Amy Tuteur’s Fact-Free Zone, recent NYT article; how Americans have been conditioned to think “… home birth is so dangerous” & why they are so wrong!

Fact-free Zones scare the be-jesus out of people! Scaring people is not nice.
A Fact-free diet . . .
. . . is dangerous to your mental health!
Little Miss Amy just keeps doing what she does so well — making a stink in ways that virtually eliminate the corrective process for the mis- and disinformation that her tirades contain. I guess that comes with the territory; since she would lose if being ‘fair and balanced’ was her style.
I’ve had more than one delicious fantasy of tying her to a chair and making her watch 48 straight hours of Sponge Bob-Square Pants cartoons. But I also know that she provides us with something that is very valuable.
First, Amy-2-2 says (screams) what a lot of other people are thinking but just don’t talk about.
Second, she clearly demonstrates that as educated communicators, we aren’t doing our job very well.
The first few sentences in her NYT post cuts to the chase of this issue. What she identifies as a core element (i.e. claiming it to be an indisputable ‘fact’) is a historical mistake or misunderstanding. In spite of being an MD and obstetrician, she knows nothing about the actual dangers of childbirth for essentially healthy American mothers living in a modern society with a functional health care system and access to high-quality prenatal care.
Amy-2-2 start off by saying:
“Childbirth is inherently dangerous, and if an emergency occurs, the baby or even the mother may die.”
Consider how this sentence would read if the word “childbirth” were exchanged for “travel” and “passengers” for “mother and baby”.
“Travel is inherently dangerous and if an emergency occurs, the passengers may die”
We’d immediately make the critical distinction between “possibility” and “probability”, and admit that yes, if certain types of emergencies were to occur, someone might die. However, we still drive cars, ride in buses and trains and fly in airplanes.
While this author wants us to believe that death in childbirth is a ‘probability’, this is only true for the pre-scientific era (prior to Pasteur’s 1881 publication of germ-theory) and/or contemporary third world countries with NO functional healthcare system w/ prenatal care and/or no access to comprehensive medical services if there is an emergency.
She continues:
Indeed, in the United States, the switch from home birth to hospital birth over the 20th century was accompanied by a more than 90 percent decrease in neonatal mortality and nearly 99 percent decrease in maternal mortality.
That statement is neither true nor helpful.
A physician who was also a statistician for the Metropolitan Life Insurance Company concluded in 1932 that if midwifery care of the quality provided by the Frontier Nurse (Midwifery) Services was generally available to childbearing women it would prevent the deaths of 10,000 American mothers, there would be 30,000 fewer stillbirth and 30,000 fewer neonatal deaths each year. What this tells us is that hospital-based obstetrical care was not as safe as the care provided by these nurse-midwives.
 Facts ~ the all-purpose antidote!
Facts ~ the all-purpose antidote!
The excerpt indented below {*} is from an excellent and extremely informative study on The Decline in Maternal Mortality in Sweden by Ulf Högberg. Am Jour Public Health: August 2004, Vol. 94, No. 8. [1].
It identifies the role of midwives in Sweden with keeping their maternal mortality rate in the early 1900s orders-of-magnitude lower than the US, which refused to professionally train and provide access to midwives as the provider of choice for healthy women with normal pregnancies.
But before you click on the link, a little history about Swedish midwifery and physician-providers of maternity care would be helpful.
Sweden already had a two-hundred-year-old tradition of care by professionally-trained, community-based midwives that included consultation with local GPs and transferred to regional hospitals for obstetrical services as needed. Then in 1881, the Swedish Parliament passed a national law requiring all midwives and physicians who attended ‘cases of childbirth’ to abide by aseptic principles and the use of sterile technique as appropriate. The result was a significant drop in their already low childbirth-related mortality.
Sweden’s MMR was so much lower than the US that a handful of American obstetricians visited Sweden in the early 1900s to find out “how they did it”. The answer — an autonomous midwifery-based maternity system — apparently didn’t appeal to these American obstetricians!
As you read the stats below, keep in mind that in the early 20th century the US could have, but didn’t adopt a professional midwifery model for providing maternity care to essentially healthy women. Had they done so, American families would have received the same benefit — dramatically fewer childbirth-related deaths — that Swedish families were enjoying.
{**} “In 1900, the US reported an MMR of 667 maternal deaths per 100, 000 live births [2]. At this same , Sweden had the lowest annual MMR of any developed country — only 230 per 100,000 lives.
The low maternal mortality rates reported for the Netherlands, Norway, and Sweden in the early 20th century are identified by researchers to be a result of an extensive collaboration between physicians and highly competent, locally available midwives in the Netherlands, Norway, and Sweden. [1]
But one thing is indisputable — the standard for normal maternity care in these countries was physiological, whether it was being provided by physicians or state-regulated midwives.”
[2] CDC ~ MMR 1900 to 1999: Achievements in Public Health, 1900-1999: Healthier Mothers and Babies mmwrq@cdc.gov

Forceps Delivery
As the use of invasive obstetrical procedures became increasingly routine in the US, the total number of maternity deaths shot up by 15% a year for the next decade, and neonatal birth injuries increased by 40%. In 1916, there were 16,000 maternal deaths reported; by 1925, the rate rose to 25,000 or an MMR of 1,250 per 100,000.
Sweden’s MMR of 230 per 100K MMR in 1900 continued to drop with each decade of the 20th century while the MMR in the US just kept going up and up. Regrettably, the statement that “childbirth in the US was dangerous” was true, but not for the reasons claimed by Amy Tuteur.
In addition to the Swedish paper and CDC report, many other reputable published sources also debunk the notion that invasive style of American obstetrics was responsible for the “90% drop” in childbirth mortality during the 20th century.
Historical information on the positive relationship btw the use of midwifery care and lower mortality and morbidity for mothers and babies
A particularly frank and formal admission of these facts was testimony provided during the White House Conference on Child Health and Protection by the Committee on Prenatal and Maternal Care on the efficacy of midwifery care: (Reed, 1932)
“…that untrained midwives approach and trained midwives surpass the record of physicians in normal deliveries have been ascribed to several factors.
Chief among these is the fact that the circumstances of modern practice induce many physicians to employ procedures which are calculated to hasten delivery, but which sometimes result in harm to mother and child.
On her part, the midwife is not permitted to and does not employ such procedures. She waits patiently and lets nature take its course.” (original emphasis)
In stark contrast is a 1975 quote in the New York Times Magazine, which is the perfect “bookend” for Amy Tuteur’s 2016 NYT article:
“In the United States in the early part of this century, the medical establishment forced midwives — who were then largely old-fashioned untrained “grannies” — out of the childbirth business.
Maternal and infant mortality was appallingly high in those days…
As the developing specialty of obstetrics attacked the problem, women were persuaded to have their babies in hospitals, and to be delivered by physicians….
Today it is rare for a woman to die in childbirth and infant mortality is (low)…” [Steinmann, 1975]

Note how the umbilical cord is already drained of blood at the moment of birth — likely a consequence of the general anesthesia administered to its mother before the baby was born
But aside from biased propaganda, the public perception of this topic is still an incredibly complicated issue.
A trivial but still influential issue is the “yuk” factor — childbirth and its biology (the “you-know-down-there” conversation) is something many men and women don’t want to talk about.
The 800-pound gorilla, make-it-or-brake-it issue is safety and each person’s perception of relative danger vs. safety.
During the pre-antibiotic era (before May of 1945), the large number of fatal complications associated with hospitalization and the invasive model of obstetrics resulted in a huge increase in maternal mortality from sepsis.
Then within a relatively short time, a series of great leaps in medical science created what we think of today as ‘modern medicine’. This historical phase began with the invention of the world’s first safe and effective antibacterial drugs — sulfa, which became available in the US in 1938, and penicillin in 1945. Other significant medical advances included safer anesthetics, safer blood transfusions, better surgical techniques brought back by WWII battlefield surgeons, better pharmaceuticals, and improved diagnostic technologies.
These new life-saving abilities — particularly antibiotics — were nothing short of a medical miracle that allowed obstetrical providers to effectively treat many previously fatal conditions. This quickly brought down the artificially high rate of maternal and neonatal deaths from iatrogenic complications (primarily infection and hemorrhage) to levels consistent with maternal mortality in many other industrialized countries.
However, the issue of causation — iatrogenic vs. unavoidable death — was invisible to the public. The PR arm of obstetrics loudly and frequently insisted that the historically high level of maternal and perinatal deaths was the fault of midwives and OOH birth and the public naturally believed them.
Personally, I think the “Call the Midwife” producers should do a TV series on the fascinating history of 20th-century obstetrics in America. It’s just a happenstance of history that transformed the biological event of normal childbirth into a surgical procedure. During the pre-antibiotic era, this was done in a last-ditch effort to reduce the rate of puerperal sepsis in hospitalized maternity patients. In 1910 a formal decision was made by DeLee and Williams to Listerize the entire 2nd stage labor as the new standard of care.
 What changed normal childbirth from the normal biological activity of the childbearing woman (who gives birth) into the new surgical procedure of “vaginal delivery” (in which the woman is being delivered by another person) was the decision to conduct the entire 2nd stage of labor under the full principles of surgical sterility. Dr. DeLee defined this as the same level of sterile technique that would be used when performing an abdominal operation.
What changed normal childbirth from the normal biological activity of the childbearing woman (who gives birth) into the new surgical procedure of “vaginal delivery” (in which the woman is being delivered by another person) was the decision to conduct the entire 2nd stage of labor under the full principles of surgical sterility. Dr. DeLee defined this as the same level of sterile technique that would be used when performing an abdominal operation.
However, conscious women in the throes of pushing-stage labor, even when strapped to the narrow delivery table, still insisted on moving around, talking, coughing, and touching themselves (“you-know-down-there!”), grabbing the doctor’s hand and other things, all of which contaminated the OR and thus the surgeon’s sterile field. If a new mother were to become septic after the birth, how could a physician-obstetrician successfully defend himself against claims by the family that the infection was iatrogenic in origin if he could not point to the use of a flawless and impeccable sterile technique in the delivery room?
As noted by Dr. DeLee, it quickly became apparent that mother would have to be put to sleep to properly protect the surgeon’s sterile field. After all, Dr. Lister’s historical process for performing operations under sterile conditions required the surgical patient to remain perfectly still and completely immobilized under general anesthesia. However, the obstetrical use of chloroform and ether were associated with respiratory depression, especially in newborns. To limit exposure to both mother and baby to anesthetic gases, episiotomy, forceps and manual removal of the placenta were routinely performed.
At this point, NSVD was really was a surgical procedure. This also represents the most profound change in childbirth practices in the history of the human species.
The surgical procedure of NSVD takes on a whole new life of its own!
In 1931, the AMA created a committee to develop what we call new refer to as ICD codes, that is, a way to systemize the reimbursement process for hospitals and physicians. The two surgeons on this committee concluded that the surgically managed ‘procedure’ of vaginal birth was rightfully monetized under a surgical billing code, which continues to be the case today.
Of equal or even greater concern, no non-surgical or physiologically-based billing code was created by the Committee to fairly compensated GPs and family practice physicians for being physically present throughout the intrapartum. Unlike hospital midwives who get paid for their time, there is no way for a doctor to bill for the considerable expenditure of professional time required to provide appropriate physiological support for active labor, spontaneous birth and the immediate PP-NN period.
Interventive obstetrics & public perceptions of childbirth as dangerous
In the obstetrical battle for the hearts and minds of Americans, there is another mistaken but very powerful association that helped to create and continues to maintain the status quo. An interlocking and self-reinforcing relationship exist btw the historical version of obstetrics and the widespread perception by Americans (especially the medical profession) that normal childbirth was (and is) extremely and inherently dangerous. In a weird convoluted way, this has similarities to the “Stockholm syndrome”.
To describe this requires a word picture that begins with the obstetrical model as it was historically applied to healthy women (1910 to 1975). When I retired from L&D nursing in 1975 — what I call the “Dark Ages of the deep South” — the norm in our hospital was little changed from 1910 model personally promoted by Dr. J. Whihrige Williams.
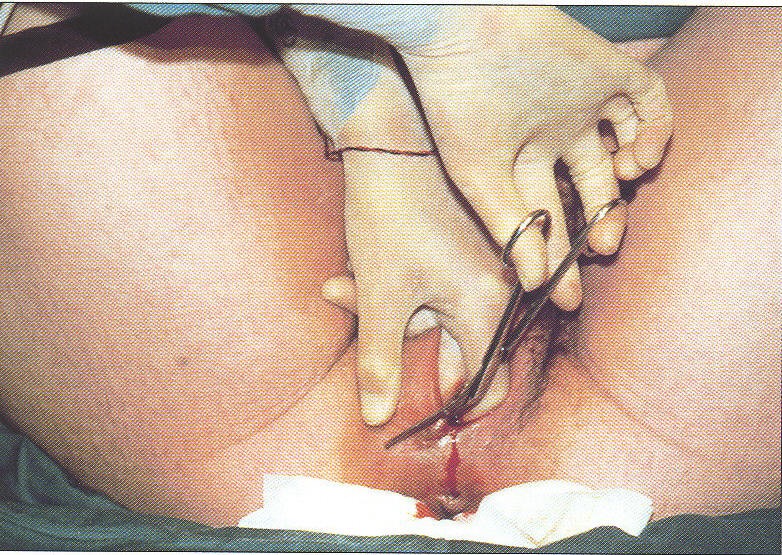
Obstetrician cutting an episiotomy with a pair of sterile surgical scissors.
Our nurses were required to medicate 100% of labor patients with scopolamine and narcotics; families were 100% excluded; delivery occurred in an OR-outfitted Del Rm and included gen. anesthesia, episiotomy, low-forceps, manual removal of placenta, and suturing of perineal incision (including the infamous ‘husband stitch!)
Now mentally picture all the public’s impression of ‘modern’ medicine during this pre-antibiotic era (circa 1881-1940), with its extraordinary new and ‘scientific’ abilities. Hospitals had well-staffed, well-lighted obstetrical departments that scrupulously used Lister’s antiseptic and aseptic methods.This included an “Authorized Personnel Only” sign on the door to the labor ward (i.e., no family members allowed) to prevent the spread of ‘germs’ to the new mother and baby. Obstetrically-trained surgeons performed the surgical procedure of vaginal delivery in the sterile conditions of an operating room.
What could possibly go wrong?
But in spite of all this chrome, chloroform, antiseptic soaps, and surgical sterility, and the very best efforts of all these highly educated, well-meaning professionals and advanced emergency services only available in a hospital, the result was still a horrifically high level of very bad outcomes.
At its highest point (1925) there was one maternal death out of every 80 births. A frequently repeated, distressing experience for every community was news of a newly-widowed husband, emotionally devastated (sometimes orphaned) kids, other grieving family members, neighbors, schools, and church congregations. To get some idea of the sociological impact of this, consider that the actual risk of an Israeli citizen dying as a result of Palestinian terrorism is only 1 in 10,000. Think how it much would distort normal life if it were 1 in 80.
So the logical conclusion was simple and straightforward –– normal childbirth, even in the healthiest of women, even in the hands of the best professionals and most respectable hospitals, is by nature horribly dangerous.
When Mother Nature is seen as a biological terrorist, then you can’t have “too much” obstetrical intervention, just as we now believe we can’t have too much protection against modern-day pseudo-Islamic terrorism (which is a syndicated crime and not a religion).
The following is my statistical synopsis of maternal mortality in the US from the citations above:
Despite heroic efforts and rigorous application of antiseptic practices and aseptic principles, childbirth septicemia in the US was still the largest single category of mortality, accounting for one-third of all maternal deaths.
From 1900 to the post-WWII baby boom in 1950, the birthrate held steady at 2 million, which makes a comparison of this record of the first half of the 20th century more informative.
According to one source, the average MMR per 100,000 live births from 1900 to 1915 was 607.9 or 1:165
• By 1925, the MMR had risen to an all-time high of 1,250 or 1:80.
• By 1931, MMR had fallen to 670 or 1:149. This was still higher than the early 1900s, but significantly less than the high water mark between 1915-1925.
• In 1938, it had dropped to 440 or 1: 227.
• By 1940 it had further fallen to 363.9 or 1:274
• Between 1940 to 1990, race-specific ratios declined from 319.8 to 5.7 for white women and from 781.7 to 18.6 for black women.
{the nxt paragraph was already included above; it compared MMR between the US, Sweden, and other Scandinavian countries during the early decades of the 20th century}
 When reading these awful numbers, it’s easy to be critical of Drs. Williams and DeLee, Titians of their time and still referred to as the “fathers of American obstetrics. I don’t have a lot of personal information about Dr. Williams, but I know that Dr. DeLee was genuinely concerned about the fate of his poor and immigrant maternity patients. To that end, he was an astute and honest observer and accurate reporter, even when what he had to say was not popular within his own profession.
When reading these awful numbers, it’s easy to be critical of Drs. Williams and DeLee, Titians of their time and still referred to as the “fathers of American obstetrics. I don’t have a lot of personal information about Dr. Williams, but I know that Dr. DeLee was genuinely concerned about the fate of his poor and immigrant maternity patients. To that end, he was an astute and honest observer and accurate reporter, even when what he had to say was not popular within his own profession.
In 1936, when the Cesarean section rate in the US was under 3%, Dr DeLee was interviewed in a Kansas City newspaper article as saying:
“the increasing tendency to perform Caesarean section is to be condemned.
He went on to note that:
“Puerperal infection still causes about 4,000 deaths a year in the U. S. The frequency of operations which are followed by infection is a contributing cause.” [ref]
In his 1924 textbook, Dr. DeLee hits the nail on the head when describing why the systematically intrusive procedures of obstetrical ‘delivery’ were associated with a rising mortality rate:
“Let the [the mother’s] natural immunities be broken down, as by severe hemorrhage … or let a new virulent bacterium be introduced; let the accoucheur in his manipulation carry too many of the vaginal bacteria up into the uterus (a procedure not entirely avoidable), or let him, by his operations, bruise and mutilate the parts too much, or let him break up the protective granulation referred to, and the germs will rapidly invade the system, producing a disease know as puerperal infection, termed by the older writers as child-bed fever.
The asepsis of the patient, therefore, consists mainly in the preservation of her immunities by sustaining her strength, procuring a normal course of labor, avoiding the necessity for operative interferences, and conducting these with the least possible amount of damage.” [p. 292-293, parenthetical notations in original text]
I characterize stories of this era as “How Normal Childbirth Got Trapped on the Wrong Side of History: the perfect storm that turned healthy women into patients of a surgical specialty, and normal childbirth into a surgical procedure ~ the last and most important UNTOLD story of the 20th century.
I continue to believe that we have to unwind this Gordian knot of how maternity care for healthy women was erroneously “obstetricalized”. While these decisions were well-meaning, the result was still a ‘wrong use’ of obstetrics and that has had long-lasting and devastating consequences that are still with us today.
Personally, I hope Amy Tuteur continues to bedevil us until we finally get this problem solved. Only then will we be able to talk about support for the physiological process of normal birth by American midwives as something other than “chaotic”.
The best answer, the only answer is to fix the dysfunctional maternity care system in the US. No woman should ever be forced to choose between a midwife and a physician-obstetrician, or between home and hospital in order to have a physiologically-managed normal childbirth.
 As a matter of national policy, the principles of physiological management for normal birth should be integrated with the best advances in obstetrical medicine to create a single, evidence-based standard for all healthy women with normal pregnancies.
As a matter of national policy, the principles of physiological management for normal birth should be integrated with the best advances in obstetrical medicine to create a single, evidence-based standard for all healthy women with normal pregnancies.
Mastery in normal childbirth services means bringing about a good outcome without introducing any unnecessary harm or unproductive expense.
In such an evidence-based model, the individual management of pregnancy and childbirth would be determined by the health status of the childbearing woman and her unborn baby, in conjunction with the mother’s stated preferences, rather than the occupational status of the care providers (obstetrician, other physician or a professional midwife)
faith gibson, LM
Palo Alto, CA
Small PHB practice
My favorite website ~ www.still-crazy-after-all-these-years.com
Postscript — Anyone who wants to read more of this historical research that i’ve posted, just scroll to the top of this post and click on “HOME”. Links to 7 other sets of information are listed on the home page of faithgibson.org.
