 10% for women who develop placenta percreta and about 1/2% for newborns. Elective Cesarean: An Acceptable Alternative to Vaginal Delivery? Peter Berstein, MD, MPH).
Babies in post-cesarean pregnancies suffer a higher rate of fetal demise and stillbirth (Ob.Gyn.News ‘C-Section Linked to Stillbirth in Next Pregnancy’ May 15 2003 • Vol 38 • No 10)
“Babies delivered by cesarean have a higher risk of lung disorders and operative lacerations.” ObGynNews, 6/15/01,
“Babies delivered by planned cesarean section are significantly more likely to require hospitalization for asthma during childhood than babies born vaginally” Asthma Associated With Planned Cesarean – ObGynNews; May 15 2003 • Vol 38 • N0 10
“Cesarean babies also suffer triple the rate of asthma as adults. [Cesarean Birth Associated with Adult Asthma — Ob.Gyn.News Jun 15, 2001, Vol 36, No 12]
Operative Deliveries and Postpartum Depression
Postpartum depression can occur after the most normal of pregnancies but is more common and more severe after the added stress of a Cesarean or other operative delivery and when a baby is premature or must be in the intensive care nursery after the birth. [Predictors, prodromes and incidence of postpartum depression; Obstet Gynaecol June 2001]
The self-esteem of first-time mothers improves and measures highest on psychological tests, for women who have normal vaginal births while showing a deterioration for mothers who delivered by Cesarean surgery. [Adverse psychological impact of operative obstetric interventions: a prospective longitudinal study Aust N Z J Psychiatry]
No VBAC Policy Results in Non-consensual, Medically Unnecessary Cesareans
It is impossible to leave the topic of Cesarean section without revisiting the issue of post-Cesarean pregnancies and “VBAC”. As noted earlier, the obstetrical profession has dramatically back-peddled on this issue from its original support in the early 1980s, followed by ACOG’s 1986 promotion of VBAC, to ACOG’s 1998 change of heart and draconian restrictions.
The final blow, the coup de gras, however was one particular study published in the NEJM that focused on the effect of inducing post-cesarean women with prostaglandins, Cytotec and Pitocin. In general it revealed a greatly increased risk of uterine rupture when these women were induced (up to 15 times higher).
But strangely enough, it was widely promoted in the media (Associated Press, NPR, etc) as establishing that Cesarean surgery was always the “safer” choice for the baby and we should return to the dictum of “once a Cesarean, always a Cesarean”. Since July of 2001, the number of VBACs has plummeted like a stone after and of course, the repeat CS is going up, up and away.
However, reinstating the policy of “once a Cesarean always a Cesarean” only trades the rare complications of spontaneous VBAC labor for increased maternal deaths from so-called ‘elective’ surgery or placenta percreta and equal number of neonatal deaths or disability from iatrogenic prematurity, and does so without truly informed consent.
Pushing the policy of automatic repeat CS assumes that death or damage resulting from a medically unnecessary surgical procedure (the over-treatment model) is morally superior to the more reasonable choice of planning a normal, spontaneous (i.e., not induced) labor.
Women now report that large areas of the country have no physician and/or hospital that will ‘permit’ a woman with a previous C-section to labor normally and give birth vaginally. The reasons cited by the medical profession are ‘safety’ but if you read the literature published by or for the obstetrical community, their spokespersons freely acknowledge that it isn’t the actual danger to mothers and babies that are fueling the elimination of VBAC but rather the malpractice risk to institutions and obstetricians.
According to a guest editorial in Ob.Gyn.News (“Informed Consent for Attempted VBAC” by Sinclitico, JD; April 1, 2005) by an attorney who specializes in malpractice law: “Some physicians prefer elective C-sections to VBAC because of the large monetary awards in medical malpractice lawsuits dealing with VBAC, such as a $30 million-dollar judgment in Philadelphia…”
He goes on to quote a large multi-center study that he calls “the first solid data” on the risks of VBAC, which showed that only 0.7% of approximately 18,000 VBAC labors resulted in neurological damage for the baby. Of that small group of 12 infants, only 7 were related to uterine rupture. He gives the absolute risk as 1 case per 2,000 women “attempting” VBAC at term.
Co-incidentally, this is exactly the same ratio of risk for neurological impairment or perinatal death that applies to all first time mothers. Risk-wise, having a VBAC is like having a ‘first’ birth, twice in a row. Previous CS mothers loose the advantage usually enjoyed by women having a second baby after a previous vaginal birth. In point of fact, the great majority of these women actually are having a ‘first’ vaginal birth, so this is a combination of natural risk plus their VBAC status.
Mr. Sinclitico goes on to say that: “Even though the risks of a bad outcome are small — and ongoing statistics support that – those statistics take flight when you’re in the witness chair. … While there were only 12 case of [permanent brain damage] in the recent multi-center study, if we assume that each of those cases went to trial and the plaintiffs won only 10% of the largest award in the Philadelphia case, that totals $36 million, plus untold millions of dollars spent defending those cases. … That’s why most obstetricians are voting to do cesarean sections instead of VBAC.”
Another example of how policy of disincentive for VBAC is influenced by factors other than the actual safety can be seen in ACOG’s very relaxed relationship to Pitocin induction. Identical dangers and physician requirements for Pitocin induction or augmentation are universally ignored by obstetricians and by ACOG.
The package insert by the pharmaceutical company (Parke-Davis) for Pitocin lists 11 complications or ‘adverse events’ associated with Pitocin administration for mothers, including anaphylactic reaction, brain hemorrhage, cardiac arrhythmias, pelvic hematomas, fatal blood clotting problems, uterine rupture and maternal death.
It also lists 7 complications for the unborn or newborn baby including cardiac arrhythmias, convulsions after birth, hemorrhages in the eyes, permanent brain damage and death. The precautions state that: “A physician qualified to manage any complications should be immediately available.”
However, this direct requirement, virtually identical in it’s wording and for identical reasons, is completely dismissed by ACOG, hospitals and malpractice carriers. Were the requirement that the physician be “immediately available” appropriately applied to labor induction, we would be see a move by the obstetrical profession for ‘natural’ labors instead of a 23% induction rate.
Clearly the consequences of this political situation means that the small risk to the physician of malpractice litigation is exchanged for the long list of risks and complications associated with “elective” repeat CS. And in all too many cases, insult is added to injury when these women, denied all other options (except unattended birth), are really forced into unwanted and medically unnecessary surgery. These so-called ‘elective’ surgeries are more truthfully best described as “unelected and non-consensual” cesareans.
Modern Tort Law and Voluntary Consent
While the medical system gives full lip service to fully informed consent, when the topic is obstetrical interventions, such as induction and especially Cesarean section, the consent process as used today in the obstetrical world does not actually comply with the legal principles of informed consent.
And should a woman be perceived as ‘non-compliant’ with obstetrical advice or even just wavering, wanting to go home and think about it longer or to get another medical opinion, enormous psychological pressure is brought to bear, up to and including threats of legal action. No outcome of that kind of power disparity can ever be considered to be voluntary and fully informed consent.
The concept of ‘informed consent’ may seem unduly complicated for a layperson but really is quite straightforward and it is ever so helpful to at least be familiar with the basic idea.
The legal theory of informed consent includes the following three aspects:
(1) An acknowledgement that physicians have a duty to obtain informed consent of patients before they perform potentially risky, complex, invasive, painful or experimental medical procedures
(2) That a mentally competent patient has the right to consent or refuse to consent to any recommended medical procedure
(3) That a patient has the right to sufficient information to make that consent meaningful
If a physician treats a patient without any consent, he or she may be liable for battery or an intentional ‘tort’. This applies not only to non-consensual treatment but also when a physician exceeds the scope of the patient’s consent, whether or not the treatment or procedure was properly performed.
If a physician obtains a patient’s consent to treatment but does so under duress or trickery, it does not count as truly voluntary or freely given informed consent. This makes the physician vulnerable to charges of battery. If the physician obtains a patient’s consent to treatment but fails to provide sufficient information to make a meaningful decision, the patient may bring legal action for negligence based on lack of informed consent.
Fully Informed Consent Means the Truth, the Whole Truth and Nothing But the Truth…
Generally speaking a physician must disclose all information which is ‘material to the patient’s decision of whether to proceed”, that is, “that information which the physician knows or should know and would be regarded as significant by a reasonable person in the patient’s position when deciding to accept or reject the recommended procedure.
This standard does not require a warning for every possible risk [i.e. remote or rare complication] and the physician is not required to give a ‘mini-course’ in medical science. However the patient must be given enough information in lay terms to make a knowledgeable decision regarding the recommended medical procedure.”
This includes the risks, complications, expected benefits of the proposed treatment (including likelihood of success) and any alternative to the procedure, including the alternative of no treatment and the relative risks and benefits of not having the procedure. [California Medical Association Document # 0415 – Informed Consent, Jan 2001]
Were we to impose the two clearest, most easily understood and most basic requirements — “information which the physician knows or should know” and “would be regarded as significant by a reasonable person in the patient’s position when deciding to accept or reject the recommended procedure” the only possible answer would be the truth as it is known to the obstetrical profession through textbooks, journals, trade papers (Ob.Gyn.News) and conferences.
To quote the editor of a well-respected obstetrical textbook (Davis) published in1966, “There can be no alibi for not knowing what is known.”
Doctors are formally educated and highly paid to know the scientific literature and be aware of the full spectrum of consequences associated with medical and surgical interventions. It is not unreasonable to expect their advice, both to the public and to individuals, to be objective.
All of this is in contrast to reality, as the obstetrical profession has gone to great lengths over the last century to convince all of us that physiological management is old-fashioned, inadequate and dangerous.
They purposefully dismantled the infrastructure for providing physiological management, claiming that care for normal childbirth, at least for the affluent, should consist of a constant stream of medical and surgical interventions provided by physician-surgeons in an acute care hospital setting.
When it comes to the astronomical expense of the interventionist model (particularly the ‘elective’ Cesarean), the sky’s the limit, because we are repeatedly assured that this extravagance is buying us better babies and saving the pelvic floor of their mothers.
“There can be no alibi for not knowing what is known,….” Foreword ~ Davis obstetrical textbook, 1966
Here is a brief list of just the headlines from contemporary editions of Ob.Gyn.News on the topic of elective or repeat Cesareans. They easily identify both what a ‘physician knows or should know’ and what would be considered significant by a reasonable person before giving or withholding permission to be induced, immobilized in bed, have medically unnecessary C-section performed, etc:
“Upright Positions Offer Most Room for Delivery” 02/01/02
“Reconsideration of ‘Purple Pushing’ Urged” 03/15/03
“Routine Coached Pushing May Be Harmful” 10/01/04
“Induction Linked to Doubling of Cesarean Rate in First-Time Mothers” 01/01/03
“Estimated Fetal Weight Not a Guide for Cesareans” 12/12/01
“Routine Episiotomy Offers Women No Benefits or Relief, long recovery, some harm” 06/01/05
“C-Section, Cervical Ripening Link Seen in Women previously delivered vaginally” 06/15/03
“C-Section to Prevent Cerebra Palsy: Results May Be a Wash” 04/15/02
“Double-Layer Cesarean Closure May Be Safer” 03/15/02
“C-Section Linked to Stillbirth in Next Pregnancy” 05/15/03
“Maternal Morbidity Rises Sharply with Repeat Cesareans” 03/15/05
“Prior C-Section Assoc. with Worse Outcomes – ICU Admit, postpartum infection” 03/01/05
“Study Shows Elective Cesarean Riskier than Vaginal Delivery” 05/01/04
“Asthma Associated with Planned Cesarean” 05/14/03
“Cesarean Birth Associated with Adult Asthma” 06/15/01
“Steep Rise Seen in “No [Medical] Risk Primary C-Sections” 01/01/05
“Offering C-Section ‘On Demand’ Can Be Ethical: ACOG” 12/01/03
“Cesarean Rate Portends Rise in Placenta Accreta” 03/01/01
“ …Placental Invasion on the Increase – hike in C-Section may be responsible” 01/15/03
“Placenta Previa, C-Section History Up Accreta Risk” 09/15/01
“Childbirth, Pregnancy Tied to PTSD, Expert Says” 01/15/03
The More Things Change, the More They Stay the Same
Despite extensive credible sources reporting on complications related to Cesarean-section, of which the above list is only a tiny fraction, the approximately 40,000 obstetricians practicing in the US that comprise the nationwide membership of ACOG, have continued to ‘drift’ towards the casual and ever-increasing use of Cesarean section.
In general, obstetricians believe that the decisions surrounding Cesarean surgery are rightfully those of the medical profession and not the childbearing woman. However, if the mother-to-be asks for a C-section, obstetricians are usually very happy to oblige them, as scheduled daytime surgery is so much better for doctors. However, we must note here that if normal hospital births were attended by hospital-employed midwives, they would only be called in the middle of the night if there was a problem for one of the labor patients or emergency cesarean surgery was needed.
The headline of an Ob.Gyn.News (12/1/2002 Vol 37, No23) report reads “Experts Say Guidelines Out of Step with Trend Toward Elective C-Section”. It goes on to states that “Practice guidelines discouraging scheduled elective Cesarean section are out of step with increasingly liberal attitudes toward the procedure on the part of rank-and-file ob.gyns….”
It is interesting to note that performing medically unnecessary C-sections are characterized as “liberal” and that it is the attitudes of “rank-and-file ob.gyns” that seem to count the most. The article argues for the right of women to have childbirth by Cesarean section the same way Burger King plays to our right to “have it your way”. One OB is quoted as saying: “Women can choose to have a breast implant, so why can’t they choose to have a C-section if they don’t want to go through the process of labor? It’s their body.”
 Halloween, 2003 ~ Unnecessary Surgery Declared “Ethical” by ACOG
Halloween, 2003 ~ Unnecessary Surgery Declared “Ethical” by ACOG

Given the long historical “trend” towards surgical birth that has been building since the late 1800s, it is no surprise that 90 years after Dr. DeLee declared normal childbirth to be by nature pathological and dangerous to both mothers and babies, 18 years after Drs. Feldman and Friedman concluded that we could save additional babies if we would only we aced to the “excess maternal mortality” associated with 100% prophylactic Cesarean, 3 years after Dr Ben Harer advised women to demand a C-section to protect and preserve their perineums, that ACOG’s Ethics Committee ruled it was “ethical” in 2003 for physicians to perform Cesarean for non-medical reasons including “patient choice”. Their rationale was based on the imagined “lack of data on the risks and benefits of Cesarean vs. vaginal delivery”.
****************************************
Link to Chapter 10
