
A specially-designed placenta-percreta operating suite outfitted with the latest interventional radiological equipment for performing Cesarean-hysterectomy on previous C-section mothers. In addition to multi-million dollar equipment, there are over 20 doctors, OR nurses, neonatal nurses and specialty hospital staff.
~ 2B ~ Cesarean Surgery – the “gift” that keeps on giving!
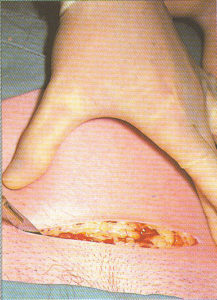
Cesarean surgery: #1 scalpel incision into the skin
Cesarean surgery is the gift that keeps on giving, not only at the time the operation is performed but in all future pregnancies. Unfortunately for 6% of post-cesarean mothers, a downstream complication of their Cesarean surgery is infertility, usually a result of post-operative infections.
Life-threatening complications of this surgery can result in the need for blood transfusions, unplanned emergency hysterectomy for uncontrollable hemorrhage and days or even weeks in the ICU.
The postpartum recovery period is longer, harder, more painful and in some cases of prolonged post-op pain, exposes new breastfeeding mothers to opioid addiction as a result of the needed narcotic medication. In other instances, the problem is post-operative infections that have to be treated with IV antibiotics and may require new mothers to be readmitted to the hospital.
Obviously, none of this is conducive to bonding with one’s new newborn or learning how to care for and meet its needs, something that may be a make-it-or-break-it issue for post-op mothers trying to breastfeed for the first time.
Cesarean surgery: The skin incision is extend down thru the subcutaneous abdominal layer of fat
Then there is the long shadow that a previous C-section casts over all subsequent pregnancies. This begins with the risks of possible uterine rupture of the Cesarean scar either before or during labor. That is the primary source of controversy over vaginal birth after Cesarean (VBAC), as many doctors, hospitals and medical malpractice insurers do not want to risk being sued in these cases. As a result, they either decide not to “do” VBACs, or hospital policies (often based on liability insurance contracts) won’t allow them to do so.
This sets up previous-Cesarean mothers for additional, often unwanted (and certainly not medically necessary) major surgeries by requiring that all future babies be delivered by repeat C-section. This exposes her to all the aforementioned risks, over and over again, and dramatically increases the likelihood of the placenta-related complications described below.
The most devastating and potentially deadly of the many delayed and downstream complications of Cesarean surgery is the propensity to develop abnormal placental implantation in future pregnancies, a risk that increases exponentially with each subsequent Cesarean delivery.
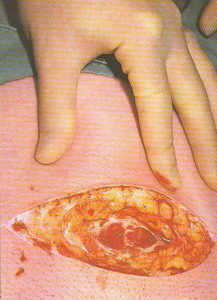
Cesarean Surgery: The peritoneum (tissue covering all abdominal organs) is surgically exposed
Even the very best of circumstances — the least invasive category of placenta accreta — can be life-threatening. Luckily. the majority of these new mothers come through without requiring blood transfusions, major surgery, or admission to the ICU.
But when the placenta grows into the uterine muscle (placenta increta), or worse yet, grows completely through the wall of the uterus (percreta) and attaches itself to other abdominal organs (usually bladder or bowel), it requires a highly risky preterm Cesarean-hysterectomy. This dire but mostly preventable emergency is fatal 7-10% of the time.
Unfortunately, the delayed and downstream complications associated with Cesarean surgery make any policies or practices that increased the C-section rate counterproductive in the extreme.
Vocabulary Review for types and levels of abnormal Placental attachments:
- Placenta Previa is when the placenta implants at the bottom of the uterus. Depending on how close to the cervix, there are 4 levels of previa: (a) low-implantation (b) marginal (c) partial and (d) complete, which covers the cervix completely and makes vaginal birth impossible.
In addition to the previa, the placenta may also grow abnormally deep into the uterus, which means the mother-to-be has both a previa and a perceta. - The most serious levels of previa (c & d) or any level of accreta-percretarequire Cesarean delivery.
- Placenta accreta is when the placenta grows abnormally into the superficial lining of the uterus and is the least serious level of invasion
- Placenta increta is when it grows into the uterine muscle
- Placenta Percreta is when it grows through the uterine wall and attachesto other abdominal organs.These are life-threatening complications that frequently require an emergency hysterectomy to stop the bleeding and has a 7 to 10% maternal mortality rate.
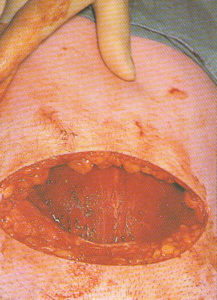
Cesarean surgery: The peritoneum has been surgically excised (cut and pushed aside) to expose the lower part of the mother’s uterus
What is the word for promising one thing & doing the exact opposite?
Now we come to the well-documented facts about the current national standard for obstetrical care in the US, which is organized around the universal use of c-EFM. There is no question that the frequent use of emergent C-section based on EFM tracings that are ‘non-reassuring’ increases our national Cesarean rate. In fact, “non-reassuring fetal heart tones” is the second most frequent diagnosis for Cesareans performed on first-time mothers.
Yet the raison d’etre for EFM — reducing the instance of cerebral palsy and other neurological disabilities — is NOT happening. What surely is happening is a decades-long medically-unnecessary increase in Cesarean surgery and its many intra-operative, post-op, delayed and downstream complications that remains an everyday reality for the four million laboring women (3.5 million of whom are healthy and have normal pregnancies).
These women will find themselves immobilized in their labor beds while they remain hooked up to continuous electronic monitoring equipment. This is almost always followed by a cascade of obstetrical interventions — IVs and epidurals for pain, automatic blood pressure cuff, pulse oximeter, foley catheter and far too often, the need for vacuum extraction or Cesarean delivery.
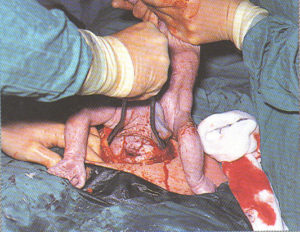
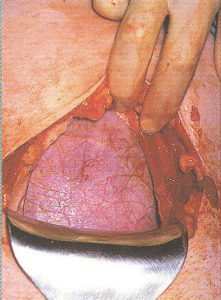
Cesarean surgery: After a four inch incision into the lower part of the uterus, the head of this breech baby is delivered by forceps (yes, you can have a C-section AND a forceps deliver both)
As if this is not problem enough, this “standard care ” predictably doubles or triples the cost of normal childbirth.
How could such a discordant practice have been perpetuated for the last 50-plus years? How come no one else had noticed?
Hospitals economics & the Nancy Reagan “Just Say No” policy
The professional journal publications quoted in this post and many other peer-reviewed articles clearly convey the obvious — the routine use of continuous EFM on low and moderate risk women is NOT a science-based practice AND has never been able to do what was advertised– eliminate or greatly reduce the rate of CP and other neurological pathologies of the newborn.
Nonetheless, the obstetrical profession and hospitals have masterfully ignored everything they don’t want to hear, decade after decade after decade, as they swept new studies under the rug to join all the earlier studies– something not to be talked about, and certainly not to be acted on!
 In spite of the many complications associated with the universal EFM for healthy women with normal pregnancies, and well-established fact that c-EFM is not associated with better outcomes, the practice continues unabated in the 3,400 hospitals in the U.S. that provide obstetrical services.
In spite of the many complications associated with the universal EFM for healthy women with normal pregnancies, and well-established fact that c-EFM is not associated with better outcomes, the practice continues unabated in the 3,400 hospitals in the U.S. that provide obstetrical services.
EFM is now the single most frequently used medical procedure in the US, which is to say that the use a $15,000 electronic monitor system has outstripped every other medical device or procedure in America.
The official estimate is that 85 to 93 % of all childbearing women are hooked up to continuous EFM equipment during their entire labor. [citation L2M Survey 2002 & 2005; Martin et al 2003]
Many health insurance carriers reimburse hospitals $400 an hour for intrapartum continuous electronic monitoring. According to doctors and hospitals, this is the cheapest and best way to protect them from multi-million dollar malpractice suit for a damaged baby, and like one’s American Express card, you shouldn’t go anywhere without it!
The April 2011 article quoted in Part 1 acknowledges the lack of a scientific basis for c-EFM, but at the same time, they went on to say some version of:
“ya, but we have to keep using universal EFM because there are too fewnurses to use IA”
This means that hospitals in the US have systematically chosen NOT to hire enough L&D nurses to use the ‘alternative’ to EFM — a simpler but equally-effective monitoring method of known as Intermittent auscultation (IA). {full explanation and description of how it works follows in Part 3}
 As noted, many hospitals bill health insurance companies and the federal Medicaid program up to $400 an hour for each labor patient who is hooked up to c-EFM. Each hospital is reimbursed many thousands of dollars for average labor (8-10 hrs = $3200-$4,000), multiplied by 3 to 12 labor patients in the unit at any one time (i.e. generating from $10,000 to $40,000 per shift).
As noted, many hospitals bill health insurance companies and the federal Medicaid program up to $400 an hour for each labor patient who is hooked up to c-EFM. Each hospital is reimbursed many thousands of dollars for average labor (8-10 hrs = $3200-$4,000), multiplied by 3 to 12 labor patients in the unit at any one time (i.e. generating from $10,000 to $40,000 per shift).
L&D nurses certainly are NOT getting paid $400 an hour (average RN pay in the US is btw $28 and $45 an hr). Obviously, hospitals in the US find it a whole lot more profitable NOT to hire enough L&D nurses to monitor (i.e. the active verb, not the machine!) the unborn baby using a hand-held Doppler and Intermittent Auscultation (IA) protocols.
While “auscultation” is a strange and hard-to-pronounce word, IA itself is a simple and straightforward screening process that collects essentially the same 4-points of information on the fetal heart rate and rhythm as EFM to determine the health status of the fetus at each specific point in time as either ‘reassuring’ or ‘NOT reassuring’. The use of low-level technologies similar to IA that are regularly used during labor includes a blood pressure cuff and thermometer to repeatedly check on the well-being of the mother.
In the case of intermittent auscultation of an unborn baby, the birth attendants or nursing staff are listening for four data point listed below and will use them, just as they would information about the mother’s BP or temp, to determine if everything is normal or if there is a problem that needs to be medically evaluated. These four data points for fetal well-being are:
- normal baseline (y/n)
- normal variability (y/n)
- the presence of reassuring Accelerations (y/n)
- the absence of pathological Decelerations (y/n)
 This screening process is repeated many times during labor, usually every 30 minutes during the 1st stage and every 15 minutes or more often during the 2nd (pushing) stage.
This screening process is repeated many times during labor, usually every 30 minutes during the 1st stage and every 15 minutes or more often during the 2nd (pushing) stage.
Whether this data is gathered by EFM or IA, the ‘screening’ process uses the same binary data (yes/no) of four specific markers that provide a clinical picture of normal vs not normal. This tells the primary birth attendant (OB or midwife) and/or L&D staff whether an additional evaluation is indicated or if emergent interventions is necessary.
These four points of information as provided by IA on fetal wellbeing allows the unborn baby to be monitored without the many complications, expense, increase C-section rate and maternal mortality associated with c-EFM.
The dilemma that c-EFM poses to obstetricians are humorously described in this brief tongue-in-cheek editorial by Dr. Drosman to his fellow obstetricians.
 Why the C-section rate is rising by Dr. Steven Drosman, MD, obstetrician-gynecologist in San Diego, CA; Editorial ~ Medical Economics, Oct 2000 ~
Why the C-section rate is rising by Dr. Steven Drosman, MD, obstetrician-gynecologist in San Diego, CA; Editorial ~ Medical Economics, Oct 2000 ~
“Probably the biggest C-section motivator, however, is fear of a lawsuit. The rationale is simple: At worst, you’ll be criticized for performing a C-section but you can be roasted for delaying one!
When a patient is hooked up to a fetal monitor, it initiates an unholy trinity — the anxious patient, the hovering nurse, and the paranoid physician. The tension escalates as monitoring devices are added: the fetal scalp electrode, the fetal pulse oximeter, and intrauterine pressure catheter. Add some more Pitocin to the mix, and the action begins.
The labor and delivery nurse watches the monitor and observes decreased variability and persistent late decelerations. The obstetrician is notified, wipes the perspiration from his forehead and pops a handful of antacids.
The patient and her family are informed of the potential crisis, and the can of worms has been opened. More likely than not this “electronically compromised” fetus will be delivered by emergency C-section, with perfect Apgar scores.
Continue to Part 3A
 The failure of routine EFM to prevent Cerebral Palsy in babies or to protect OBs & Hospitals from lawsuits
The failure of routine EFM to prevent Cerebral Palsy in babies or to protect OBs & Hospitals from lawsuits
Reference
1. The Permanente Journal
