Birth images: Part 2 ~ The Disappearing Mother: the active role of women giving birth is replaced by a passive & subservient role in which physicians are credited with “delivering” babies
The historic evolution of birth practices as revealed in images of normal childbirth from approximately 3,000 BCE to modern day
Part 2: The Disappearing Mother ~ a four-hundred-year journey into an obstetrical Dark Ages
in the middle of the 17th century, the medical profession decided that normal childbirth needed to be modernized by having obstetrically-trained physicians replace midwives as the customary birth attendant, and the non-interventive support for normal biology be eclipsed by medical and surgical interventions. In Europe, thousands of years of woman-centered childbirth began to be slowly but systematically replaced by physicians who increasingly managed labor as a medical condition.
This historical period of time (1650 to 1800 CE) followed the Renaissance and is known as the “Age of Enlightenment”Educated members of the aristocracy, many of whom were physiciansOver the course of several centuries childbearing women were limited to a role that was increasingly passive and subservient. Instead of healthy women as active agents in their own normal labors, attended by midwives and giving birth under their own power, spontaneous vaginal birth was replaced by a medical/surgical procedure ‘performed’ by medical doctors that came to be called “the delivery“. This ‘new way’ eventually became the unquestioned ‘norm’ in most developed countries in the modern-day world.
( influenced by the scientific revolutions of the previous century, believed in shedding the light of science and reason on the world in order to question traditional ideas and ways of doing things.
were convinced that replacing old superstitions with science and reason would automatically improved the lives of human beings and human society.
When new mothers are active agents in their labors and births, giving birth is something they can take personal credit for having accomplished. This is a critical part of the normal developmental process that turns a woman into a capable, confident new mother. Her childbearing experiences reflect inner qualities of perseverance, endurance, adaptability, physical strength beyond what she thought she could do or what she could tolerate. All this generates confidence in the woman’s ability to fulfill her role as a new mother. A recent popular woman’s magazine quoted a Hollywood star who’d had a normal and unmedicated birth as saying that it was really hard, but afterward she realized that tolerating many hours of labor and pushing her baby out by her own efforts left her feeling that “I can do anything”.
Whenever a doctor (and not the mother) is credited with “delivering the baby”, the absence of this natural and necessary development stage makes it much more difficult for many (if not most) women to take on this new motherhood role.
Birth Image Synopsis ~ Part 2: As an active agent in normal childbirth, the upright and active childbearing woman gradually disappears as external forces restricted her actions, level of activity and posture assumed while giving birth.
This begins simply and benignly enough with sitting still on a simple birth seat or stool (early Middle Ages 1500s), and then furniture is developed that tipped the mother-to-be back so she progressively went from merely reclined again the back of lounge chair to lying fully prone with legs bent and knees pulled back and finally laying prone with her feet in obstetric stirrups. By the early 1900s in the US, normal childbirth was conducted as a sterile surgical procedure that included the routine use of episiotomy and forceps and was ‘performed on a mother rendered unconscious by general anesthesia.
The photographs and graphics in Part One clearly identified the central role of the mother in childbirth — it can only be said that she gave birth — that is, she was active, upright, and with the emotional and physical support of other women and family members, the woman labored and using her own efforts and physical strength, pushed her baby out. In some cases, she was helped in her efforts by physical objects, for example, steadying herself by leaning against a tree, pulling on a rope, squatting on two bricks (in Exodus these are usually translated as “discs”or sitting birth stool. Whatever type of help might have been found useful, the mother GAVE BIRTH. Her baby was NOT ‘delivered’ by efforts or activities of another person.
Over the last four centuries, normal childbirth has become increasingly disconnected from the biology, psychology and sociology of healthy women as competent, capable adults. Laboring women as competent persons in charge of their experience and their own bodies, and the women friends and family that helped them (midwives and others) were either gradually or suddenly eliminated over these four centuries. By the early 1900s, they were replaced in the US by hosptial staff, physician-obstetricians and the use of narcotics, amnesic drugs and anesthesia.
The perspective of medical doctors was dramatically and drastically different than that of childbirth as seen through the eyes of the childbearing woman or her midwife. As a medical or surgical procedure, the intellectual focus of physicians was on the role they played as medically providers instructions on how to labor and as the person called on to ‘perform’
The vantage point of men with medical training was dramatically and drastically different than that of childbirth as seen through the eyes and repeated experience of childbearing women and the midwives who attended normal births. In the historic model, the childbearing woman is the most important person in the room and the center of everyone’s attention.
However, when childbirth is re-contextualized as a medical or surgical procedure ‘performed’ by a physician, the intellectual focus quite naturally become the role that doctors saw themselves playing as the ‘smartest’ person in the room and the one responsible for the outcome and the one that would be blamed if there was a serious problem. Under these circumstances, it was the physician-obstetrician role to instruct the mother, and any helpers present, on the proper way to labor. As a medical birth attendant, it was the physician (instead of the mother) who was responsible for seeing that baby was born by whatever means necessary.
During this process were forcibly disconnected from our inner power and became “patients” in an institutionalized system run by other for purposes that had little or nothing to do with our personal well-being as individuals with social, emotional and practical needs, or those of our unborn or newborn babies.
Childbearing women are inherently the center of the biological process of laboring and giving birth. Over the last 4 centuries, the role assigned to pregnant woman by society went from being an active and indispensable agent, who is naturally triggered by the physiology of labor to making right use of gravity giving birth in upright position, able to move about on her own two feet, helped by other women and midwives, to laying on one’s back in the passive role of a ‘patient’, isolated from other women helpers, and being “being delivered” by doctors
Women as an active agents in their own normal labors and birth have for 5,000 or more years naturally made ‘right use of gravity’ by laboring in upright position, able to move about on her own two feet, helped by other women and midwives to give birth as an unencumbered person able to choose the place, the person and the position that best suited her and the actual events of the birth.
In the last several centuries, social and political pressures conspired to remove to childbearing women from their own births, insisting that they lay on their back in the passive role of a ‘patient’, isolated from other women helpers, and being “delivered” by doctors
The Fall ~
Over the last few centuries, the active role of the mother — on her own feet and in charge of her own body — devolves as laboring women became increasingly encumbered with physical limitations and a role that saw women as physically inadequate and mentally unstable, this in need of being rescued by outside forces.
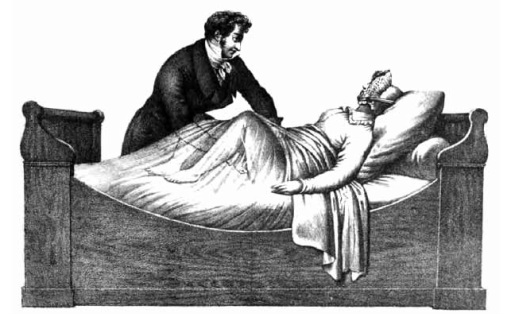
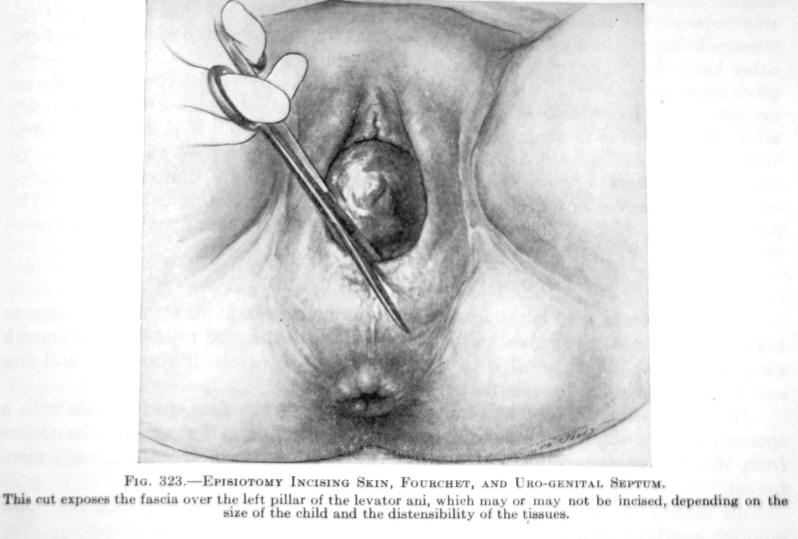
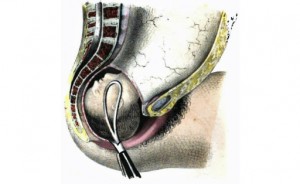
When male physicians began to attend normal childbirth as ‘man-midwives’, the mother became a patient confined to bed and give birth laying on their back, in the classic, stranded-beetle position. Deprived of the right use of gravity and normal movement, the normal pushing stage was prolonged. Doctors used a variety of methods to hurry things along, including medical interventions (such as the balloon used to dilate the cervix pictured below) and surgical interventions such as a series of cuts an inadequately dialated cervix, then doing an episiotomy and using forceps to deliver the baby.
1700 to 1899
 Physician performing vaginal exam |
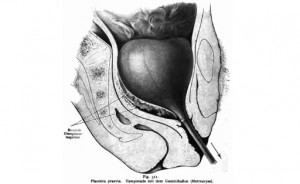 Balloon inserted thru cervix into uterus and then inflated |
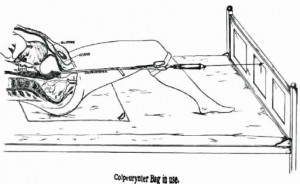 The neck of inflated balloon was tied off with a long cord and other end tied to the foot of bed to exert downward traction |
| Cut-away diagram |
 |
 |
 |
  |
 |
 |
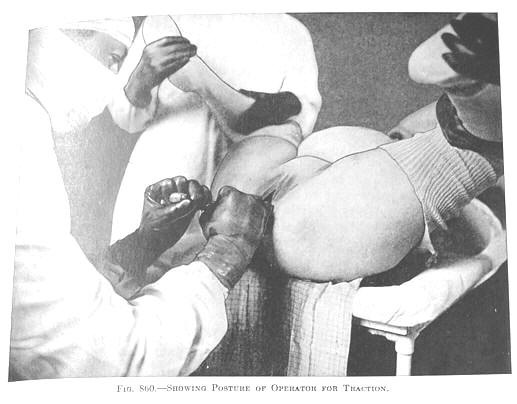
After being moved by stretcher from the labor ward to the OR-type delivery room, her hands would be put in leather wrist restraints, lest she touch something and contaminate the doctor’s sterile field. Her legs would be strapped into stirrups, her crotch scrubbed with an antiseptic soap, and her body covered up under mounds of sterile sheets. When the doctor arrived, the mother-to-be was rendered unconscious under general anesthesia. The physician-obstetrician then deftly performed a ‘baby-ectomyw’ using ‘low’ forceps. In these circumstances, women no longer gave birth — doctors ‘performed’ the surgical procedure of vaginal ‘delivery’ while the mother was unconscious.
 Insertion of forceps in anesthetized mother |
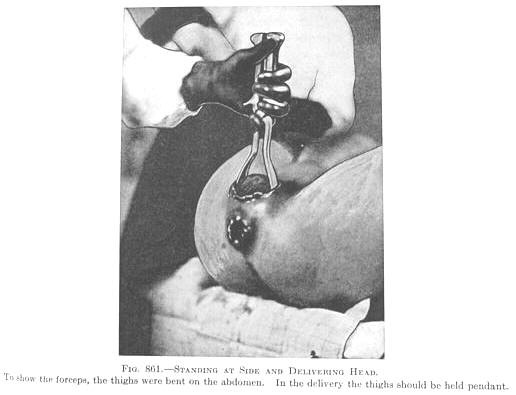 In order to follow the natural 60-degree curve of the pelvis, the obstetrician has to pull up, towards the ceiling to delivery the baby’s head |
 |
In many (but not all) parts of the county, spinal and pudental blocks (a form of local anesthesia), and eventually epidurals during labor and birth replaced general anesthesia by the 1960, 70s and 80s. Women were no longer unconscious (although the labor patient in the picture looks like so be happier if she were), but labor and birth were still heavily medicalized and women moved to the delivery room for the birth, where they continued to disappear under a mountain of sterile drapes.
By the 1900s and early 2000s, upgraded obstetrical unites had replaced the routine use of the delivery room with LDRP beds that can be taken apart and turned into a gynecology-type OR table. Also the mandatory use of OR-garp had been relaxed and surgical masks were no longer mandatory. However women under epidural are still unable get out of bed or move about very well, so they also lay no their backs, still pushed the babies out over empty space to be ‘caught’ by the masked stranger standing at the end of the LDRP be/deliver table.
For women who were not anesthetized, the head of their bed was sometimes gatched up so they were no longer flat on their back when the (now) unmasked stranger caught their baby.
A few lucky women managed to use a squatting bar, or “allowed” to give birth lying on their side. This was an improvement but note — the labor woman’s feet still never get to touch the ground, she is never a physically free agent, to hold up her own body, and move about as will.
This very depressing story culminates in the late 20th and early 21st century with the laboring woman strapped to an OR table in the classic “crucifix” position and the masked and hooded OR staff pulling her baby out of a Cesarean surgery incision.
|
Post C-S uterus is ‘extroverted’ — pulled up and out to lay externally on the mother’s abdomen. This makes suturing easier. Sutured incision is front bottom of photo, metal bladder retracted at bottom center and surgeon’s gloved fingers middle far right |
