Trapped on the Wrong Side of History ~ Chapter 12: Right & Wrong Use of Gravity ~ Unpublished manuscript
 Chapter 12 — not yet edited,
Chapter 12 — not yet edited,
currently has text for Ch 13 as well as Ch 12

Right and wrong use of gravity:
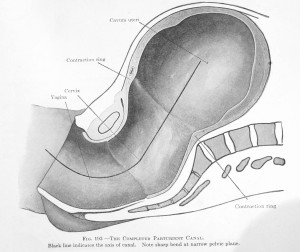
At a meeting of the Radiological Society of North America two radiologists from the University Hospital, Zurich, Switzerland described a pelvimetry study using magnetic resonance imaging (MR) to determine which maternal positions provided the most room for the baby to be born.
The study contrasted the conventional supine position (mother lying flat on her back) to positions in which the mother was squatting or an all-fours ‘hands and knees’ position. A report on their presentation, aptly entitled “Upright Positions Offer Most Room for Delivery”, was published in Ob.Gyn.News [2002;Volume 37 • No 3]. They measured the space available for the baby to pass through at the three critical landmarks of the childbearing pelvis –intertuberous diameter, interspinous diameters, and the sagittal outlet. They discovered that upright positions provided an average of slightly more than a centimeter at each of these junctions.
“Upright birthing positions provide significantly more room for delivery in terms of pelvic dimensions, compared with lying supine, Dr. Thomas Keller said. He and his colleagues …who performed MR pelvimetry on 35 non-pregnant women to compare pelvic bony dimensions in the supine, hand-to-knee, and squatting positions.
These differences are statistically significant and confirm the advantages of birthing positions long practiced in other cultures, the study’s coauthor Dr. Rahel Kubik-Huch noted during an interview. [emphasis added]
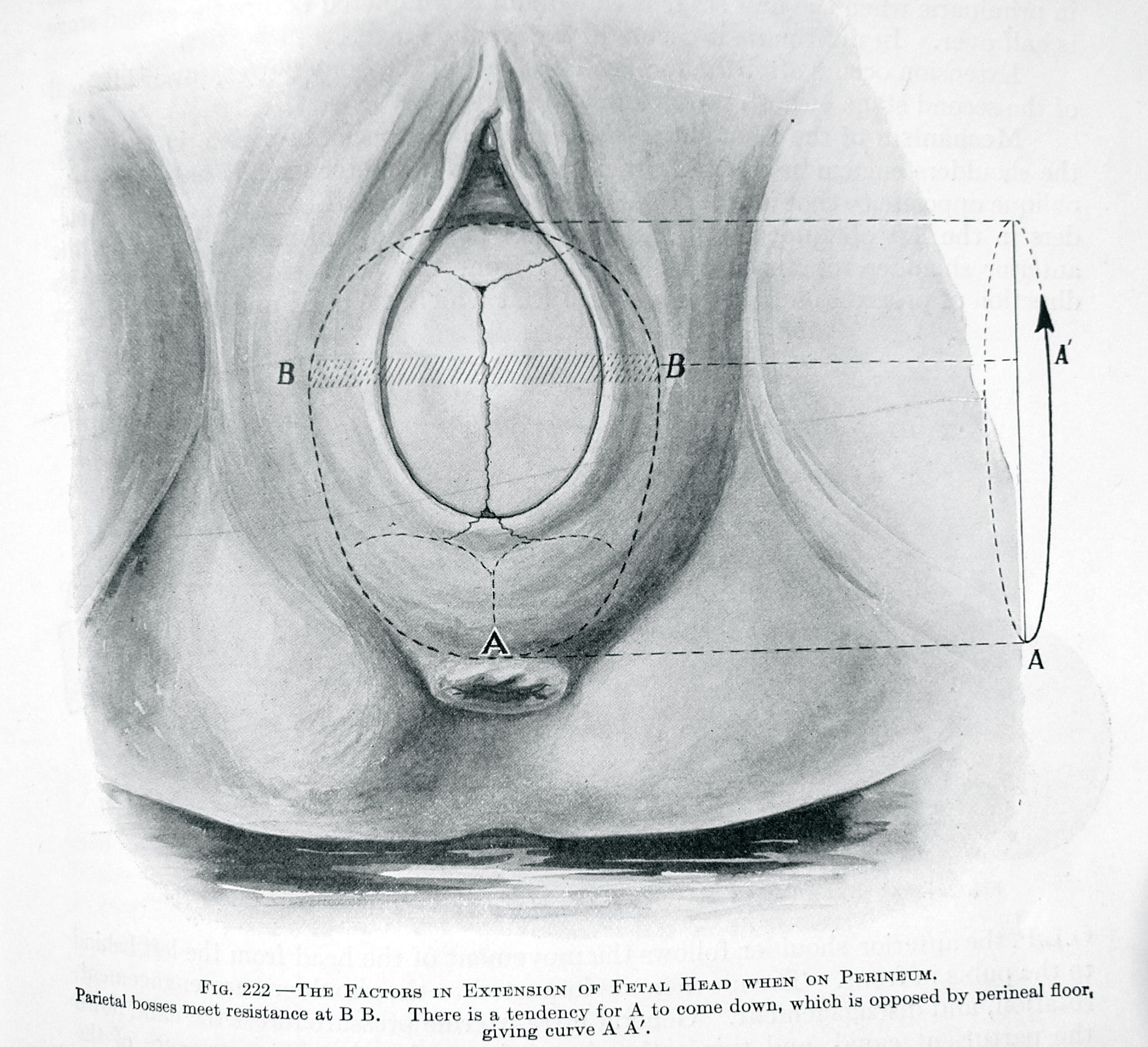
… the theoretical ideal would thus be to adopt the hand-to-knee position to help the presenting part through the interspinous diameter, and to squat rather than remain supine as the [head] traverses the sagittal outlet, said Dr. Kubik-Huch.”
This silly little centimeter of extra space between lying down and standing up can easily be the difference between a spontaneous vaginal birth with a healthy baby and a difficult one that required unusually long and hard pushing, the use of forceps or vacuum to extract the baby or even a Cesarean section that may leave both mother and baby in need of prolonged or specialized care after the birth. It turns out that the ‘right use of gravity’ during the 1st and 2nd stage of labor is the best way facilitate a normal birth. By avoiding the use of obstetrical forceps or vacuum, the soft-tissue of the mother’s pelvis and the unborn baby’s brain are protected from the damage associated with either prolonged pushing or instrumental deliveries.
The Bible of Science-Based Birth Care
The next issue is the efficacy (safety + cost-effectiveness) of the system of obstetrical management for a healthy population of childbearing women. If obstetrical management is to replace physiological forms of maternity care, we should be certain the replacement system is a scientifically sound one that uses evidence-based practices.
For an objective determination on this issue, there are two excellent, well-respected sources that we may turn to. The first is a scientifically researched publication known as ‘A Guide to Effective Care in Pregnancy and Childbirth’ and the second is a survey of contemporary maternity care practices entitled “Listening To Mothers”, commissioned by the Maternity care Association of New York City and conducted by Harris Poll Interactive in 2002.
To determine the scientific aspect of current obstetrical practices we’ll first look to the published work of Drs Ian Chalmers and Murray Enkins and their life-long work — the bible of evidenced-based maternity care — entitled ‘A Guide to Effective Care in Pregnancy and Childbirth’ (GEC). It is a compilation of all pregnancy and childbirth related studies published in the English language in the last 30 years.
 The Guide to Effective Care identifies six levels of effectiveness/efficacy, ranging from the positive end of ‘clearly beneficial’ (category 1) to the negative end (category 6) of ‘likely to be ineffective or harmful’. Using the preponderance of available evidence, Drs Chalmers and Enkins rated each ‘standard’ maternity-care practice and regularly used medical/ surgical interventions for safety and efficacy. Based on these categories, the G E C cautions that:
The Guide to Effective Care identifies six levels of effectiveness/efficacy, ranging from the positive end of ‘clearly beneficial’ (category 1) to the negative end (category 6) of ‘likely to be ineffective or harmful’. Using the preponderance of available evidence, Drs Chalmers and Enkins rated each ‘standard’ maternity-care practice and regularly used medical/ surgical interventions for safety and efficacy. Based on these categories, the G E C cautions that:
“Practices that limit a woman’s autonomy, freedom of choice and access to her baby should be used only if there is clear evidence that they do more good than harm”
“Practices that interfere with the natural process of pregnancy and childbirth should only be used if there is clear evidence that they do more good that harm”
As measured by the six categories identified in the Guide to Effective Care, the “standard of care” presently as provided by obstetricians is extremely discordant when measured by scientific principles (both in practice and in interpretation of scientific studies) and evidence-based practice parameters.
Contemporary obstetrics reverses the recommended safe practices, with those identified as most beneficial and least likely to cause harm (List #1) being the last or least used and those identified as most likely to be ineffective or harmful (List #6) being the primary or routinely used methods. This vastly increases the number of medical and surgical interventions used and the complications occurring, both immediately and downstream.
Maternity Center Association Report “Listening to Mothers”
Information on the childbearing woman’s experience of childbirth and the care she received is strangely missing from most obstetrical sources. For that information we turn to the October 2002 report by the Maternity Center Association “Listening to Mothers: Report of the First National US Survey of Women’s Childbearing Experiences” conducted by the Harris Interactive Polling Service.
The Maternity Center Association (MCA) of New York City, is a non-profit organization established in 1918. It promotes safer maternity care and develops educational materials for expectant parents on ‘evidenced-based’ maternity practices — that is, policies that are based on a scientific assessment of the safety and effectiveness of commonly used methods and procedures.
The MCA commissioned a survey of healthy mothers with normal pregnancies (no premature babies, multiple gestations, breech or sick mothers) who gave birth in the last 24 months to track contemporary obstetrical trends and the quality of care received by healthy childbearing women. The full report (some 60 pages long) is available on the Internet at www.maternitywise.com.
MCA Study Concludes ~ No ‘normal’ birth in American Hospitals
According to the “Listening to Mothers” survey, 99% of healthy pregnant women do not receive science-based maternity care from their obstetrical providers. The average healthy mom was exposed to 7 or more significant medical interventions and/or surgical procedures during a ‘normal’ labor and birth. The document notes that in the previous 24 months (Oct 2000 to Oct 2002) there were virtually NO ‘natural’ births occurring in hospitals. The entire hospitalized population of healthy mothers-to-be were subjected to one or more major interventions. The only women who had a normal birth without medical or surgical interventions were those who had their babies at home or an independent birth center.
It also documented a significant gap between scientific evidence and standard obstetrical practice. Healthy, low-risk women in the United States often receive maternity care that is not consistent with the best research and in fact, is often directly in opposition to scientific recommendations. According the MCA, many people are not aware of the following major areas of concern:
~ The under-use of certain practices that are safe and effective
~ The widespread use of certain practices that are ineffective or harmful
~ The widespread use of certain practices that have both benefits and risks without enough
awareness and consideration of the risks~ The widespread use of certain practices that have not been adequately evaluated for safety and effectiveness
 According the ‘Listening to Mothers’ survey, the majority of childbearing women did not receive the safer and more satisfactory type of care delineated in the top 3 categories (those established as beneficial) and instead were exposed to a plethora of practices in the bottom 3 categories which were rated as of unknown or unproven effectiveness, unlikely to be effective or known to be harmful. These statistics are for healthy women at term with normal pregnancies. Intervention rates would be higher for women medical complications. I posted these stats previous chapters but duplicate them here to make it easier for the reader to understand the extreme disconnection between the four ‘values/goals’ of ethically-based scientific care what is actually being provided in American hospitals.
According the ‘Listening to Mothers’ survey, the majority of childbearing women did not receive the safer and more satisfactory type of care delineated in the top 3 categories (those established as beneficial) and instead were exposed to a plethora of practices in the bottom 3 categories which were rated as of unknown or unproven effectiveness, unlikely to be effective or known to be harmful. These statistics are for healthy women at term with normal pregnancies. Intervention rates would be higher for women medical complications. I posted these stats previous chapters but duplicate them here to make it easier for the reader to understand the extreme disconnection between the four ‘values/goals’ of ethically-based scientific care what is actually being provided in American hospitals.
93% Continuous electronic fetal monitoring;
86% IV fluids and denial of oral food and water
74% Immobilized or confined to bed due to physician preference,
hospital protocols or the limitations imposed by multiple medical devices
(EFM, IVs, epidural catheter, Foley bladder catheter, etc)71% Push and deliver with mother lying flat on her back
67% Artificial rupture of membranes
63% Epidural anesthesia
63% Pitocin induced or accelerated uterine contractions
58% Gloved hand inserted up into the uterus after the delivery
to check for placenta or remove blood clots
52% Bladder catheter
35% Episiotomy
24% Cesarean delivery (12.6% planned/12.4% in labor
11% Operative – one-half forceps, half vacuum extraction
 In a population that was essentially healthy (95% +/-), an astounding 75% of women had some form of surgery performed – episiotomy, forceps, vacuum extraction or Cesarean section. Using the classical definition of operative delivery (CS or forceps/vacuum extraction) the rate for 2002 would be 38% or 2 out of 5. This is twice the rate of operative deliveries reported by physicians in the early 1900s who merely performed operative procedures on 1 out of 5. Intervention rates would be much higher for women with premature labor, multiple pregnancies or frank medical complications.
In a population that was essentially healthy (95% +/-), an astounding 75% of women had some form of surgery performed – episiotomy, forceps, vacuum extraction or Cesarean section. Using the classical definition of operative delivery (CS or forceps/vacuum extraction) the rate for 2002 would be 38% or 2 out of 5. This is twice the rate of operative deliveries reported by physicians in the early 1900s who merely performed operative procedures on 1 out of 5. Intervention rates would be much higher for women with premature labor, multiple pregnancies or frank medical complications.
 The Listening to Mothers survey is consistent with data from the CDC’s (Center for Disease Control) National Center for Health Statistics Vol. 47, No 27, on The Use of Obstetric Interventions 1989-97. It documents a steady annual increase since 1989 in each of these interventions.
The Listening to Mothers survey is consistent with data from the CDC’s (Center for Disease Control) National Center for Health Statistics Vol. 47, No 27, on The Use of Obstetric Interventions 1989-97. It documents a steady annual increase since 1989 in each of these interventions.
A press release dated June 6, 2002 based on the NCHS report “Births: Preliminary Data for 2001” [NVSR Vol. 50, No. 10. 20 pp] for the year 2001 documents a 24.4% CS rate (the same rate as identified by the Listening to Mothers survey). Statistics for the year 2003 show an even higher Cesarean rate – 26.1 in the US and 26.8 in California. http://www.cdc.gov/nchs/releases/02news/birthlow.htm)
As a result of the Listening to Mothers survey, the Maternity Center Association’s recommended:
“ ..more physiological and less procedure-intensive care during labor and normal birth”.
Cesarean Surgery as the 21st century Standard of Care
The cumulative effect of a hundred years of unopposed obstetrical politics is a well-funded and so far remarkably successful 21st century campaign by organized medicine to replace the expectation of a normal vaginal birth (described as far too risky, defined as the obstetrician’s personal risk of litigation) with scheduled Cesarean surgery. Incredibly enough, replacing normal low-risk biology with scheduled abdominal surgery is also being promoted as the better, safer, cheaper and, even more surprising, the ultimate expression of a woman’s “right to choose”. Of course, the claims of improved safety or lowered cost do not square with the facts, but that crucial information has never made it into the media.
 Here is an example of how the 21st century’s ‘new obstetrics’ (circa 1910) is promoting Cesarean Section as the rising star of “industrialized childbirth” (the author’s choice of words):
Here is an example of how the 21st century’s ‘new obstetrics’ (circa 1910) is promoting Cesarean Section as the rising star of “industrialized childbirth” (the author’s choice of words):
“A measure of how safe Cesareans have become is that there is ferocious but genuine debate about whether a mother in the thirty-ninth week of pregnancy with no special risks should be offered a Cesarean delivery as an alternative to waiting for labor. The idea seems the worst kind of hubris. How could a Cesarean delivery be considered without even trying a natural one? Surgeons don’t suggest that healthy people should get their appendixes taken out or that artificial hips might be stronger than the standard-issue ones. Our complication rates for even simple [surgical] procedures remain distressingly high.
Yet in the next decade or so the industrial revolution in obstetrics could make Cesarean delivery consistently safer than the birth process that evolution gave us.
Currently, one out of five hundred babies who are healthy and kicking at thirty-nine weeks dies before or during childbirth—a historically low rate, but obstetricians have reason to believe that scheduled C-sections could avert at least some of these deaths. Many argue that the results for mothers are safe, too. [The Score; Dr. Gawande, the New Yorker, Oct 2007]
 The obstetrical profession is once again confusing cause and effect, as they did in the early 20th century. The 21st century version of goes like this: The outcome of a hundred years of increasingly heavy interference in the biology of normal birth is still a very problematic experience for the obstetrician profession, with a high rate of operative deliveries and long-term morbidity such as maternal incontinence, babies with cerebral palsy and a lot of lawsuits. A negative association is again drawn between these problems and the fundamental nature of childbearing biology, resulting in an assumption that elective Cesarean surgery is the better and safer than normal vaginal birth.
The obstetrical profession is once again confusing cause and effect, as they did in the early 20th century. The 21st century version of goes like this: The outcome of a hundred years of increasingly heavy interference in the biology of normal birth is still a very problematic experience for the obstetrician profession, with a high rate of operative deliveries and long-term morbidity such as maternal incontinence, babies with cerebral palsy and a lot of lawsuits. A negative association is again drawn between these problems and the fundamental nature of childbearing biology, resulting in an assumption that elective Cesarean surgery is the better and safer than normal vaginal birth.
Cesarean section is the ultimate operative intervention and is associated with a birth-related emergency hysterectomy rate 13 times greater than vaginal birth. Complications of Cesarean in subsequent pregnancies include placenta abruption, placenta previa, accrete and percreta. The rate of placental anomalies rises with each subsequent pregnancy, making it the ‘gift’ that keeps on giving.
 The rate of maternal mortality associated with post-cesarean placenta percreta is 7 to 10 %, even in the very best most prepared hospitals. Additional risks to fetuses and infants in post-cesarean pregnancies include placental abruptions (increased fetal demise & stillbirth rate) and uterine rupture. For the baby, being born by cesarean increases the rate of respiratory distress and admission to NICU. A Cesarean birth also increases the rate of asthma during childhood and as an adult by 33 percent.
The rate of maternal mortality associated with post-cesarean placenta percreta is 7 to 10 %, even in the very best most prepared hospitals. Additional risks to fetuses and infants in post-cesarean pregnancies include placental abruptions (increased fetal demise & stillbirth rate) and uterine rupture. For the baby, being born by cesarean increases the rate of respiratory distress and admission to NICU. A Cesarean birth also increases the rate of asthma during childhood and as an adult by 33 percent.
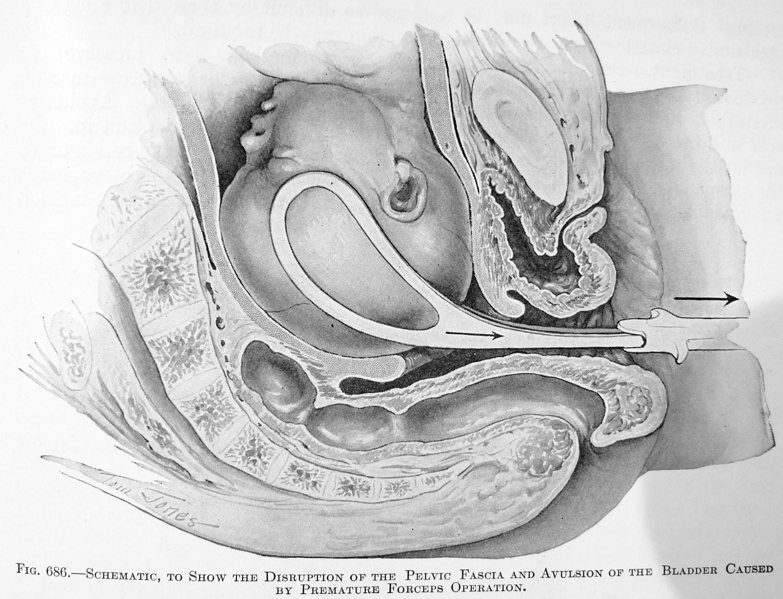
Other common surgical interventions such as episiotomy, forceps and vacuum extraction are strongly associated with pelvic organ dysfunction and maternal incontinence after the birth. These pelvic floor problems are not, as some obstetricians claim, merely collateral damage of normal birth but are the predictable consequence of a failure to make right use of physiological principles, especially spontaneous labor and the right use of gravity. Claims to the contrary are another example of confusing cause and effect.
Despite all the iatrogenic and nosocomial problems associated with the 21st century “obstetrical package”, obstetricians are exceedingly proud to define a 90% intervention rate for healthy women as a better, safer, cheaper and more elegant form of care. But when potentially life-saving obstetrical interventions are applied to healthy women with no life threatening problem (i.e., no pre-existing complication of pregnancy or labor), it introduces unnatural and unnecessary dangers. These intrinsically risky medical and surgical procedures create other complications that increase mortality and birth injuries.
 An example of this detrimental effect would be the “prophylactic” administration of a blood transfusion to everyone before traveling in a car, just in case of a serious automobile accident. Obviously, this expensive, risky and poorly targeted procedure would expose an astronomical number of healthy people to potentially fatal allergic reactions, hepatitis and HIV infections. The great cost to the health care system would divert medical services from the genuinely ill and injured to a healthy cohort that actually does not need or benefit from them.
An example of this detrimental effect would be the “prophylactic” administration of a blood transfusion to everyone before traveling in a car, just in case of a serious automobile accident. Obviously, this expensive, risky and poorly targeted procedure would expose an astronomical number of healthy people to potentially fatal allergic reactions, hepatitis and HIV infections. The great cost to the health care system would divert medical services from the genuinely ill and injured to a healthy cohort that actually does not need or benefit from them.
In an eerie way, Cesarean as the ‘new’ new obstetrics of the 21st century brings the obstetrical profession back full circle to its origins in 1910, when birth as activity accomplished by the mother was first replaced by a surgical procedure in which the mother was simply a passive vessel. Cesarean surgery reduces the 21st century childbearing woman and her whole family to the status of outsiders who have no real decision-making role or legitimate opportunity for active participation.
 For surgical delivery, ‘normal’ is the highly technical process of surgically incising into the uterus in an OR full of obstetrical and neonatal specialists and surgical scrub nurses and extracting the baby, who is then handed off to a perinatalogy team. The mother’s job is to lay still, be passive, let the doctor do his work and be grateful. Except as it relates to her potential to sue the doctor or hospital, she is a non-entity whose personal preference are irrelevant. Just as it was in 1910, the mother is the least important person in the surgical event of her own birth. Again it is the doctor who is the hero in the drama of childbirth. As was true of 20th century obstetrics, 21st Century obstetrics is about obstetricians.
For surgical delivery, ‘normal’ is the highly technical process of surgically incising into the uterus in an OR full of obstetrical and neonatal specialists and surgical scrub nurses and extracting the baby, who is then handed off to a perinatalogy team. The mother’s job is to lay still, be passive, let the doctor do his work and be grateful. Except as it relates to her potential to sue the doctor or hospital, she is a non-entity whose personal preference are irrelevant. Just as it was in 1910, the mother is the least important person in the surgical event of her own birth. Again it is the doctor who is the hero in the drama of childbirth. As was true of 20th century obstetrics, 21st Century obstetrics is about obstetricians.
Chapter 13
Unrealistic Expectations & Lawsuits ~ a vicious cycle for everyone
The poet Ralph Waldo Emerson once wrote: “There is no wall like an idea”. That is also an issue for birth attendants, as people have the idea that high-tech obstetric care can control or eliminate all possible problems, and like a thick brick wall, and no amount of information to the contrary is able to dissuade them.
Since 1910, the obstetrical profession has eagerly promoted the idea that normal birth is a surgical procedure but legally, this is a double-edged sword. It creates the idea of childbirth as an event under total control of the physician-surgeon. The resulting unrealistic expectations makes doctors and hospitals much more vulnerable to litigation whenever there is any problem. First off, it’s not true. As an L& D nurse and midwife, I know the difference between an operation and normal childbirth. I have seen hundreds of babies come out before the obstetrician arrived, but have never once seen anyone’s tonsils or gallbladder take themselves out before the surgeon arrived.
The combination of unrealistic expectations and dashed hopes inevitably results in malpractice litigation. When these statistically predictable complications occurred despite the obstetrician’s best efforts, the heartbroken parents believe they have been wronged by their doctor. Most of the time, this is not the fault of individual obstetricians, but rather a system predicated on erroneous assumptions that marches forward in locked step, promising something that no human can do –control the biology of anther person so as to guarantee zero risk and a hundred percent perfection. This ultimately fuels a vicious cycle of escalating interventions, matched by run-away lawsuits, outrageous malpractice premiums, inflated maternity care costs, dissatisfied customers and thanks to the elective use of unnecessary Cesarean surgery, preventable maternal-infant deaths.
19th century childbirth-as-pathology locks the obstetrical profession out of 21st Century science: Over the last couple of decades, the medical profession as a whole has broadened its base by acknowledging and working with the mind-body continuum. However, the obstetrical profession has never revisited their historical relationship with birth as a pathological aspect of female reproduction. As a result obstetrics focuses more and more tightly on the laboring uterus as a pathological organ, relating to childbirth as if the uterus were a carburetor that needed to be tinkered with, the baby was a spark plug that needed to be removed and the mother’s social and emotional needs were an inconvenient distraction to the real work of the obstetrician.
Despite a daunting list of surgical complications, the Cesarean section rate continues on an unrestrained upward spiral. While the high rate of surgical delivery (31% for 2006) is usually blamed on the large number of older mothers, multiple births and fertility treatments, it turns out that the largest rate of increased in primary Cesarean surgery is for healthy women giving birth to a single baby at the term. [Lisa Miller, CNM, JD; Advanced Fetal Monitoring, Nov 8-9, 2007] The higher the income of the mother and the lighter her skin color, the greater likelihood that her baby will be delivered by Cesarean surgery, so obviously it is not medical factors that are fueling the aggressive use of these obstetrical interventions.
The Cesareans surgery rate in 2006 was 31%. The last year we have economic data for is 2003, during which 1.2 million Cesarean surgeries were performed at a cost of $14.6 billion. As a measure of just how much money $14.6 billion is, it should be noted the economic damage from by the Loma Prieta earthquake in the San Francisco area in1989 was estimated to be only $6 billion and more recently, the US contributed $10 billion dollars to Pakistan since 2001 in an effort to fortify the Pakistani government’s anti-terrorism efforts.
In spite of hemorrhaging money on a system that does not improve outcome, public health officials are predicting a 50% Cesarean rate by the end of the decade. Some hospitals are actually replacing labor rooms with additional operating rooms in anticipation of the dramatic rise in C-sections.
Most inexplicably, there is a move within the obstetrical profession to promote electively scheduled Cesarean for healthy women as the preferred standard of care for the 21st century. Unnecessary Cesarean surgery is the ultimate iatrogenic intervention in normal birth. One recent study from France identified a 3½ times greater maternal mortality rate in electively scheduled Cesareans in healthy women with no history of problems or complications during pregnancy. Another study on the elective or non-medical use of Cesarean surgery documented an increased mortality and morbidity for newborns.
Were Cesareans to become the 21st century standard, it would triple the current rate to 4 million surgical deliveries every year. This would make C-sections six times more frequent that the second most common hospital procedure — the 700,000 upper GI endoscopies done every year to diagnose ulcers and stomach cancer. Cesarean as the new obstetrical standard would put childbirth surgery smack in the middle of our healthcare system, making American medicine more about elective Cesarean surgery than treating people who genuinely need medical services. It would provide yet another opportunity for women and babies to be exposed to hospital-acquired, drug-resistant infections. Already a quarter of all hospitalizations are related to pregnancy and childbirth. An additional 2 1/2 million Cesareans every year would bump this number up quite a bit, as a result of re-admissions for various post-operative complications of mothers and babies.
Pink for girls, Blue for boys and Green for planet-friendly maternity care
Obstetrics for healthy women already has an outsized carbon footprint, especially as it relates to routinely scheduled induction of labor and elective Cesareans surgery. It is a resource-intensive system that requires more than its share of the environmental pie. In particular, million more Cesareans mean more medical schools to train a ballooning numbers of obstetrical surgeons and anesthesiologists. It means more operating rooms, more highly-specialized hospital staff, more nurses, more vehicular traffic, more electricity, more water, longer hospital stays.
Additional surgeries and prolonged hospitalizations mean an increased number of drugs-resistant infections to be added to the thousands of hospital-acquired infection each year and more insoluble antibiotics in human urine which cannot be filtered out and wind up back in our drinking water. It also generates huge quantities of bio-hazardous garbage piling up in land fills. This process of intensive medicalization feeds back on itself, as hospital-based care becomes both cause and effect of nosocomial complications. This translates into the need to build more hospitals, more roads, more traffic and all the other infrastructures that generate more carbon-laden emissions.
Medicalizing normal birth is also responsible for an outsized economic burden — the unproductive cost of unnecessary intervention. This severely hampers our ability to compete in a global economy against other countries that, wisely for them, have not saddled themselves with this albatross. Maternity care policies for healthy women in the vast majority of other countries, both developed and developing, do not routinely medicalize healthy women with normal pregnancies. Many EU countries, Japan and other highly developed countries depend on time-tested methods of physiological management provided by professional midwives and general practice physicians. Obstetrical care is used appropriately whenever there are complications. This small carbon footprint equates to “green maternity care”.
Doing it “Smarter”
Worldwide, the economic drain associated the use of obstetrical interventions on healthy women, particularly the high Cesarean rates, is causing some countries to rethink their national maternity care policy. For example, the C-section rate Britain had crept up to 25% and was still increasing. The UK has historically had a midwife-based system but in the last 20 years, English midwives have been used as labor room nurses. As such, they were carrying out the medicalized procedures of the obstetrical staff, instead of independent professionals providing physiological management. In February 2007, the Ministry of Health in the UK announced the reconfiguring of the National Health Services to reduce the medical costs associated with normal childbirth. During debate in the British House of Commons on July 11th, Prime Minister Gordon Brown noted that by 2009, every healthy childbearing woman in the UK would be able to choose among three options:
- Physiological care by a community midwife in the mother’s home
- Physiological care in a local midwife-led unit based in a hospital or community clinic
- Medicalized care in a hospital, supervised by a consultant obstetrician, for mothers who may need specialist care to deliver safely or may want epidural pain relief [The Guardian, Feb 6, 2007]
This will bring Britain back into alignment with their historical maternity care practices, other EU countries and the entire developing world. The majority of the world is using the cost-effective model of physiological management as their standard of care for healthy women, which is approximately 80% of the childbearing population in most countries.
Safe, Simple & Satisfactory alternatives to Birth as a Surgical Procedure
Aseptic technique is the standard of care used around the world by professional birth attendants who provide physiologically-based maternity care. This protects mothers and babies from infection through a body of knowledge and a variety of effective methods, including hand-washings and universal precautions. In practical application, it means nothing ever touches the mother that has come into contact with any source of contamination – body fluids of others people or sources of ordinary dirt. All materials and supplies that could conceivably come in contact with the mother’s birth canal or the newborn baby are guaranteed to be clean, dry and free of pathogens. Sterile supplies are used anytime an instrument or gloved hand must enter into a sterile body cavity or touch tissues that have been cut or lacerated.
Labor and birth as an aseptic rather than surgical event allows continuity of care, permitting laboring women to be cared for by the same caregiver — physician or professional midwife– through out the process of both labor and birth. It also does not result in the social isolation of the childbearing mother from her family. Under aseptic conditions, the spontaneous vaginal birth of the baby is not considered to be a surgical procedure. No special environment or equipment is required such as a specially-designed bed with obstetrical stirrups. The doctor or midwife does not have to be “gowned and masked” nor does the mother have to lie still on her back or be admonished not to touch anything. The common sense conditions for aseptic technique allow the mother to move about and use physiological positions and the ‘right use of gravity’. Aseptic care does not overshadow the mother’s psychological and social needs. Her family, including other children, can be present when the baby is being born.
The necessary sterile supplies for normal birth are simple — a pair of sterile gloves, a sterile scissor to cut the cord, a sterile umbilical clamp and a sterile towel to make a suitable surface upon which to set these instruments. Accompanying this short list of sterile supplies is the liberal use of clean linens, paper towels, disposable under pads and diapers, sanitary napkins and appropriate trash receptacle.
Aseptic practices do not restrict attendance of normal birth to doctors trained in the surgical specialty of obstetrics and gynecology. It does not require two separate professions providing sequential care – a nurse for labor and a doctor for the birth. It does not disturb the normal process of labor or birth. It prevents nosocomial infection without requiring a surgeon, a surgical environment or billing as a surgical procedure under a surgical code.
The Importance of a Non-Surgical or “Physiological” Billing Code
No effort to reform our national healthcare system can afford to ignore the medicalizing of normal childbirth. No effort to reform this inappropriately medicalized system can afford to ignore the issue of the surgical billing code for normal birth. Presently, there is only one billing code for the entire spectrum of birth-related care and that is a surgical code. Because obstetrics is a surgical specialty, normal childbirth has unfortunately been classified as a surgical procedure for most of the 20th century. A surgical diagnostic category automatically generates a surgical billing code, which produces an entirely different (and expensive) kind of care and a different form of reimbursement.
This surgical designation means the care provided during labor, birth and immediately after the birth, is divided up into billable units and parceled out between multiple service providers. This is the most expensive way possible to pay for maternity care. It eliminates continuity of care and makes the use of physiologically-based practices impractical. Under our current system, non-medical forms of care are so poorly reimbursed that hospitals would quickly find themselves out of business if they did not purposefully increase the number of billable procedures done on each maternity patient.
However, a simple solution is at hand and that is a specific billing code for normal childbirth. To provide continuity of care and to fairly compensate birth attendants, maternity care for a healthy population must allow the physician or midwife to use a non-surgical billing code for physiologically-based childbirth services. A physiological billing code would permit primary birth attendants to be appropriately paid for their full-time presence during active labor as well as the birth and the time and professional responsibility taken for the immediate postpartum and newborn period of care.
