Stand-alone Addendum for mfry educators,
students journalists and patients’ rights
and product liability attorneys
Easy Shortcut to share –> http://tinyurl.com/y3evnwwa word count 4100
 A brief history of monitoring the unborn baby: Intermittent Auscultation ~ its verbs, nouns, and physician-inventors.
A brief history of monitoring the unborn baby: Intermittent Auscultation ~ its verbs, nouns, and physician-inventors.

For information about fetal monitoring as an electronic device (i.e., noun instead of an action verb), please read Part 1, 2 & 3 of the Rethinking-the -Role-of-EFM-Report-2019_#1 {easy-to-share Tiny URL}
The False Association btw routine use of
continuous electronic fetal monitoring (c-EFM) to
prevent Cerebral Palsy & Protect OBs from Lawsuits
 Editor’s Note: The first section, which is on the 400-year history of medical professionals listening to the unborn baby’s heart tones, and monitoring FHTs during labor, is a slightly more detailed version of the information given in the last part of the previous post (link to Part 1 immediately above):
Editor’s Note: The first section, which is on the 400-year history of medical professionals listening to the unborn baby’s heart tones, and monitoring FHTs during labor, is a slightly more detailed version of the information given in the last part of the previous post (link to Part 1 immediately above):
Even if you read that previous post, reviewing this more detailed information is good preparation for the section on the historical form of Intermittent Auscultation — what it is, it’s history, why it should be the modern standard of care for healthy women with normal term pregnancies, and 2nd generation auscultation techniques that yield the best and most reliable results.
As members of a compassionate society, but one that nonetheless does NOT have unlimited funds, our goals is to inform the public about the ineffectiveness, unproductive expense, and potentially-fatal complications of continuous electronic monitoring when it is inappropriately used as the standard for healthy women.
At the same time, we must make the public aware that there is a safe, satisfactory and cost-effective ‘alternative‘ — Intermittent Auscultation — that provides the same four categories of information on status the unborn baby and IA includes the continuous presence of a midwife or L&D nurse through out labor. This mother-focused care provides eyes-on, ears-on and hands-on support and encouragement to the laboring woman, this reducing the likelihood that drugs will be need to to speed up labor or for pain relief.
 In addition, the continuous presence of a nurse or midwife is so more cost-effective than the $400 per hour charge billed to insurance companies or the federal Medicaid program for c-EFM. The average salary of nurses and midwives is under $50 an hour, or a saving of $350 an hour over the cost of c-EFM. The continuous presence of a trained labor and birth attendant also reduces the incidence of Cesarean or other operative delivery and all the expensive complications and increased maternal morbidly and mortality associates with Cesarean surgery.
In addition, the continuous presence of a nurse or midwife is so more cost-effective than the $400 per hour charge billed to insurance companies or the federal Medicaid program for c-EFM. The average salary of nurses and midwives is under $50 an hour, or a saving of $350 an hour over the cost of c-EFM. The continuous presence of a trained labor and birth attendant also reduces the incidence of Cesarean or other operative delivery and all the expensive complications and increased maternal morbidly and mortality associates with Cesarean surgery.
Auscultation ~ Effective fetal monitoring without exposing the laboring woman to higher rate of Cesarean surgery and its complications
 We need to dramatically change the thinking of the majority of Americans in two important areas.
We need to dramatically change the thinking of the majority of Americans in two important areas.
The first is the extremely inaccurate idea that the US has the very best healthcare in the entire world. Actually the American healthcare system ranks near the bottom of developed countries.
Secondly, most Americans assume that maternity care in America is likewise the best in the world. Unfortunately, that’s also not true. Compared to other high-income industrialized countries, and in spite of spending two or three times money more on maternity care, the US has one of the highest maternal and neonatal mortality rates of all the developed countries. America is one of only eight countries disgraced by a high and increasing maternal mortality rate.
However, the majority of American are unaware of these grim facts. Instead they believe our obstetrical system is as good as it gets and from this perspective, electronic fetal monitoring seen as the crown jewel of the obstetrical profession. EFM is seen as the marvelous machine that allows OB doctors, assisted by L&D nurses, to monitor and record every beat of the unborn baby’s heart during labor and at the first hint of a possible problem, to rush the laboring woman off to the operating room and ‘rescue’ the baby by performing an emergency CS.
These people see continuous EFM as one of the very best life-saving technologies ever invented, able to save the lives of babies that otherwise would not have lived or would be born with terrible problems like cerebral palsy and permanent mental and physical handicaps.
Seen from this perspective, it’s logical to believe that any doctor who doesn’t use continuous EFM is guilty of medical malpractice and any childbearing women who refused to let her unborn baby be electronically-monitored during the labor is guilty intra-uterine child-abuse.
The suggestion that (a) routine continuous EFM of heathy women during labor actually makes both mother and baby less safe and (b) recommending instead that the nurse or midwife use a hand-held Doppler to monitor the baby’s health status during labor would be seen by many as a crazy, upside-down idea. Nonetheless, second generation auscultation regularly listens to and records the rate and rhythm of the unborn baby’s heart rate, while also tracking the same four categories of data as EFM, is the safer and better choice for healthy women with normal term pregnancies than routine EFM.
According to forty-four years of studies that compared continuous EFM to the ‘control’ group, auscultation was consistently found to be as effective as EFM, while having a statistically-significant reduction in the cesarean section rate. One of the very first clinical trials of EFM reported 6% CS rate with auscultation compared to 16% Cesarean rate associated with EFF.
Action verbs of auscultation vs. the nouns that describe an electronic devise
We are asking the public to re-define the idea of “continuous” intrapartum “monitoring” as something provided by an ineffective machine that is extremely expensive (both in dollars and personal cost), and instead to systemize the continuous presence of a person who is professionally trained to provide intrapartum care that includes the use of IA as the standard of care for healthy women with normal term pregnancies.
This labor and birth attendant will monitor (as an active verb!) fetal well-being via intermittent auscultation (IA) during active labor every 15 to 30 minutes. This consists of using a pocket-sized fetal Doppler and watch or clock with a quartz movement (second-hand stops briefly with each tick) to gather information on the very same 4 markers of fetal well-being as is collected by EFM and used by doctors, midwives and nurse to determine the well-being of the fetus and to take action if it indicates a possible problem.
These are a:
- Normal baseline
- Normal variability
- Presence of normal accelerations
- Absence of pathological decelerations

This professionally-trained labor and birth attendant is able to continually observe and provide ears-on, hands-on support, encourage and assist the laboring mother, which greatly reduces the number of unplanned CS that result from iatrogenic (care-provider-related) or nosocomial (hospital-related) factors.
So expensive, continuous machine monitoring (EFM) is not good for healthy laboring women, while the continuous presence of a trained professional using the safer and more cost-effective techniques of IA to monitors fetal well-being is good.
 The first person to report hearing the sound of an unborn baby’s heartbeat was a 17th century physician by the name of Dr. Marsac.
The first person to report hearing the sound of an unborn baby’s heartbeat was a 17th century physician by the name of Dr. Marsac.
A contemporary of his, a Dr. Killian, was the first to ponder the possibility that the rate and rhythm of the fetal heart might be an indicator of how well the fetus was (or wasn’t) tolerating the process of childbirth.
Professor of Obstetrics, Dr. Jacques Alexandre Kergaradec, L’Academie de Medicine, Paris, Queen’s University of Belfast ~ early 1800s
However, this possibility went unnoticed for two more centuries, until 1818, when doctors Mayor and Kergaradec described a method of auscultating fetal heart sounds by placing one’s ear on or very near the maternal abdomen. Dr. Kergaradec also suggested that fetal heart sounds could be used to determine fetal viability and proof of life in the months before ‘quickening’, that is, before the mother could feel the baby kick.
In 1833, an English physician, Dr. Evory Kennedy, published guidelines for fetal distress and also recommend auscultation of the fetal heart rate to monitor the well-being of the fetus during labor and birth.

A simple tool for counting the fetal heart rate
However, the big leap forward came in 1893, when Dr. Von Winkel established criteria for fetal distress. After listening to the hearts of many babies during many labor, he realized that the FHR of an unborn baby in trouble would often (but not always) become abnormal, and beat much faster or much slower, or become extremely erratic. Some of these babies died before the birth, other were born profoundly depressed and often died later.
With this understanding, Dr Von Winkel identified the signs of fetal distress, which included abnormal fetal heart rates (FHR):
- tachycardia (a over 160 bpm);
- bradycardia (under 100 bpm),
- irregular heart rate, passage of meconium,
- abnormal fetal movement (i.e. agonal spasms of a dying baby).
By the turn of the 20th century, maternal fever was recognized as a cause of fetal tachycardia; head compression and cord compression were also known causes of bradycardia, and hyper-stimulated uterine activity associated with an abnormal FHR patterns and asphyxia.
When these abnormal heart rates were discovered very late in the labor, doctors could sometimes perform a forceps delivery to rescue the baby. By the late 19th century, the development of general anesthesia, germ theory of infectious disease (resulting the principles of asepsis and sterile surgical techniques) made Cesarean surgery safe enough to use during labor to rescue babies with extremely abnormal heart rates.
 By the early 20th century — 50 years before fetal heart monitoring was electronically automated by a computerized machine — doctors, midwives and nurses were using a special stethoscope called a Pinard Horn to regularly listen to the heartbeat of the fetus during labor. Pinard fetal stethoscope was developed in the 1880s and remained in use until the 1950s and is still used by some midwives, particularly in developing countries.
By the early 20th century — 50 years before fetal heart monitoring was electronically automated by a computerized machine — doctors, midwives and nurses were using a special stethoscope called a Pinard Horn to regularly listen to the heartbeat of the fetus during labor. Pinard fetal stethoscope was developed in the 1880s and remained in use until the 1950s and is still used by some midwives, particularly in developing countries.
Helpful as this information was, there were still a few babies with apparently “normal” FHR that were born with unexpected and unexplained problems that prevented the baby from breathing on its own. This usually resulted in death or severe handicaps.
As noted above, birth attendants and nurses were ‘monitoring’ these babies, but they paid little or no attention to the rhythm of the fetal heart or other elements now known to be equally, if not even more important: Variability, the presence of reassuring accelerations, absence of pathological decelerations, and noting the depth, timing, and duration of any decelerations that were detected.
 Then in 1922, Dr. Joseph De Lee, the famous obstetrician that founded the Chicago Lying-in Hospital and Chicago Maternity Center advanced the ability of birth attendants to prevent stillbirths. He and his colleague, Dr. David Hills, invented a hands-free fetal stethoscope for listening to fetal heart tones. This device became known as the DeLee-Hills Fetoscope.
Then in 1922, Dr. Joseph De Lee, the famous obstetrician that founded the Chicago Lying-in Hospital and Chicago Maternity Center advanced the ability of birth attendants to prevent stillbirths. He and his colleague, Dr. David Hills, invented a hands-free fetal stethoscope for listening to fetal heart tones. This device became known as the DeLee-Hills Fetoscope.
Then Dr. DeLee went on to develop the process and protocols for the intermittent auscultation (IA) of the fetal heart rate during labor, which included the 1893 description of fetal distress by Dr. Von Winckel. Using his new fetoscope, the FHR was to be auscultated every 30 minutes during first stage of labor, every three or five minutes during second stage, and continuously if signs of fetal distress were seen as an indication for forceps delivery.
 In 1924, 4th edition of Dr. DeLee’s obstetrical textbook Principles and Practice of Obstetrics includes a wonderful graphic that displays a fetal heart rate auscultated and charted in 5-second increments during a minute-long contraction.
In 1924, 4th edition of Dr. DeLee’s obstetrical textbook Principles and Practice of Obstetrics includes a wonderful graphic that displays a fetal heart rate auscultated and charted in 5-second increments during a minute-long contraction.
It shows a normal baseline rate of 132 bpm at the beginning of the contraction (ranging from 120 to 144 bpm when computed in 5-second samplings) during the first 20 seconds.
 As pressure on the fetal head builds up, there is a mild head compression decel, and we can see the FHR go down from 144 to 108 bpm over a span of 20 second during the middle of the contraction.
As pressure on the fetal head builds up, there is a mild head compression decel, and we can see the FHR go down from 144 to 108 bpm over a span of 20 second during the middle of the contraction.
As the contraction wanes and the uterus relaxes during the last 20 seconds, the unborn baby’s heart rate speeds back up to its pre-contraction normal baseline of 132.
Copy of a page in Dr. Joseph DeLee’s 1924 obstetrical text book
entitled “The Principles and Practice of Obstetrics”
![]()
If you read Dr. DeLee’s comments below the graph, he refers to a pattern of decelerations during the pushing stage that we now know to be head compression decels — the result of triggering the mammalian diving reflex that has been extensively documented in whales.
Dr Joseph DeLee on TIME magazine Cover in 1936
Dr. DeLee somewhat anticipated this explanation by referring to the abnormally slow heart rate of men working deep under water in a “caisson” (a big metal contraption used during the underwater building of bridges and similar construction projects).
DeLee’s work is the theoretical precursor to both IA and EFM, as it is the first instance of dealing with variations in the FHR during the period of auscultation by using a timepiece with a second hand to count fetal heart beats in 5-second samplings. Prior to this, the only information on fetal heart activity that was gathered was the sum total of beats over a 60-second period and recorded as a baseline rate.
When is a minute not a minute? ~ Ending a bad habit by the medical, nursing and midwifery professions:
As unfortunate and inadequate as it was to ONLY gather baseline information on fetal well-being, even more problematic is a long-time protocol for taking pulses and fetal heart rates. Both are stated in the universal language of beats per minute (bpm), but medical and nursing students are both taught that the proper way to take pulse and fetal heart rates is to palpate or lisent for only 15 seconds and then multiplied that number by 4 and state it the rate-per-minute, as if the care provider had listened or palpated for one whole minute.
In fact, this makes lay people think something that is not true and it deprived the practitioner of critically useful information. This in turn risks the well-being of the baby, as the baseline rate by itself is only a small part of the picture. Depending on what is happening with the baby, the beats-per-minute count may not change dramatically until the baby is just a few minutes away from dying.
A Brief Aside: It’s crazy (as well as bad policy) for doctors, nurses, midwives and other healthcare professionals to be thinking in terms of shaving seconds off the time they spend in the presence of their patients. What bedevils the provision of medical services in the US is the constant attempt to spend less time with the patient and more time having one’s assistants and employees doing minor and impersonal activities such as taking temperatures, drawing blood, etc.
As a result, doctors miss so much information that would come directly and easily from listening to their patients, getting to know more about them, taking time to assess them them from the standpoint of eyes-on, ears-open, hands-on care.
I hope midwives everywhere realize that it takes a full minute to gather the data that will be charted as the fetal heart rate per minute. This is a particular issue when using Dopplers that flash out a beats per minute number after only a few seconds. The point here is the same as the 15-second palpation of pulses and multiply by 4, except EFMs and hand-held Doppler calculate on a 2-second cycle.
Functionally, this is a throwback to a hundred years ago, when doctors and nurses first began to monitor the fetus during labor, but only listened to FHTs for a few seconds, and then wrote down a beats per minute rate (or made decisions on that number) but without having assessed for variability, accelerations or decels. It’s not IA unless the midwife is accesses all 4 data point each time she auscultates.
The only exception that I have found is the last few minutes of second state, just before the birth when so much is happening at the very same time that is hard to hear FHTs because the baby is so low in the pelvis. Then just when you start counting the FHR, the mother starts pushing again and moves away.
In those cases, if I get 5 or 10 seconds of a reasonably normal baseline, I consider that to be adequately reassuring that the baby is not in immediate distress and that’s as good as it get under such circumstances.
Of course, I keep trying, but often the baby is born before I get to hear a whole minute of its fetal heart rate. In those case, I immediate put my hand on the cord to palpate the neonate’s heart rate and be sure it’s over 100 and regular.

Returning to out topic of fetal monitoring
Dr. DeLee recognized a second-level source of valuable information that could be gathered by paying attention to the FHR changes that occurred (or failed to occur) within the one- or two-minute period that the FHR was routinely monitored by the L&D nurse, doctor or midwife. The more sophisticated 4-part criteria protocols for IA allowed care providers to intervention early and in most instances, prevent permanent damage.
The theoretical basis developed by Dr. DeLee and its 5-second sampling protocol, which yielded much a more useful picture of fetal wellbeing. This critical aspect of IA was not widely acknowledged or integrated into standard obstetrical practice until the development of electronic fetal monitoring equipment in the late 1950s and 60s.
Auscultation ~ An alternative method of fetal monitoring proven be as effective as continuous c-EFM
Counting the unborn baby’s pulse (i.e. heart rate and rhythm)
The simplest example of IA is to compare it to counting the unborn baby’s pulse over the span of one minute and using the second hand of a clock or wristwatch to calculate the beats-per-minute (baseline) and the three other well-established attributes of fetal wellbeing: normal variability; presence of reassuring accelerations; absence of pathological decelerations.
All over the world and for many hundreds of years, doctors, nurses, and midwives have regularly collected a similar set of facts from infants, children and adults by physically palpating their pulse, counting the beats for 15 seconds and then multiplying by 4 to get a 1-minute rate (for example, 21 beats in 15 seconds is a heart rate of 84). When doing this, the care provider would also note whether the rate was regular or irregular.
If the rate is irregular, or the person/patient is being evaluated for cardiac disease, the medical professional would palpate and count for one or more full minutes in order to detect the presence or absence of irregularities and whether there was any discernible pattern noted in the abnormal pulse.
These same medical professions would be thunder-struct if told that the only way to take a person’s pulse was to purchase an electronic machine that cost many thousands of dollars, was the size of a large suitcase and required access to electricity to work. In terms of the ‘wrong use’ of medicalization, this is akin to having to catheterize someone every time a urine specimen is needed. This would be particularly bad news for those of us who made house calls and for EMTs.
Luckily for them and for midwives and the families who choose low-tech care in their own home or a free-standing community birth center, we don’t need a $15,000 electronic maternal monitor to check the mother’s pulse, and we don’t need a $15,000 electronic fetal to take the baby’s pulse.
 The Nuts and Bolts of IA – what you need, how to do it, how to chart it
The Nuts and Bolts of IA – what you need, how to do it, how to chart it
However, there is no way to hold the baby’s wrist before it’s born, so either a special fetal stethoscope or electronic Doppler is used to hear the heart rate.
To count the heart rate, a battery-operated timepiece with a quartz movement is used to count the heart beats in each of the 12 or more samplings.
The reason for choosing a watch or clock with quartz movement is that its second hand has a tick–tick motion that moves once per second, while mechanical watches have a smooth, sweeping seconds motion. This momentary stop as each second is ticked off is very helpful when auscultating FHR in 5-second units.
The video below demonstrates how a quartz movement works, with the red second hand darting forward and the rest for a second with each tick of the clock.
There is ambient sound in this video, but you can’t hear the tick of the clock unless you are very close, and it’s not the sound of ticking that is uses in intermittent auscultation.
The contemporary practice of IA, most practitioners use a relatively inexpensive hand-held Doppler ($300-$600 vs. $10,000 to $15,000), which amplifies the sound and has a speaker so everyone in the room can hear the baby’s heart rate. This also makes it easier for mothers, as they don’t have to lay down and try to stay still during a contraction while the midwife listens and the birth attendant can hear and count fetal heart tone while the mother is standing up (including in the shower or while sitting on the toilet).
The protocol for IA is to listen to the unborn babies of mothers with low risk pregnancies on a schedule of:
- every hour in latent (very early) labor
- every 30 minutes in active (progressive) labor
- every 15 minutes in the first part of pushing stage
- after every 3rd contraction (or more frequently if needed) as the baby is being pushed down and out of the vagina (perineal stage) and being born.
As noted above, the purpose of fetal monitoring (verb or noun) during labor is to either document the unborn baby’s condition as well-oxygenated and neurologically intact or detect that, for whatever the reason, the fetus requires immediate interventions.
The 5-minute video below provides the sound of the FHTs and a Quartz clock that allows the reader to play around with IA skills. This was recorded during a normal prenatal exam at 34 weeks gestation. You can hear a normal baseline, variability, accelerations and no decel. Since this video made, the mother had a normal spontaneous labor and gave birth to a healthy baby boy.
It begins with my explanation to the mother of why I first palpate the position of her baby before listening to fetal heart tones, and how IA helps midwives know if our assessment of fetal position is correct. If her baby is currently in the position that I think it is (LOT, LOP, ROT or ROP, the heart sound should be best heard in spot on her abdomen that I specified.
The specific criteria that IA depends on is gathered by L&D nurses and midwives by listening for an entire minute or longer during which they count the fetal heart rate in five-second sampling over the course of a minute. This equates to twelve 5-second units or ‘samplings’ per minute. Note: one minute is the shortest length of time needed to be relatively certain there are no FHR irregularities, but when listening for accelerations, it’s sometimes necessary to listen for 2, 3, 4 or even 5 minutes
** For example, the normal baseline range for a fetus at term is between 110 and 150 bpm, with 120, 132, and 144 bpm being the most typical normal baselines during 1st stage labor. FH baselines () that are over 150 for 10 minutes or more are considered to be a mild stage of tachycardia.
When using 5-second sampling over one full minute or longer, what is counted per 5-seconds is generally a combination of 10s, 11s, 12s, 13s and occasionally a 14.
So a …
- normal baseline rate of 144
- normal variability
- one acceleration of 15 seconds {**}
- no pathological decelerations
…. would generate a sequence of numbers such as: 12, 12, 11, 12, 13, 12, {**13, 14, 13}, 11, 10, 11, 12, 12. ** The {13, 14 13} is an acceleration that momentarily elevated the baseline (if maintained) to 156, 168, 156 and then a return to the baseline of 144.
 A preponderance of 12s for 5-second units indicate a normal baseline of 144 (12 X 12 =144), just as a preponderance of 10s is 120, 11s is 132, 13s is 156, and 14s would be 168.
A preponderance of 12s for 5-second units indicate a normal baseline of 144 (12 X 12 =144), just as a preponderance of 10s is 120, 11s is 132, 13s is 156, and 14s would be 168.
That the slightly changing beat-to-beat rhythm is ‘varied’ documents the normal attribute of ‘variability‘, while a consecutive and elevated set of 13s (a cluster of 3 or more) indicates the presence of ‘reassuring accelerations’. Last but certainly not least, there were NO instances of 5-second units in which the 5-second sample was 9 or less for 30 at least 30 seconds. This tells us that the baby is not currently suffering from any pathological decelerations. **
For each hour and in most cases, each fraction of an hour of the mother’s labor, IA provides information that allows the primary birth attendant or L&D staff to determine if the FHR baseline is normal (or not), if the variability is normal (or not), whether reassuring accelerations are present (or not) and if any pathological decelerations are detected.
Charting IA data
All this is charted, so there is a record of the baby’s FHR over the course of the labor that accompanies information on the mother’s stage of labor, her progress and any other pertinent medical factors. Date from each auscultation can be plotted on a graph after every auscultation (particularly useful if its a longer labor or there are questions about something. But when the FHR is ‘boringly’ normal (the best kind!), most midwives just incorporate the FHR checks into the narrative notes.
I use a simple method that identifies the most frequent 5-second sampling number heard during the one-minute ausculations as the baseline (i.e. the rate for the majority of samplings). I also note the range or variations of the less frequent numbers and record them.
If there is an acceleration is present, there will be 3 or more 5-second units that are higher than the baseline 11s (12s, 13s, occasional 14). If one or more deceleration is heart, it will be counts that are below 11, or 10s, 9s, 8, etc).
Let’s use the example in a few paragraphs above. The different numbers generated by 12 sets of 5-second samplings were –> 12, 12, 11, 12, 11, 12, {**13, 14, 13}, 11, 10, 11, 12, 12, which would be charted as a baseline of 144, with normal variability, one acceleration and no decels. So here is how that conclusion was reached and how it would be charted.
- First, the baseline of 144 was based on a preponderance of 12s.
- Normal variability was established by a at least a few of those 5-second units being higher or lower than 12; in this case there were 4 lower (10s and 11s) and 3 higher (13s).
- Accelerations were noted with a run of three consecutive sets above the baseline number of 12, in this case, two 5-second sets of 13, and one of 14 (over a total of 15 seconds).
- There were NO decels.
So the baseline would be charted as the numeral 144, then would chart all the numbers counted over the course of one (or more) minutes. I don’t mean writing done each 5-second count, just the various number heard during the one minute auscultation. In this particular, but not necessarily typical instance, that was one 10, several 11s, 12s, 13s and one 14.
On my paper charts, I list all of them, which records the range of variation, then I put a vertical line of 3 small checks over the baseline (number heard most often that becomes that is charted as the baseline) and 2 checks over the next most frequent number (in this example, 11s) and 1 check over the least frequent, in the case a number lone 14.
@@@ IA graph for intrapartum charting (ACCM-1999) @@@
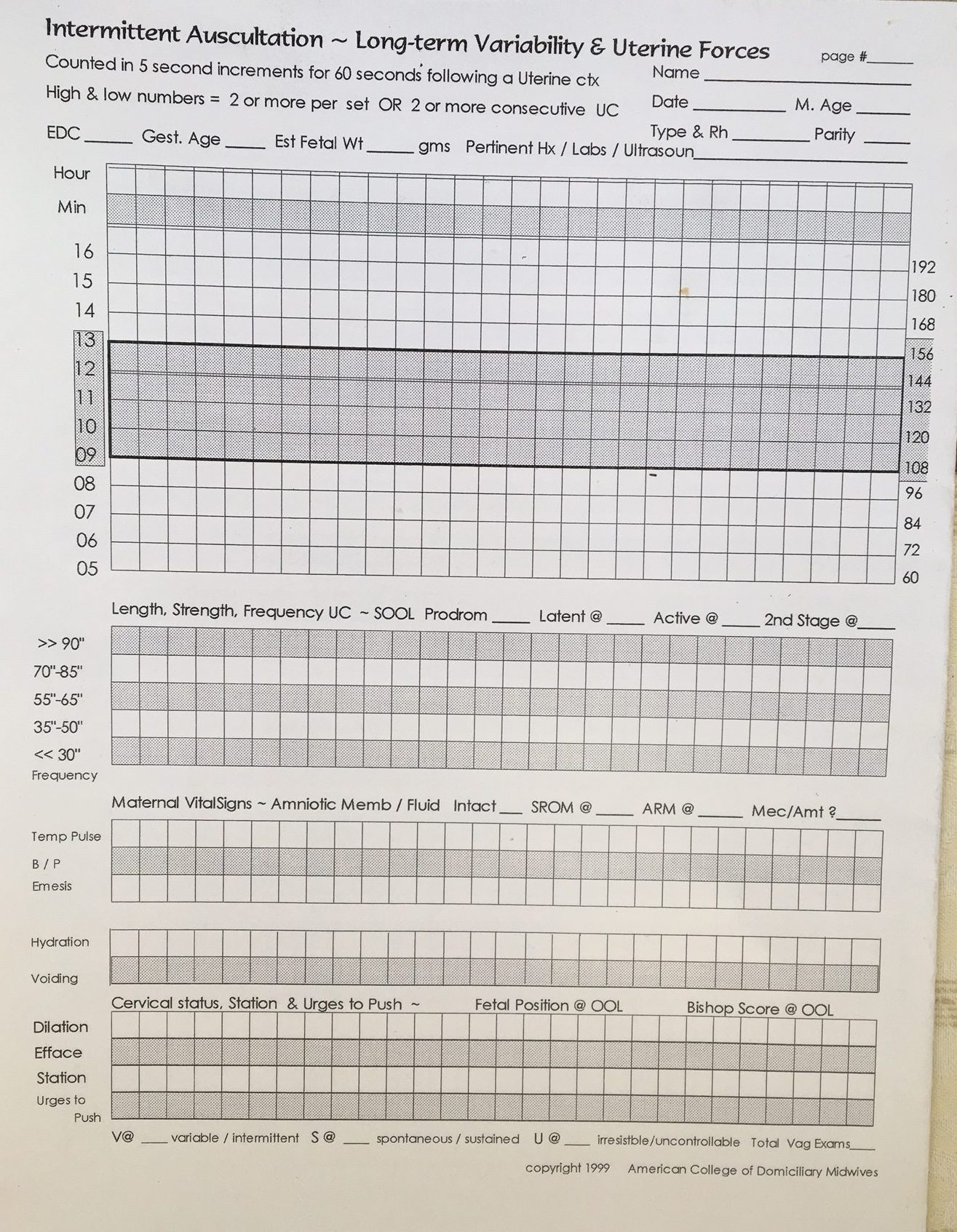
If you use electronic charting, the special category for charting FHTs will not let you record these fine distinctions. However, you can put this same IA data in the narrative part of the record, and while you can’t put checks over number, you can list the as (a) most frequent, (b) next most frequent and (c) least frequent.
Outliers, Artifacts and Errors: The reason for these find distinctions is to avoid using a random high or low number — i.e. an outlier that could be an artifact or error –to make determinations that are not justified by the facts.
For example, after hearing a super low 5-second sampling of 6 or a super high of 16 is not by itself, it’s not appropriate to diagnose bradycardia, tachycardia or fetal distress all by themselves. To represent “actionable information“, practitioners must first confirm this abnormality with additional monitoring. If they find them to be repeated with enough frequency to indicate a problem that needs to be evaluated or requires emergent treatment.
A Parting Comment on Quartz Watches and Clocks
For prenatal care in my own office, I use a typically use an inexpensive 7-inch quartz clock with big black numbers on a white background and a “tick-stop” second hand ($4.99 @ Target). I have a similar quartz clock that is part of my birth equipment. I set it upright somewhere in the room where the mother is laboring in a place that I can see AND (very important) is completely hands-free.
However, one of my midwife friends (thank you so much, Emily Deckenback, LM) told me about a handy smartphone app that has nearly all the wonderful feathers of my 7″ quartz. It’s great when the moms are somewhere else in the house (like the bathroom). I say nearly, because I have to handle it (extract from my pocket) before i can take FHT. This almost always requires at least two hands to retrieve it from my pocket and find a place to put it down where it won’t fall on the floor or slide into the tub while I am counting FHTs over the course of a minute or two or longer.

Most adverse outcomes discovered after the birth did not have anything to do with the labor or birth
Vast majority of adverse events during the perinatal period having nothing to do with the type of birth attendant (MD vs. midwife) or place of birth (home vs. hospital) but everything to do with prenatal problems of unknown origin.
The professional opinions of experts in this field have concluded that the origin of most unexpected bad outcomes (92%) traces back to prenatal problems for the fetus that arose during the pregnancy or were genetic in nature. These complications had nothing to do with how labor was managed or if an elective Cesarean was performed before labor started.
Cesarean section may be able to take the baby out of the mother’s body, but there is no operation that can take the metabolic acidemia or abnormal DNA (and damage it’s already done) out of the baby.
The scientific literature has repeatedly reported that IA has an equal or better outcome, a conclusion that is a combination of studies and the fact that IA has always been associated with fewer medical interventions and invasive obstetrical procedures than continuous EFM, including reduced operative delivery and CSs rates.
However, only midwives (whether in or out-of-hospital) are educated in the principles of IA, taught the technical skills during their clinical training and experienced in both the art and science and currently using it to monitor labors.
This is not because they couldn’t use EFM if they wanted or needed to, but because IA works so very well when used by practitioners who understand a fetus’s biological response to both normal and abnormal labor and who believe it’s their duty to “Do No Harm”. For community-based midwives, “Do No Harm” means not needlessly exposing the families we serve to the well-known risk of c-EFM and are willing to personally listen to fetal heart tones at least once an hour and for most of the labo, several times an hour.
In slightly more abstract terms, this means we are choosing not to reduce our own risks and the burden to ourselves by shifting the risk and burden to the mother and unborn baby.
Another video for anyone who wants to practice IA skills
