Part 3A ~ 2019 Easy shortcut to share –> http://tinyurl.com/y65wzon5 word count 2,400
How did the extreme discordance btw the scientific studies and current obstetrical standard of care come about?
Unfortunately, the answer is “follow the money”, or i should say, follow the three biggest economic areas.
Two obviously positive revenue streams: the manufactures who sell EFM machines, software, and central monitoring system, and hospitals which sell the service of continuous EMF, being reimbursed several hundred dollars each hour for each woman in labor by insurance companies and the federal MediCaid program (49% of US births are reimbursed by MediCaid).
The last aspect of ‘following the money’ leads us to the malpractice issue. In regard to EFM, the economics of professional liability insurance are two-fold. First, manufacturers benefit enormously from the popular idea (often wrong) that using EFM is equivalent of “insurance” against lawsuits — buy and use our EFM machines and you (or your institution) will save a ton of money by not getting sued!
The second part of the money stream is the income it generates for professional liability carriers. Many obstetricians pay $150,000 in annual premiums. Companies, who obviously hope to get everyone business, sometimes offer the equivalent of a ‘good driver discount’ — that is, agree to reduce the annual premium if the OB follows all the policies of their hospitals and also agrees not to provide any planed vaginal birth services to mothers who previous had a Cesarean or who had a twin pregnancy or baby in a breech position.

A quick history of fetal monitoring: Intermittent Auscultation & EFM ~ verbs, nouns, and names of physician-inventors
 The first person to report hearing the sound of an unborn baby’s heartbeat was a 17th century physician by the name of Dr. Marsac. A contemporary of his, a Dr. Killian, was the first to ponder the possibility that the rate and rhythm of the fetal heart might be an indicator of how well the fetus was (or wasn’t) tolerating the process of childbirth.
The first person to report hearing the sound of an unborn baby’s heartbeat was a 17th century physician by the name of Dr. Marsac. A contemporary of his, a Dr. Killian, was the first to ponder the possibility that the rate and rhythm of the fetal heart might be an indicator of how well the fetus was (or wasn’t) tolerating the process of childbirth.
However, this possibility went unnoticed for two more centuries, until 1818, when doctors Mayor and Kergaradec described a method of auscultating fetal heart sounds by placing one’s ear on or very near the maternal abdomen. Dr. Kergaradec also suggested that fetal heart sounds could be used to determine fetal viability and proof of life in the months before ‘quickening’, that is, before the mother could feel the baby kick.
In 1833, an English physician, Dr. Evory Kennedy, published guidelines for fetal distress and also recommend auscultation of the fetal heart rate to monitor the well-being of the fetus during labor and birth.

A simple tool for counting the fetal heart rate
However, the big leap forward came in 1893, when Dr. Von Winkel established criteria for fetal distress. After listening to the heart rate of many babies during many labor, he realized that the FHR of an unborn baby in trouble would often (but not always) become abnormal, and beat much faster or much slower, or become extremely erratic. Some of these babies died before the birth, other were born profoundly depressed and often died later.
With this understanding, Dr Von Winkel identified the signs of fetal distress, which included abnormal fetal heart rates (FHR):
- tachycardia (a over 160);
- bradycardia (under 100),
- irregular heart rate, passage of meconium,
- abnormal fetal movement (i.e. agonal spasms of a dying baby).
By the turn of the 20th century, maternal fever was recognized as a cause of fetal tachycardia; head compression and cord compression were also known causes of bradycardia, and hyperstimulated uterine activity associated with an abnormal FHR patterns and asphyxia.
When these abnormal heart rates were discovered very late in the labor, doctors could sometimes perform a forceps delivery to rescue the baby. By the late 19th century, the development of general anesthesia, germ theory of infectious disease (resulting the principles of asepsis and sterile surgical techniques) made Cesarean surgery safe enough to use during labor to rescue babies with extremely abnormal heart rates.
 By the early 20th century — 50 years before fetal heart monitoring was electronically automated by a computerized machine — doctors, midwives and nurses were using a special stethoscope called a Pinard Horn to regularly listen to the heartbeat of the fetus during labor. Pinard fetal stethoscope was developed in the 1880s and in wide use in the 1950s.
By the early 20th century — 50 years before fetal heart monitoring was electronically automated by a computerized machine — doctors, midwives and nurses were using a special stethoscope called a Pinard Horn to regularly listen to the heartbeat of the fetus during labor. Pinard fetal stethoscope was developed in the 1880s and in wide use in the 1950s.
Helpful as this information was, there were still a few babies with apparently “normal” FHR that were born with unexpected and unexplained problems that prevented the baby from breathing on its own that resulted in death or severe handicaps.
At this early stage of development of fetal monitoring, auscultation was only used to count the heart rate for one minute (b.p.m, charted as a baseline for that period of time). However, birth attendants and nurses paid no attention to the rhythm of the fetal heart or other elements now known to be equally, if not even more important — variability, the presence of reassuring accelerations and absence of pathological decelerations, as well as the depth, timing, and duration of any decelerations that are detected.
 However, in 1922 Dr. Joseph De Lee, obstetrician, founder of the Chicago Lying-in Hospital and Chicago Maternity Center, invented, in conjunction with another obstetrician (Dr. David Hills) a hands-free fetal stethoscope for listening to fetal heart tones. This device became known as the DeLee-Hills Fetoscope.
However, in 1922 Dr. Joseph De Lee, obstetrician, founder of the Chicago Lying-in Hospital and Chicago Maternity Center, invented, in conjunction with another obstetrician (Dr. David Hills) a hands-free fetal stethoscope for listening to fetal heart tones. This device became known as the DeLee-Hills Fetoscope.
Then Dr. DeLee developed the process and protocols for the intermittent auscultation (IA) of the fetal heart rate during labor, which included Dr. Von Winckel’s 1893 description of fetal distress listed above. Using his new fetoscope, the FHR was to be auscultated every 30 minutes during first stage of labor, every three or five minutes during second stage, and continuously if signs of fetal distress were seen as an indication for forceps delivery.
In 1924, 4th edition of Dr. DeLee’s obstetrical textbook Principles and Practice of Obstetrics includes a wonderful graphic that displays a fetal heart rate auscultated and charted in 5-second increments during a minute-long contraction.
 It shows a normal baseline rate of 132 bpm at the beginning of the contraction (ranging from 120 to 144 bpm when computed in 5-second samplings) during the first 20 seconds. As pressure on the fetal head builds up, there is a head compression decel, and we can see the FHR go down from 144 to 108 bpm over a span of 20 second durning the middle of the contraction. As the contraction wanes and the uterus relaxes during the last 20 seconds, the unborn baby’s heart rate speeds back up to its pre-contracton normal baseline of 132.
It shows a normal baseline rate of 132 bpm at the beginning of the contraction (ranging from 120 to 144 bpm when computed in 5-second samplings) during the first 20 seconds. As pressure on the fetal head builds up, there is a head compression decel, and we can see the FHR go down from 144 to 108 bpm over a span of 20 second durning the middle of the contraction. As the contraction wanes and the uterus relaxes during the last 20 seconds, the unborn baby’s heart rate speeds back up to its pre-contracton normal baseline of 132.
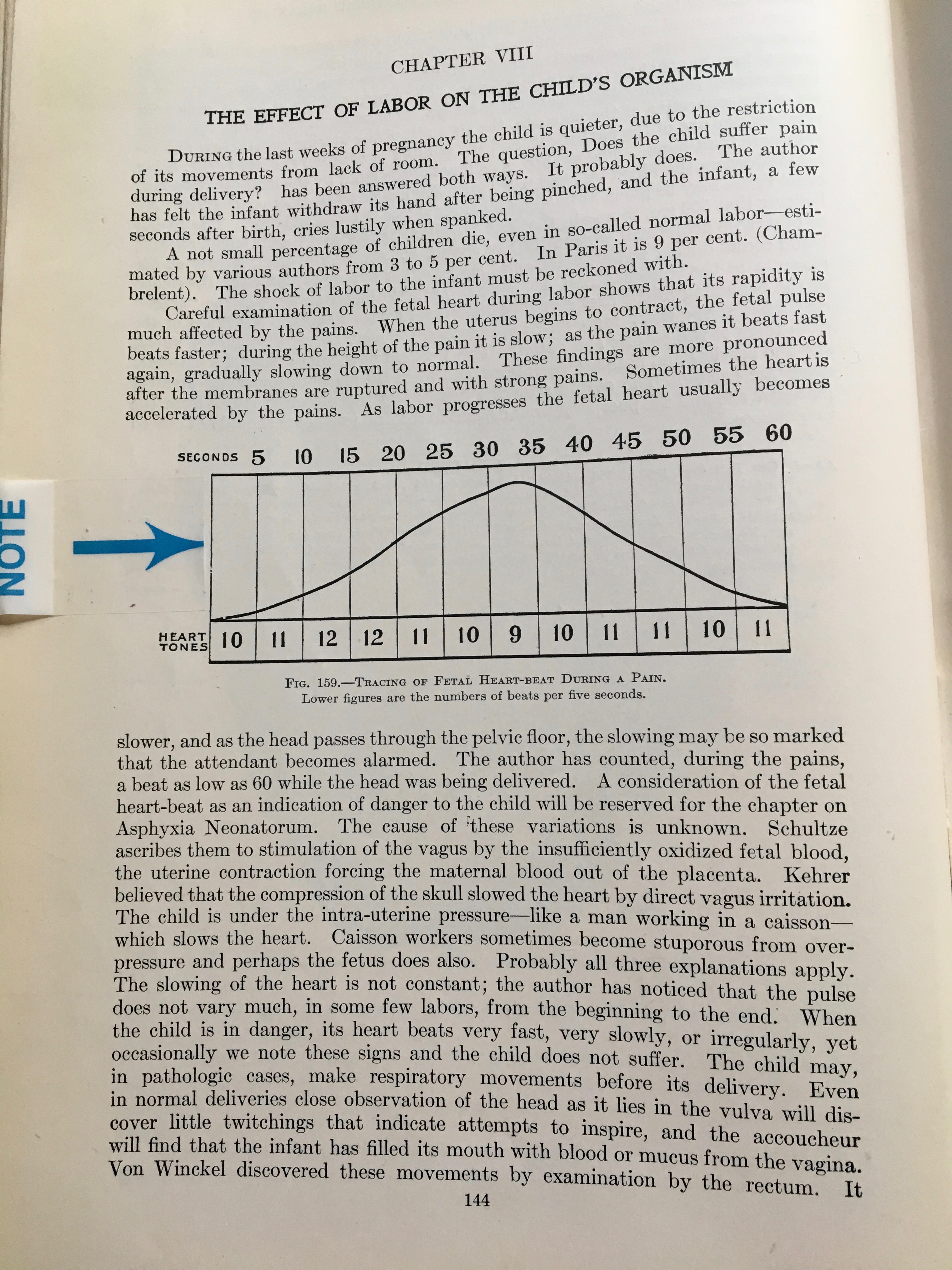
If you read Dr. DeLee’s comments below the picture of the graph, he refers to a pattern of decelerations during the pushing stage that we now know to be head compression decels — the result of triggering the mammalian diving reflex that has been extensively studied in whales.
Dr. DeLee somewhat anticipated this explanation by referring to the observed effect of an abnormally slow heart rate of men working deep under water in a “caisson” (a big metal contraption used during the underwater building of bridges and similar construction projects).
DeLee’s work is the theoretical precursor to both IA and EFM, as it is the first instance of dealing with variations in the FHR during the period of auscultation by using 5-second samplings. Prior to this, the only information on fetal heart activity that was gathered was the sum total of beats over 60 seconds period, which was stated as beats per minute (bpm) and recorded as a baseline rate.
Dr. DeLee recognized a second-level source of valuable information that could be gathered by paying attention to the FHR changes that occured (or failed to occur) within the one- or two-minute period that the FHR were routinely monitored by the L&D nurse, doctor or midwife.
The theoretical basis developed by Dr. DeLee and its 5-second sampling protocol, which yielded much a more useful picture of fetal wellbeing. This critical aspect of IA was widely not acknowledged or integrated into standard obstetrical practice until the development of electronic fetal monitoring equipment in the late 1950s and 60s.

If you are interested in learning how intermittent auscultations (IA) works, this link will take you to a subsequent stand-alone post on IA
Note: The historical background material on non-electronic fetal monitoring is repeated. To skip that part, keep scrolling down until you see this photo and the heading:”How IA Works“.
The invention of electronic automated fetal monitors and its displacement of IA
 With the clarity of hindsight, we now know that just recording the one-minute fetal baseline rate was not sufficient to identify subtle indicators of fetal distress.
With the clarity of hindsight, we now know that just recording the one-minute fetal baseline rate was not sufficient to identify subtle indicators of fetal distress.
In the decades before and after the ideas expressed in Dr. DeLee’s 1924 textbook, untold numbers of unborn babies unexpectedly ‘crashed’ during labor or were born severely depressed.
It’s not surprising that American obstetricians and worried parents continued to wonder if better information on the biological status of the fetus — a way to know what the fetal heart rate was during every minute of the entire labor & birth — would allow them identify unborn babies in trouble in time to rescue them before damage was done.
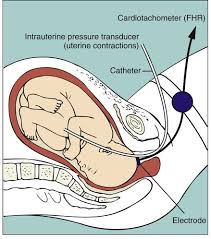
The very first attempt to record a FHR by using an electric machine came in 1906, which was when Dr. Cremer invented the first ‘fetal monitor’, which was an electro-cardiogram that used abdominal and intra-vaginal electrical leads. (!)
Other physician-inventors attempted to determine fetal status using a microphone to magnify the auscultated FHR and electronic phono-cardiography to record it. They ultimately decided that such devices could not provide the kind of consistent results that would allow them and other obstetricians to identify early indications of fetal distress.
But in 1958, Dr. Edward Hon, the pioneer of modern EFM, developed the first system for capturing continuously the fetal ECG and coined the terms early, late, and variable decelerations. I don’t know for sure that Dr. Hon knew about Dr. DeLee’s observations in the 1920s, but whether he did or not, he applied Dr. De Lee’s theories and methods.
In just five years (1964), Dr. Callagan had developed a commercially viable system for capturing the FHR with Doppler technology.

By the late 1960s, EFM systems by Dr. Hon were commercially available in the United States (1968). Other pioneers in these electronic systems include Dr. Hammacher in Germany who reduced noise-to-signal ratios and Dr. Caldeyro-Barcia from Uruguay, who was father of a number of fetal monitoring terms, including Montevideo units and long-term and short-term variability.
By the early 1970s, electronic fetal monitors had been purchased by 20% of hospital obstetrical units. Today, 100% of labor and delivery units have electronic fetal monitors and over 90% of hospital births include the use of c-EFM, along with an epidural anesthesia rate over 80%.
A web article called How to read a EFM on VeryWellFamily.com concluded its description of EFM (obviously from the perspective of hospitals) by saying that c-EFM:
“… also allowed the monitoring to be done without one-on-one care at the bedside.”
EFM: Really good for business
 Hospitals spend much more on electronic monitoring systems than handheld Dopplers. This is consistent with a decision NOT to hire enough nursing staff to do one-on-one intrapartum care that includes the use of IA.
Hospitals spend much more on electronic monitoring systems than handheld Dopplers. This is consistent with a decision NOT to hire enough nursing staff to do one-on-one intrapartum care that includes the use of IA.
- blood transfusions
- emergency hysterectomy
- postpartum infections
- rehospitalizations
- all the downstream emergencies:
-
- placenta percreta in future pregnancies that requires a Cesarean hysterectomy
- ICU admission for as long as to 20 days
- maternal death for 7 to 1o out of 100 women.
The routine use of electronic fetal monitoring as the standard of care for healthy women with normal pregnancies is high-tech, high-cost, non-evidence-based care. [EvidenceBasedBirth.com]
Since the first EFM was purchased by the first hospital, the push to expand c-EFM has been ever up, up, upward, irrespective of the science, damn the torpedoes, full speed ahead! There is no doubt that a constant pitch for buying the latest hot new upgrade is being driven by the EFM manufactures, for whom the sale of EFM equipment is so profitable.
Interestingly enough, the economic goals of EFM manufactures fit perfectly with those of hospitals, for whom billing insurance carriers and the federal *Medicaid program hundreds of dollars an hour makes the use of c-EFM into one of their favorite “cash cows”.
As for the health insurance industry, they can afford to reimburse hospitals at this extraordinary rate because it’s just a pass-through for premiums paid by their customers. Anytime the insurance carriers aren’t making as much profit as they want, they can hike premiums up to the moon and back and there is NOTHING we, the public, can do — we either pay or become uninsured. So “cost containment” is not a necessary aspect of health insurance as an unregulated industry.
[**Medicaid pays for half of all births in the US]
For hospitals, this profit-making scenario is the polar opposite of having to spend hundreds an hour to hire enough L&D nurses to provide one-on-one care (i.e. to ‘midwife’ as an active verb) each patient, using IA to monitor the fetus as an eyes-on, hands-on process performed in real time by a real person.
@@@@@@@@@@@@@@@@@@@@@
