Trapped on the Wrong Side of History ~ Chapter 11 ~ unpublished manuscript
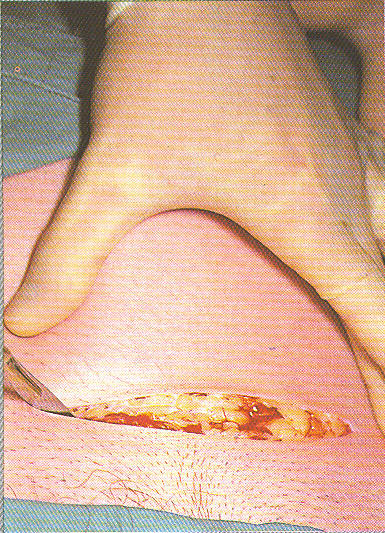
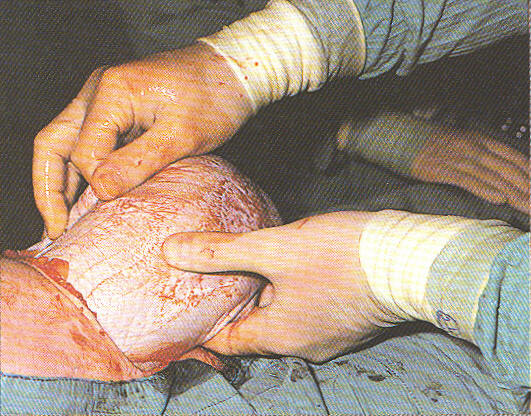
Cesarean surgery ~ The first incision into the skin
The obstetrical profession mistakenly ascribed absolute value to things of relative worth.
This confusion of cause and effect means that inappropriate generalizations are made from a specific situation.
Chapter Eleven
Like the 1970s, 80s, and 90s, the first years of the 21st century were a sequel to the same underlying definition of female reproduction as a pathological process. This meant the same legal and billing code classification of normal birth as a surgical procedure and the obstetrically interventive process with the addition of highly technological electronic fetal monitoring.
All these interventions had become the ‘business as usual” standard, with elective induction and/or scheduled C-sections being used even more often or even earlier in the process.
But the late 20th and early 21st century was most notable for an order-of-magnitude change that equaled in audacity the critical decisions made by Drs DeLee and Williams in the early 1900s. This was (is) a genuine effort within the obstetrical profession to promote the elective or non-medical use of Cesarean as a replacement for normal birth in healthy women. If adopted, this would result in the second most radical change in childbirth practices in the history of planet Earth.
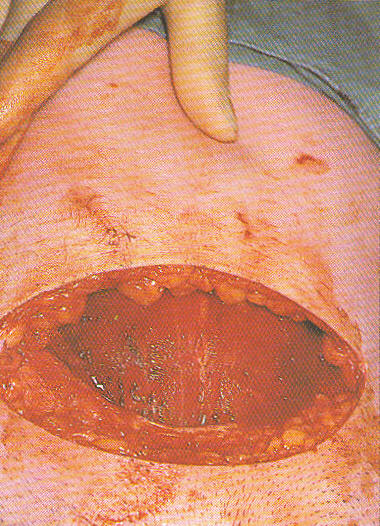
Cesarean Surgery ~ the skin, abdominal fat and peritoneal layers have all been incised and the uterus is now exposed
A lot of thoughtful people are thoroughly convinced that a nice scheduled C-section is the “modern” best choice. In 2000, elective or ‘prophylactic’ Cesarean section for healthy women (often referred to as the ‘maternal choice’ Cesarean) was proposed for the second time, as the new standard for obstetrical care.
Unlike the “Prophylactic Cesarean” paper by Feldman and Friedman, which was published in the prestigious New England Journal of Medicine in 1984, but previously unknown to the public, this time the idea was presented very publicly on Good Morning America.
Dr. Ben Harer, then president of ACOG, was interviewed by Diane Sawyer on GMA. Dr Harer repeated the century-old ideas of DeLee and Williams and others that described vaginal birth as damaging to both mother and baby.
Where Dr. DeLee had proposed the ‘prophylactic’ use of forceps in the early 1900s, Dr Harer proposed an ‘elective’ Cesarean in the early 2000s. According to him, C-section was clearly safer for the baby and “no big difference” risk-wise for the mother.
He and many other obstetricians assumed that most women who have a vaginal birth will need corrective surgery later in their life to repair the damage. With that in mind, the post-operative complications of one, two, or three C-sections were believed to be no more risky for the mother, since cesarean surgery was believed to eliminate pelvic surgery later on.
Here are excerpts from the transcript of the show, taped at a time when the Cesarean rate was significantly lower than it is now:
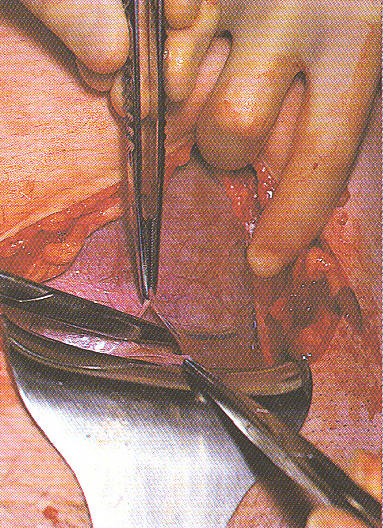
A metal retractor is used to pull the bottom of the incision downward as the surgeon uses a pair of sterile scissors (middle left) to cut into the uterus
Diane Sawyer: “Each year, one in every five** babies in America comes into the world through a cesarean section, the country’s most common surgery.”
**That number has increased to one in three
Diane: “Some obstetricians are now calling the cesarean section preferable to vaginal births.”
Diane Sawyer: “ . . . (doctors) believe that women should at the very least have the option to choose between the two . . . . and that insurance companies should basically pay … equally and treat them equally.”
Dr. Harer: “…Yes …. women should be given the facts and then given the choice.”
Diane: “…and there’s a higher rate of problems with vaginal birth, than with cesarean section?”
Dr. Harer: “Yes, for the baby, the risks are far higher for vaginal delivery . . .than for an elective cesarean section at term.** For the mother, the immediate risks for a cesarean section are a little higher ….
** Both of these statements are wrong — Cesarean surgery is NOT safer for either mother or baby!
Dr. Harer: …. but the longer term, risks of pelvic dysfunction, incontinence . . . . . . those risks are higher for vaginal birth. Over the long term, I think that the risks balance out, that there really is no big difference.” {Note: this statement also is not backed by any scientific evidence}
The uterine wall has been incised and now the amniotic membranes that surround the baby can be seen
The show ended as a charming Diane Sawyer assured the viewers that this ‘obviously’ controversial position would surely occasion additional coverage by GMA, so “stay tuned” for the updates.
Apparently, the idea of Cesarean surgery as the 21st-century standard of care was not at all controversial to viewers, as this topic quickly became a non-story, never to be heard of again on Good Morning America.
Obstetrics ~ 2000 and beyond
“The more things change, the more they stay the same” certainly applies to obstetrics. We think of our lives, our hospitals, and our expectations as dramatically different from the typical overworked and underfed woman having her 6th (or 16th!) baby at the turn of the 20th century.
As a maternity patient in a teaching hospital in 1910, the laboring woman would have been admitted to an open ward full of women, each lying in her bed and laboring under the effects of scopolamine.
Her labor would have been medically managed by nurses, who listened to fetal heart tones every half hour with a fetoscope and routinely administered shots of morphine and scopolamine every 2 or 3 hours per standard Doctor’s Orders. Under the amnesic influence of twilight sleep, our 1910 labor patient would have been restrained in her bed until it was time to be taken by stretcher to the delivery room and put to sleep with general anesthesia.
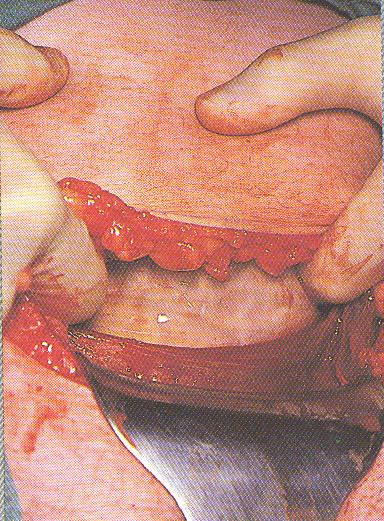
The obstetrical surgeon is extracting the baby’s body from its mother’s uterus
As ‘clinical material’ for medical students, the surgical procedure of vaginal delivery (and all that entailed) would be conducted by a student or intern who was being supervised by an obstetrical professor. After the birth, she would be too groggy to hold the baby for many hours or even know whether she had a boy or a girl.
21st Century Obstetrics — the same level of obstetrical control while using different technologies
Contrast that with the experience that the contemporary laboring woman had. In the year 2000 and beyond, the typical maternity patient would be much less likely to be poor or a ‘grand multipara’ having an umpteenth baby. It would be statistically unlikely for her to be cared for by a medical student or obstetrical resident. Instead, she would be healthy with a normal pregnancy and having a first or second baby, with a private obstetrician in charge of her care.
While being cared for by a “private obstetrician” sounds very appealing, the reality is very different from what most women expect, which is that their doctor will be there in the room with them while they are in labor. However obstetricians are trained as surgeons, which is to say, they aren’t present during the long hours of labor. When a labor patient presents herself to the L&D staff for admission, the nurse calls her doctor, who then legally authorizes the nurse to formally admit the patient and provides directions for how the nurse should manage the patient’s labor.
So the downside of private obstetrical care is that, unlike interns and residents who are consistently present, her doctor will not be physically present in the hospitals until it’s time to come in and ‘deliver’ the baby. Before that, nurses will mainly manage their labor via the telephone while the OB is in absentia, or maybe briefly stop by during his/her normal pre or post-office hours hospital rounds.
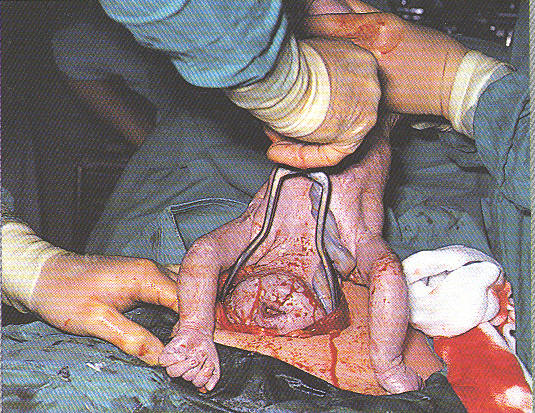
The obstetrical surgeon is using forceps, inserted into the uterine incision, in order to extract the baby’s head from the mother’s uterus
Upon admission to the labor & delivery unit, our 21st-century obstetrical patient would be ushered to a single occupancy LDR. She would not hear other women screaming or cursing, nor would she be ‘prepped’.
She would however be immediately hooked up to continuous electronic fetal monitoring or EFM, to legally record the unborn baby’s status at the time its mother was admitted to the hospital’s L&D unit.
The new labor patient would likely have an IV started, and statistically speaking, Pitocin was added to be sure that her labor progressed at a predictable rate.
She will also be hooked up to a bedside electronic fetal monitor (EFM) to detect possible fetal distress caused by an overreaction to the Pitocin. This is so the staff can do a timely emergency C-section if the situation gets out of hand.
When the labor contractions got more painful, an epidural would replace the narcotics and scopolamine drugs previously given in labor as the standard treatment from 1910 to as late as the 1980s in the Deep South and very small hospitals anywhere in the country. Being in labor in the 21st century will also save her from the indignity of a hood put over her head, four-point restraints and literally ‘losing her mind’ for the many hours of her labor.
Once the epidural catheter was in her back, she would need to have her blood pressure very closely monitored, so an automatic BP cuff would be placed on her arm.
Since she couldn’t feel the lower half of her body, she wouldn’t be able to void on her own so a Foley catheter would be placed in her bladder and hooked up to a bag to collect the urine. In most hospitals, the catheter is left in place until after the baby is born (saves time if a crash CS should have to be done), but this also means that she will push during the second stage with the 30cc Foley balloon in her bladder (a fluid-filled ball approximately the size of a walnut). With every expulsive contraction, the Foley balloon also being pushed down into the upper end of her urethra, stretching the soft tissue and perhaps over-stretching the urinary sphincter.
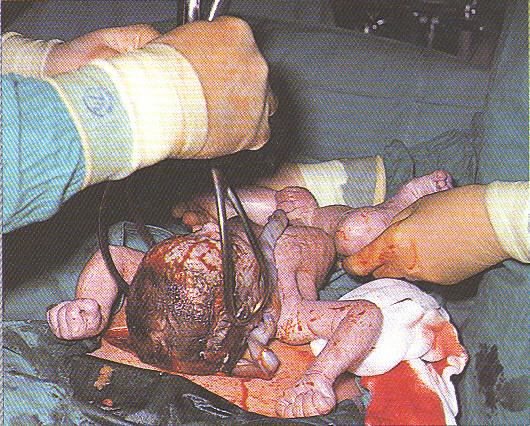
The surgeon removes the forceps as the baby is momentarily laid on his mother’s abdomen. This photo clearly demonstrates the reality of how incredibly invasive Cesarean surgery is for both mother and baby, dispelling Dr. Harer’s claim that “there’s no big difference” between a normal vaginal birth and a C-section. It’s like telling someone there is “no big difference” between taking the chair lift up to the top of the trail when skying versus slugging up the mountainside in boots that have 20-pound weights in them!
Opinions differ as to whether leaving the Foley in during pushing increases the incontinence rate after childbirth, but some hospitals take it out as soon as the mother starts pushing, based on the idea that it is not a good technique, as pushing the walnut-sized ballon into her urethra each time the mother has a contraction might stretch it out and lead to incontinence.
This issue particularly applies to women who had a Cesarean after many hours of futile pushing in the second stage.
When it was time for the baby to be born, the obstetrician would be called at home or his or her office. When the doctor arrived, the 21st-century mother would no longer be separated from her family by being trundled away on a stretcher to the delivery room. Instead, the delivery room would be brought to her in a form of a bed that turned into a delivery table with stirrups and cupboards that opened up to provide state-of-the-art delivery room equipment and supplies.
The epidural she already had would take the place of the general anesthesia that used to be given in preparation for surgical delivery. This would spare both her and her baby from the dangers of anesthetic gases and allow her husband to stay by her side during the ‘procedure’ of vaginal birth. She would be permitted to hold her baby soon after its birth since she wasn’t under the influence of consciousness altering anesthetics.
According to interviews conducted in 2002 & 2006 of healthy childbearing women who had recently given birth under obstetrical management:
93% reported continuous electronic fetal monitoring during their labor
86% were given IVs (and prohibited from drinking or eating)
74% of women required to give birth lying on their back,
71% immobilized / confined to bed / not permitted to walk during labor
67% rate of artificial rupture of membranes,
63% of labors induced or accelerated with prostaglandins and/or Pitocin
63% epidural anesthesia rate
58% had a gloved hand inserted into their uterus after birth
52% catheterizations / indwelling bladder catheter,
35% episiotomy rate, 30% cesarean surgery,
13% instrumental delivery by forceps or vacuum extraction.
[Listening to Mothers Survey, 2004 & 2006 @ www.childbirthconnection.org]
It should be noted that these statistics apply to healthy women with normal pregnancies. The operative rate for the healthy portion of our childbearing population is more than 70% (aggregated rate of 35% episiotomies, 30% Cesarean section rate & 13% forceps /vacuum extraction). Added to this already dismal list of disruptions in biological processes is the increasingly accepted notion of scheduling elective Cesareans for healthy women before they have a chance to go into labor. If anyone wonders why this is so, the answer lies in the ‘new’ obstetrics and the crucial decision made by DeLee and Williams.
Having defined obstetrics as a hybrid surgical specialty (combined with gynecology) in the late 1800s, obstetrical residents have been taught ever since to conduct normal birth as a surgical procedure. This surgical designation is the reason physiological management is not taught in medical school, why labor and delivery units are a restricted area, why doctors wear OR scrub clothes, suit up for delivery with a sterile, long-sleeved doctor’s gown, and wear a surgical cap and mask. Vaginal birth as a surgical procedure has to be under the tight control of professionals.
As a ‘procedure,’ it is something the doctor does, instead of the mother, and is why we say “the doctor delivered the baby”, instead of saying “the mother gave birth”. It is also the reason that normal birth has a surgical billing code and a correspondingly hefty price tag.
As a highly medicalized process, care for childbirth had already been moved out of the main steam of normal life and reconfigured to fit the protocols for an appropriate surgical environment. The social and emotional needs of the mother and the father and the historically social nature of childbirth all have to be subsumed to the needs of institutional for ensure ‘sterility’. Like life during Covid, it meant that family members were not allowed to be present.
The primary focus became the technical details of maintaining their sterile technique, which neither add to the safety of the childbearing women or allows the birth attendant to directly address what are the real needs of spontaneous biology (right use of gravity) or the mother’s own physical and psychological experience.
As a result, the mother and the father were both psychically erased from the picture for the first seventy-five years of the 20th century. While hospitals no longer bar the father or other family members from a vaginal delivery in the LDR, when childbirth becomes Cesarean surgery, everyone but the father is excluded and he quickly becomes an outsider that must depend on the good graces of the anesthesiologist for permission to remain with his wife. The dad’s participation and conduct in the OR suite are tightly controlled and in cases instances of urgency, he can be barred completely.
But the most detrimental of all is the systemized loss of physiologically-based birth services and its replacement by the inappropriate idea of normal birth as a surgical procedure. The purposeful non-teaching of normal physiology in medical school, combined with the unwarranted use of interventionist obstetrics, wreaks havoc on the biology of childbirth.
The surgical delivery of healthy women as an American custom has not and will not improve outcomes and actually is associated with an increase in maternal mortality. Countries that rely on simple low-tech techniques of physiologic childbirth practices do much better than the US.
In fact, all we have gotten out of birth as a surgical procedure is a surgical billing code for a normal biological event, disproportionate expense, and huge piles of bio-hazardous waste, topped off by those all-to-familiar pictures of the mother-to-be lying on her back under sterile sheets with her legs in stirrups while her doctor suited up like the Michelin Man, peering over his surgical mask at her. This did not buy us better babies and so far we have no reason to believe that scheduled C-sections would do any better and lots of evidence that it ups the danger.
Standardization versus Customization of care during labor and birth
The 20th-century industrialization of normal birth was a process for standardizing care, an attempt to make it more efficient in a manner not far removed from the industrialization of manufacturing and other process-related businesses.
But the biology of childbirth, and the physical, social, and psychological needs of the mother-to-be cannot be deconstructed and dealt with like objects on a conveyor belt that will be assembled farther down the line. The individual needs that each childbearing woman presents to her caregiver are unique and change minute by minute. They require the moment-by-moment attention of the caregiver, which requires the physical presence of the childbirth attendant throughout active labor and birth. As in piloting a plane, the pilot or co-pilot has to be there and be engaged on a moment by moment basis. What laboring women need is not standardization but customization.
The reasons that physiological management – a process of customization — was displaced are legion. The most central one is the simple fact that physiological management is held in distain and not taught in medical school. It was considered to be ‘woman’s work’, as can be seen by assigning the long hours and of supportive care during labor to nurses and low-paid ancillary staff and the exciting, well-compensated photo finish to physicians. In the absence of physiologically-based methods, a number of policies, procedures, and medical devices must inevitably be called upon to take the place of these classically non-interventive methods.
The list is lengthy but a few rise to the top in terms of their negative effect – EFM, induction or augmentation of labor with Cytotec and Pitocin, epidural, anti-gravitational positions and coached pushing, episiotomy, vacuum extraction, liberal use of Cesarean as a strategy to prevent cerebral palsy in babies and/or pelvic floor damage in mothers and the idea of “maternal choice’ Cesareans as the 21st standard of care. The word usually used to indicate the process for using all this ‘stuff’ is the ‘cascade of interventions’.
The Cascade of Intervention:
The obstetrical profession has never acknowledged the domino effect, also called the cascade of interventions, associated with highly medicalized childbirth. This cascade occurs when an obstetrical procedure — for example, induction of labor — triggers the need for other interventions, such as continuous EFM and epidural anesthesia.
The cascade of interventions can so disturb the biological process that it results in iatrogenic-induced fetal distress that requires a variety of emergency interventions, including Cesarean section. This inherently complex chain of events and the large number of problems encountered during the labor and vaginal birth, make Cesarean surgery look a problem solving strategy, especially if the large number of lawsuits associated with vaginal birth were factored in.
Can continuous Electronic Fetal Monitoring and Cesarean eliminate Cerebral Palsy? — the obstetrical profession’s own research says “No”
Since 1975 there has been a 6-fold increase in the routine use of electronic fetal monitoring (EFM) on low-risk mothers. The obstetrical profession hoped to eliminate cerebral palsy and other neurological complications through the expanded use of EFM, combined with the liberal use of cesarean section whenever the fetal monitor strip indicated a possible problem. EFM is the most frequently used medical procedure in the US – 93% of all childbearing women are continuously hooked up to this equipment during labor. Many health insurance carriers reimburse hospitals $400 an hour for continuous electronic monitoring in labor.
However, the consensus of the scientific literature has never supported the routine use EFM. One recent study noted that the ability of continuous EFM to detect potential cases of cerebral palsy during labor is only 00.2%, not because the electronics of the equipment are flawed but because the premise is incorrect. In spite of these faulty assumptions, the universal use of EFM on low-risk women continues unabated and has resulted in a skyrocketing Cesareans section rate that was not associated with better outcomes.
In 2003, 1.2 million Cesarean surgeries were performed in the US (27.5% cesarean rate) at a cost of $14.6 billion. Our current Cesarean rate is over 31% and climbing. The public and the press never seem to question the unlikely idea that normal childbirth is somehow made safer and better by turning it into an expensive and risky surgical operation as documented in the above series of intraoperative photos.
Yet the obstetrical policy of ‘pre-emptive strike’ has not made the tiniest bit of difference in the incidence of CP and similar neurological conditions. This verifiable fact is now gratefully used in court to defend obstetricians facing litigation.
@@@
Use this link to continue reading –> @@@ Link to Chapter 12
