Note-2-self ~ copied to AI project on CALM auscultation incl. providing background info on EFM (last edited 10-25-2023)
Review article from Australia posted
by ScienceDirect.com
Editor’s Preliminary Notes:
In UK and Australia, what we “Yanks” describe as an “electronic fetal monitoring” (EFM for short) is called “CTG“, which is an abbreviation used for cardio – toco – graphy or “cardiotocography“.
So every time you see the initials ‘CTG’ in the following article, think “EFM” for electronic fetal monitoring as a verb, and electronic fetal monitors as a noun.
The Most Common Childbirth Practice in America — EFM — is both unnecessary and dangerous
{https://newrepublic.com/article/122532/most-common-childbirth-practice-us-unnecessary-dangerous}

In spite of the expense of EFM (about $15,000 per unit), this product does not provide any benefit or better “outcomes” for babies or their mothers.
This is a well-established scientific fact, proven over and over again for more than 50 years.

Unfortunately, EFM is routinely used on healthy women in more than 90% of all hospital labors.
The unnecessary and inappropriate use of EFM is directly responsible for a three-fold increase in Cesarean surgeries and indirectly responsible for a subsequent increase in maternal mortality (death) and morbidity (serious complications, often with long-term consequences). {see references at the end of this article}
However, electronic fetal monitoring is a very expensive technology, which means it is especially profitable for the companies that manufacture fetal monitors.
This helps explain why electronic fetal monitoring technology has been found, again and again over the course of 47 years. While it provides NO benefit, EFM has always been associated with both direct and indirect harm to childbearing women.
This has been an established fact since Havenkamp‘s clinical trial comparing the outcomes of EFM to auscultation was published in 1976. This was followed by hundreds of other scientific papers that confirmed their 1976 finding — while EFM had no benefit for babies, it tripled the C-section rate (16%) compared to auscultation (only 6%).
This is a predictable consequence of medically unnecessary Cesarean surgeries and delayed and downstream harm in post-Cesarean pregnancies and mandated repeat C-sections.

Politically-effective Action — Mandatory Product Disclosure
Many other posts on this site call for legislation that would legally require the manufacturers of EFM equipment to include the scientifically established, irrefutable fact that their EFM technology provides NO benefit to the unborn baby, either before or after its birth, while its routine use increases the rate of surgical deliveries and post-cesarean maternal deaths.
Mandatory Product Disclosure (MPD), as is legally required for virtually every other type of medical technology, would establish a legal obligation for obstetrical providers (hospitals and physicians) to inform pregnant and laboring women that intermittent auscultation (IA) has been scientifically established as the most effective method for monitoring fetal well-being during labor and that using continuous EFM during the labor of healthy women with normal pregnancies is associated with three-fold increase in Cesarean deliveries and an elevated level of post-Cesaean maternal mortality.
We must keep in mind that a Cesarean section is major abdominal surgery, which always is accompanied by known and unknown risks and often includes unexpected problems.
Hospitals began replacing auscultation with continuous EFM during labor in the 1970s. At that time, no scientific studies had established that EFM was safer or better than IA. But starting in 1976, multiple comparison studies of EFM vs. IA found that EFM did not benefit the fetus, while at the same time being associated with an increased rate of Cesarean deliveries and multiple intra- and post-op complications, as well as delayed and downstream problem with fertility and future pregnancies.
But most egregious of all is the significant increase in maternal mortality rate following complications of Cesarean surgery and longer hospitalization and re-hospitalization that increases their exposure to iatrogenic (i.e. medical mistakes) and nosocomial harm (i.e. hospital-acquired drug-resistant infections, medication errors, etc).
Women and Birth

Intrapartum cardiotocograph monitoring and perinatal outcomes for women at risk: Literature review
Volume 33, Issue 5, September 2020, Pages 411-418
Literature review for:
Intrapartum cardiotocograph monitoring and perinatal outcomes for women at risk
Abstract
Problem
Caesarean section rates have risen in high-income countries.
One of the potential drivers for this is the widespread use of CTG monitoring.
Background
 Intrapartum cardiotocograph monitoring is considered to be indicated for women at risk for poor perinatal outcomes.
Intrapartum cardiotocograph monitoring is considered to be indicated for women at risk for poor perinatal outcomes.
Aim
This systematic literature review with meta-analysis examined randomised controlled trials and non-experimental research to determine whether cardiotocograph monitoring rather than intermittent auscultation during labour was associated with changes in perinatal mortality or cerebral palsy rates for high-risk women.
Methods
A systematic search for research published up to 2019 was conducted using PubMed, CINAHL, Cochrane, and Web of Science databases. Non-experimental and randomised controlled trial research in populations of women at risk which compared intrapartum cardiotocography with intermittent auscultation and reported on stillbirth, neonatal mortality, perinatal mortality and/or cerebral palsy were included. Relative risks were calculated from extracted data, and meta-analysis of randomised controlled trials was undertaken.
Findings
 Nine randomized controlled trials and 26 non-experimental studies were included.
Nine randomized controlled trials and 26 non-experimental studies were included.
Meta-analysis of pooled data from RCTs in mixed- and high-risk populations found no statistically significant differences in perinatal mortality rates.
The majority of non-experimental research was at critical risk of bias and should not be relied on to inform practice. Cardiotocograph monitoring during preterm labour was associated with a higher incidence of cerebral palsy.
Discussion
Research evidence failed to demonstrate perinatal benefits from intrapartum cardiotocograph monitoring for women at risk for poor perinatal outcome.
Conclusion
There is an urgent need for well-designed research to consider whether intrapartum cardiotocograph monitoring provides benefits.
Introduction
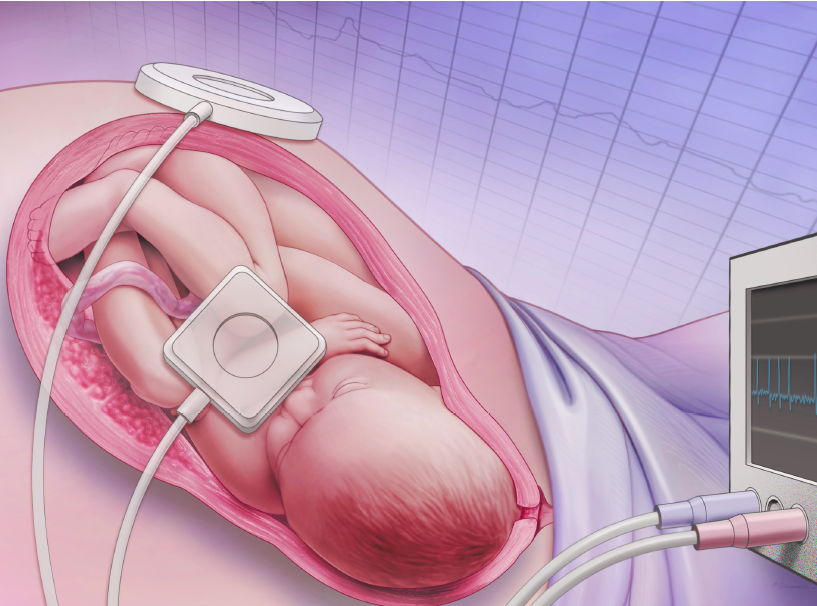 Intrapartum cardiotocograph (CTG) monitoring was introduced in the 1970s.1 The CTG records and displays the fetal heart rate and uterine tone over time making it possible to examine relationships between heart rate and uterine activity. Fetal heart rate patterns are considered to provide physiological information regarding oxygenation of the fetus.2
Intrapartum cardiotocograph (CTG) monitoring was introduced in the 1970s.1 The CTG records and displays the fetal heart rate and uterine tone over time making it possible to examine relationships between heart rate and uterine activity. Fetal heart rate patterns are considered to provide physiological information regarding oxygenation of the fetus.2
During labour a reduction in placental blood flow occurs during uterine contractions.3 This reduction may place the fetus at risk for low oxygenation.4 Hypoxia is presumed to be responsible for a proportion of perinatal deaths and cases of cerebral palsy (CP).5, 6
CTG monitoring was introduced as a screening tool in order to detect fetal hypoxia so that corrective action could be taken.7 The goals of intrapartum CTG monitoring include reducing perinatal mortality and CP. CTG monitoring confers no benefits over intermittent auscultation (IA) for women considered to be at low risk for poor perinatal outcome.8
 Most professional guidelines regarding intrapartum fetal monitoring therefore consider that IA is appropriate for women at low risk.
Most professional guidelines regarding intrapartum fetal monitoring therefore consider that IA is appropriate for women at low risk.
Continuous intrapartum CTG monitoring for women at risk is universally recommended within professional guidelines.9, 10, 11, 12, 13 Caesarean section rates have increased over the past two decades,14 with clear evidence that use of CTG monitoring contributes to increases in the use of cesarean section.15
Rates of maternal mortality and significant maternal morbidity appear to be increasing in some high-income countries16 and are associated with rising cesarean section rates.17, 18
The Royal Australian and New Zealand College of Obstetricians and Gynaecologists Intrapartum Fetal Surveillance guideline acknowledges that evidence from randomized controlled trials (RCTs) do not demonstrate a perinatal benefit from intrapartum CTG monitoring for infants born to women with risk factors but suggests that non-experimental evidence supports this practice and therefore justifies the guideline’s recommendations for CTG use.9
No systematic review of non-experimental research regarding intrapartum CTG use in high-risk women has previously been undertaken. The Cochrane review of RCTs investigating intrapartum CTG monitoring included subgroup analyses for high and mixed-risk populations of women, but this information was not foregrounded within the review making it easy to overlook.
Given that CTG monitoring is associated with surgical risks for women, it is important to revisit the evidence regarding intrapartum CTG monitoring to ensure that current efforts to reduce perinatal hypoxic injury and death are effective and balance this risk.
The research question underpinning this systematic literature review and meta-analysis was: does continuous intrapartum CTG monitoring modify the risk for fetal or neonatal mortality, or cerebral palsy, for infants born to women who are considered to be at increased risk of experiencing perinatal mortality or CP? In order to address this question evidence from both RCTs and non-experimental research was examined.
Section snippets
Literature search
This systematic literature review was registered prospectively with PROSPERO (CRD42018114637). The PubMed, Cumulative Index to Nursing and Allied Health Literature, Cochrane Library, and Web of Science databases were searched in November 2018 and updated in July 2019. The search string used was (“Cardiotocography” OR “Fetal Monitoring” OR “Monitoring, Physiologic”) AND (“Labor, Obstetric” OR “Delivery, Obstetric”). The search was limited to English language publications, humans and no date
Non-experimental research
Twenty-seven non-experimental papers reported data between 1972 and 2018. Data from Fleet et al.24 and Hopkins et al.25 were merged, as the earlier paper provided data prior to and the latter provided data after CTG monitoring was introduced.
Most research (n = 16) was undertaken in the United States of America (USA). The remainder was conducted in Canada (n = 3), Denmark (n = 2), the United Kingdom (UK) (n = 1), Africa (n = 1), Germany (n = 1), Israel (n = 1), Norway (n = 1), and Switzerland (n = 1).
Discussion
Only non-experimental studies at critical risk of bias showed reductions in perinatal mortality related to intrapartum CTG monitoring. During the 1970s and 1980s significant advances occurred in neonatal care.62, 63 Contraception and pregnancy termination became increasingly available, and there was a reduction in preterm birth, which is known to be a strong determinant of perinatal mortality.64 These changes occurred contemporaneously with the introduction and expansion of CTG use and may well ????? (no further text available on their website)
Conclusion
Evidence from quality non-experimental research and RCTs shows no difference in the rates of stillbirth, neonatal mortality or perinatal mortality between the use of IA or CTG monitoring during labour in populations that include or consist of women considered to be at increased risk for poor perinatal outcome. Intrapartum fetal surveillance guidelines which recommend CTG monitoring for women considered to be at risk are not consistent with the evidence base. Clinicians and professional bodies
Ethics statement
None declared.
Funding
None declared.
Conflict of interest
None declared.
CRediT authorship contribution statement
Kirsten A. Small: Conceptualization, Data curation, Formal analysis, Methodology, Writing – original draft, Writing – review & editing. Mary Sidebotham: Supervision, Validation, Writing – review & editing. Jennifer Fenwick: Supervision, Writing – review & editing. Jenny Gamble: Supervision, Validation, Writing – review & editing.
Acknowledgments
The authors would like to acknowledge the assistance of Ms Bonnie Dixon, Health Librarian, Griffith University who assisted in structuring the search terms, and Professor Rob Ware, Menzies Health Institute, for statistical advice.
References (66)
- et al.
Electronic fetal monitoring: past, present, and future
Clin Perinatol
(2011)
Understanding cardiotocographic patterns associated with intrapartum fetal hypoxia and neurologic injury
Best Pract Res Clin Obstet Gynaecol
(2013)
Oxygenation of the placental-fetal unit in humans
Respir Physiol Neurobiol
(2011)- et al.
Cerebral palsy: causes, pathways, and the role of genetic variants
Am J Obstet Gynecol
(2015) - et al.
FIGO consensus guidelines on intrapartum fetal monitoring: cardiotocography
Int J Gynaecol Obstet
(2015) - et al.
No. 197b-fetal health surveillance: intrapartum consensus guideline
J Obstet Gynaecol Can
(2018) - et al.
Maternal mortality after cesarean section in the Netherlands
Eur J Obstet Gynecol Reprod Biol
(2018) - et al.
Predictors of intrapartum fetal distress: the role of electronic fetal monitoring. Report of the National Institute of Child Health and Human Development Consensus Development Task Force
Am J Obstet Gynecol
(1979) - et al.
Intrapartum electronic fetal heart rate monitoring versus intermittent auscultation: a meta-analysis
Obstet Gynecol Surv
(1995) - et al.
Efficacy and safety of intrapartum electronic fetal monitoring: an update
Obstet Gynecol Surv
(1995)
Cited by (13)
-
The social organisation of decision-making about intrapartum fetal monitoring: An Institutional Ethnography
2023, Women and BirthCitation Excerpt :In 2018, Sartwelle and Johnston [8] asserted that ongoing widespread use of intrapartum CTG monitoring was unethical, arguing that those who promote its use are using “junk science” (p. e24). No perinatal benefit has been demonstrated from the use of intrapartum CTG monitoring – even for women considered to be at risk for poor outcome – and women face additional risk of harm because of higher rates of instrumental and caesarean births [9–11]. English researchers surveyed pregnant women about their views and found the vast majority expressed a desire to make decisions regarding intrapartum fetal monitoring [12].
-
The overuse of intrapartum cardiotocography (CTG) for low-risk women: An actor-network theory analysis of data from focus groups
2022, Women and BirthCitation Excerpt :International and national guidelines for Fetal Heart Rate Monitoring from WHO [7], FIGO [8], ICM 2017 [9], and NICE [10] recommend IA for healthy, low-risk women. These guidelines recommend continuous CTG monitoring for pregnant women with risk factors, although there is no evidence of any actual benefit [6]. Additionally, the guidelines from Australia, Denmark, New Zealand, and Norway, the four countries included in the present study, recommend IA for low-risk pregnancies [11–13].
-
Wanting to be ‘with woman’, not with machine: Midwives’ experiences of caring for women being continuously monitored in labour
2022, Women and BirthCitation Excerpt :For women identified as having a complex pregnancy or being at high risk of complications in labour, continuous electronic fetal heart rate monitoring (CEFM) is recommended by numerous local and international guidelines [4,5,37]. Clinical guidelines recommending CEFM persist despite a lack of evidence for the ability of CTG to improve maternal and neonatal outcomes [6,7]. Women with complex pregnancies are often monitored in labour via a cardiotocograph (CTG), commonly referred to as CTG monitoring.
-
Experiences and outcomes on the use of telemetry to monitor the fetal heart during labour: findings from a mixed methods study
2022, Women and BirthCitation Excerpt :Women are also unable to use a birthing pool with wired CEFM. Despite the lack of high quality evidence for the benefits of CEFM in reducing adverse outcomes [8,9], it continues to be used widely in modern maternity care, and is set to increase with higher levels of maternal complexity and intervention. Wireless CEFM, or telemetry, has advanced in its technology and capability so that modern machines can be purchased as an adjunct to existing cardiotocograph (CTG) facilities, are waterproof, have a longer range and result in better recording of the fetal heart than older models.
Recommended articles (6)
-
Research article
Admission cardiotocography: A hospital based validation study
European Journal of Obstetrics & Gynecology and Reproductive Biology, Volume 229, 2018, pp. 26-31 -
Research article
Combining intermittent auscultation and contraction palpation monitoring with cardiotocography in inpartu mothers
Enfermería Clínica, Volume 30, Supplement 2, 2020, pp. 547-549 -
Research article
What would Florence think of midwives and nurses in 2020?
Women and Birth, Volume 33, Issue 5, 2020, pp. 409-410 -
Research article
Quantitative cardiotocography to improve fetal assessment during labor: a preliminary randomized controlled trial
European Journal of Obstetrics & Gynecology and Reproductive Biology, Volume 205, 2016, pp. 91-97 -
Research article
FIGO consensus guidelines on intrapartum fetal monitoring: Cardiotocography
International Journal of Gynecology & Obstetrics, Volume 131, Issue 1, 2015, pp. 13-24 -
Research article
Continuous cardiotocography during labour: Analysis, classification and management
Best Practice & Research Clinical Obstetrics & Gynaecology, Volume 30, 2016, pp. 33-47
