1700 words

The Big Blue Elephant in the Room: the hospital economics of c-EFM and the unproductive expenses billed to health insurance carriers and the federal Medicaid program
The question here is pretty simple: Are state, county and federal governments, other 3rd party payers (insurance companies) and those who must pay out-of-pocket are getting an appropriate bang for their buck?
Are we getting the ‘value-added’ we are all paying for from our current configuration of a technology-centric, one-size-fits-all model of obstetrics that doesn’t distinguish between high-risk and low-risk situations?
This system turns the cost-effective contribution for added value on its head, since the more we pay, the more we lose. Society is being asked to pay for a safety service that makes childbirth more dangerous for healthy women.
Based on a consensus of the scientific literature over the last 5 decades, the answer is a resounding “no” — c-EFM is value lost and should be immediately curtailed.
How did this craziness happen?

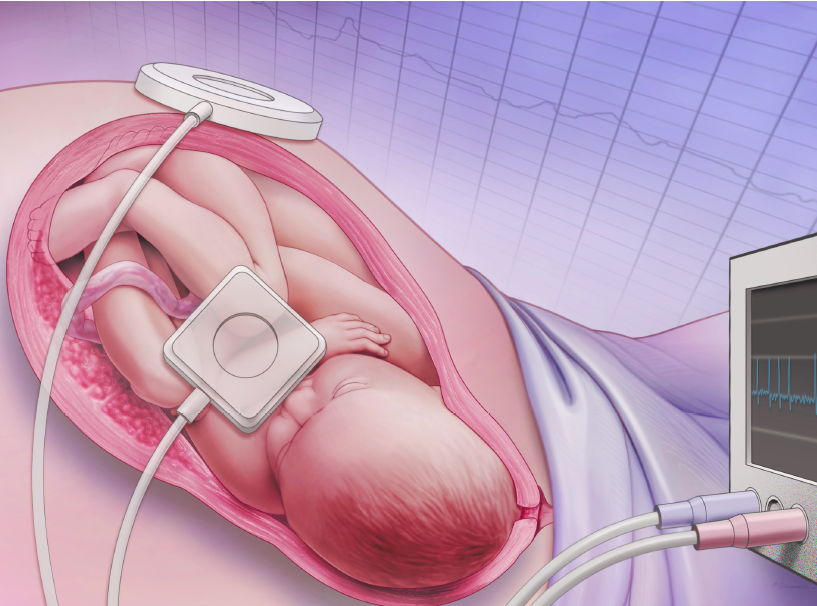
A healthy laboring woman two c-EFM belts wrapped around her pregnant belly that lead to the EFM machine at the bedside, an automatic blood pressure cuff hooked to a different monitoring machine and a pulse oximetry device on the index finer of her left hand.
This drift away from obstetrical care as a value-added services for women with high-risk conditions began in the mid-1970s.
That’s when the obstetrical policies and practices that were so effectively used on women with high-risk pregnancies gradually began to be used as the new standard of care for healthy women with normal low-risk pregnancies.
Even more disturbing is the unambiguous cause-and-effect relationship btw the use of continuous EFM and a statistically significant increase in the rate of unplanned Cesarean surgeries and its many complications. [1, 2]
During the 5 decades-plus between 1970 and 2016, the Cesarean rate in the U.S. increased from 5% to 32%. During this same period, the use of c-EFM when from zero to 90%.
In the U.S, the 2nd most common reason for first-time Cesareans is “non-reassuring fetal heart tones” (ACOG 2017, #184)
It must be noted that the adoption of c-EFM, which began as a gradual trend, was turned into a avalanche by the malpractice crisis of 1970s.
The Failure of c-EFM as a screen tool designed to improve maternal-infant health
A commentary in the Journal of Obstetrics & Gynecology, (Grimes and Peipert, 2010) makes the case that that EFM was adopted as a public health screening program without meeting important criteria for what make an effective screening test.
To be valid a screening tool, the test or process must be able to tell the difference between people with a real problem and those without. A poor screening tool for a rare outcome would not be considered ethical if it causes healthy people to think they are sick, leads to unnecessary medical tests and procedures with harmful side-effects, and wastes money and other resources.
This is the ethical concern with routinely using of continuous EFM, which is documented false-positive rate of 99.8% for detecting fetal complications, to screen healthy laboring women with low-risk pregnancies.
The type of problem that EFM does have an established track record for detecting — 2 out of a thousand — is trying to find an incredibly rare problem by exposing a very large demographic (over 70% of the 4 million annul births in US) to all the various risks of continuous EFM.
This starts at the most simple level with unnecessarily immobilizing 3-plus million women in their labor beds, which increases the need for Pitocin to keeps the labor progressing, and the need for epidural anesthesia because the laying still in bed hour after hour while in active labor is too painful to tolerate.
Last but not least is the going on to the cascades of complications associated with increase level of operative vaginal deliveries and Cesarean surgeries.
There are all evidence-based reason for not routinely using of continuous EFM to continually screen healthy, low-risk laboring women for fetal complications,
Plain Facts, Plain Talk
The facts are indisputable: Our current obstetrical system treats all healthy women with normal pregnancies as if they were high-risk without improving perinatal outcomes. In addition to not getting the promised “bang for one’s buck“, routine electronic fetal monitoring increases maternal mortality and morbidity due to the great number of unplanned surgical deliveries associated with c-EFM, and complications that accompany major abdominal surgery.
These facts are not a secret that the obstetrical profession doesn’t know anything about. There are literally hundreds of peer-reviewed professional papers published since 1975 documenting continuous EFM’s lack of efficiency.
An highly respected but older obstetrical textbook (Davis Obstetrics, 1966) specifically charges obstetricians with a duty to keep up with the facts of their profession:
“It is the duty of every obstetrician to know what can be known”
As for how many opportunities there are for the obstetrical profession “to know what is known” about the routine use of c-EFM on low-risk labor patients, one only has to read the many studies published on c-EFM.
The first 22 pages of my Google query “clinical trials of electronic fetal monitoring” provided an average of 11 links per page or 242 studies and clinical trial on c-EFM. I stopped downloading at that point.
Many of these titles point out that assumptions by the obstetrical profession about the efficacy of the EFM don’t match the scientific evidence.
One example in which the title tells it all is a study titled: “Electronic fetal monitoring, cerebral palsy, & caesarean section: Assumptions vs Evidence. BMJ. 2016;355:i6405.”
Some studies found that the continuous EFM group were more than twice as likely (63%) to have a Cesarean surgery and 15% more likely to experience the use of vacuum or forceps compared to those in the auscultation or “hands-on” listening group.
A paper written by an obstetrician for other obstetricians begins with this startling statistics:
“Intrapartum fetal heart rate monitoring is the most common obstetric procedure performed in the United States.
- Despite the widespread use of EFM, there has been no decrease in cerebral palsy.
- … meta-analysis of randomized control trials has shown that EFM has no effect in perinatal mortality or pediatric neurologic morbidity.2
- However, EFM is associated with an increase in the rate of operative vaginal and cesarean deliveries.1”
Although intermittent fetal auscultation {IA} may be a theoretical option in low-risk patients, nursing staffing limitations makes this impractical … ”
{Fetal Heart Rate Monitoring Update; The Female Patient, April 2011}
Another study noted that only 0.2% (that’s only two out of a thousand) cases of cerebral palsy were able to be detected during labor by continuous EFM.
In their 2009 practice bulletin, ACOG concludes that there is Level A evidence (based on good and consistent scientific evidence) that the false-positive rate of EFM for predicting cerebral palsy is greater than 99%.
Other researchers have found that continuous electronic fetal monitoring is a very poor test for detecting potential cerebral palsy, with a false positive prediction rate as high as 99.8% [EvidenceBasedBirth.com]
The response by EFM equipment manufactures to this sobering information has been to churn out various “improvements” on the existing crop of monitors, and amp up their R&D (Research & Development) for a host of new, but equally, or even more complicated monitoring devices.
Unfortunately, none of these 2nd, 3rd and 4th generation EFM upgrades and add-on have been able to fix the central ‘problem’ with electronic monitoring — interventions that reliably improve outcomes for very high-risk patients predictably make matters worse for healthy women with normal pregnancies.
Since the federal MediCaid program reimburses doctors and hospitals for approximately 49% of all maternity care services in the US, its appropriate to mention that under Title 33 U.S. Code § 931 (Penalty for misrepresentation) anyone who “knowingly and willfully makes a false statement or representation for the purpose of obtaining a benefit or payment under this chapter shall be guilty of a felony“.
 We must remember that the science-based method for monitoring the well-being of a fetus during labor is to regularly listen to the rate and rhythm of the fetal heart with a fetoscope or hand-held Doppler.**
We must remember that the science-based method for monitoring the well-being of a fetus during labor is to regularly listen to the rate and rhythm of the fetal heart with a fetoscope or hand-held Doppler.**
** Link to information of the principles, techniques and skills of auscultation
C-EFM, Product Liability Law & A Duty to Warn
Keeping in mind the federal “Penalty for Misrepresentation” (Title 33 U.S. Code § 931, we believe product liability law in the United States creates a Duty to Warn for all manufacturers and distributors of continuous EFM equipment.
This means that those who profit from the sale of continuous EFM equipment must include a product disclaimer.
This manufacturer’s disclaimer must report the established limitation of c-EFM as documented in the many clinical trials and other studies conducted over the last 50 years on the efficacy of EFM as compared to the control — i.e. auscultation.
Furthermore, it must warn physicians and obstetrical providers that use of their product is associated with a statistically significant increase in operative deliveries and Cesarean surgery and associated increase in maternal mortality.
Again and again, studies and prospective clinical trials on the efficacy of c-EFM found no benefit for heathy women with normal pregnancies while establishing an unambiguous cause-and-effect relationship btw the use of continuous EFM and a statistically significant increase in the rate of unplanned Cesarean surgeries and its many complications. [1, 2]
Based on the preponderance of scientific evidence, this “Duty to Warn” must include the following information:
- As defined by a reduction in the rate of CP and other neonatal encephalopathies, studies that compared the routine use of periodic auscultation with c-EFM consistently determined that healthy laboring women with normal term pregnancies did NOT benefit from c-EFM
- The intrapartum (during labor) use of c-EFM in this same category of low-risk women with normal pregnancies has been proven to significantly increase unplanned Cesareans deliveries and associated complications
- A list of the known complications of Cesarean surgery include (but are not restricted to):
-
- 13-fold increase in peri-partum emergency hysterectomies
- 6% rate of secondary infertility
In addition, the manufacture’s Duty to Warn relative to known complications of Cesarean surgery must include the well-documented facts about about abnormal placental implantation, a potentially fatal, but unfortunately frequent complication in post-Cesarean pregnancies.
This includes (but is not restricted to) the following:
-
- Cesarean hysterectomy
- placenta accreta, increta, and percreta
- 7% to 10% maternal mortality rate for post-Cesarean mothers women with a placenta percreta
 Continued ~ Part 2
Continued ~ Part 2
How did things go so far in the wrong direction?
Before addressing that key question, it will be helpful to step back and look at the big picture from an historical perspective.
Chapter 2 is devoted to doing just that.
