Continuation ~ Part 1-B
Commonly used obstetrical interventions
and why their use is so often a problem
for the mother and also results in an
unplanned Cesarean surgery

The normal, but most painful, position for women laboring in the hospital and hooked up to an IV infusion of Pitocin
The standard obstetrical interventions used in virtually every hospital L&D unit start by putting the newly admitted laboring woman in a hospital bed. This is the most unnatural place of all to labor.
What childbearing women naturally do during labor is to move around a lot — walking around the house, spending time in the shower or bathtub, lying down for a little while. eating lightly and drinking frequently.

Depending on the time of day and or the weather, laboring women walking around in the backyard or their neighborhood.
The one thing laboring women naturally don’t do, and never benefit from is lying in a bed.
ELECTIVE INDUCTION OF LABOR
Making elective induction before the baby’s due date into the new obstetrical “norm” in the US
According to two studies done a few years ago in Europe, the neonatal mortality rate for births that occurred during the week before the mother’s official due date, there was a small statistical advantage for babies born during the 39th week of pregnancy.
The mortality rate for babies born during the seven days prior to the mother’s due date was 4 per 1,000, compared to 7 per 1,000 for babies born during the seven days that started with the mother’s due date. However, very large data sets like this can never predict what the outcome will be for any individual pregnant woman.
Nonetheless, the American obstetrical profession recommends that all healthy pregnant women with perfectly normal and healthy term pregnancies be electively hospitalized and induced during the week before their due date (i.e. 39 weeks) based on these two studies.
But unfortunately, there are a lot of problems with an obstetrical policy of inducing all pregnant women at 39 weeks.
 Being born before the due date may or may not have a small advantage for the baby, but any who has ever been induced, or provided care to pregnant women who were being induced before the childbearing woman’s body is ready to give birth spontaneously, has always and will always be a very much longer and much more painful labor, accompanied by a long list of labor-related interventions and statistically greater likelihood of an unplanned Cesarean surgery during the labor.
Being born before the due date may or may not have a small advantage for the baby, but any who has ever been induced, or provided care to pregnant women who were being induced before the childbearing woman’s body is ready to give birth spontaneously, has always and will always be a very much longer and much more painful labor, accompanied by a long list of labor-related interventions and statistically greater likelihood of an unplanned Cesarean surgery during the labor.
I have had seen more than one woman who was induced — a process that often took a couple of days and still resulted in an unwanted to necessary Cesarean delivery — that in the future they would just have a scheduled C-section.

For the pregnant woman, being induced means a much longer time in the hospital labor room while lying in a hospital bed while hooked up to an impressive number of medical and electronic paraphernalia.

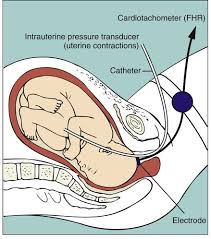
Being admitted to any hospital in America almost always (according to a Google search it’s 85% of the time) a
continuous electronic fetal monitor, known to fans of the Monty Python movie “The Meaning of Life” as “the machine that goes ping” strapped around her abdomen.
Being induced means having a needle in your arm connected to a plastic tube that goes up to one or more IV bottles designed to constantly drip Pitocin (sometimes also a saline solution or D5W) into your bloodstream.
There will also be an automatic blood pressure on one arm that goes off without warning about every 15 minutes, and a pulse oximeter on one of her fingers that glows in a way that is reminiscent of the extraterrestrial from outer space in the movie: “ET Call Home”.
Lying in bed hour after hour while hooked up to all this medical equipment is so miserable for the most labor patients that pretty soon everyone — patient, spouse, L&D nurse and the OB doctor — will all agree that epidural anesthesia is needed to get the mother-to-be through the many long hours of being trapped in bed while being inducted.
The hospital anesthesiologist soon appeared in the room and put an epidural catheter in the laboring woman’s back, which made the patient numb from the waist down. The anesthesia pump would be hooked up to yet another IV pole that huddled together at the top of her hospital bed.
But unfortunately, a side effect of being anesthetized from nipples to the knees is that the mother can no longer feel her bladder, which also means she can’t urinate spontaneously. The nurse will need to put in an indwelling Foley catheter in her bladder that will silently drain urine into a plastic pouch attached to her hospital bed for the remainder of her labor.
 Statistically she will be darn lucky if some spurious reading from the electronic fetal monitor — the second most frequent reason for doctors to do an emergency C-section on a first time mom during labor — or the doctor’s concern that she’s been pushing too long and “the baby maybe getting tired”.
Statistically she will be darn lucky if some spurious reading from the electronic fetal monitor — the second most frequent reason for doctors to do an emergency C-section on a first time mom during labor — or the doctor’s concern that she’s been pushing too long and “the baby maybe getting tired”.
Vacuuming the baby out when the mother gets too tired to push
 The first thing obstetricians do under these circumstances is use an obstetrical device known as a “vacuum extractor”. It is somewhat reminiscent of a miniature toilet plunger – a 4-inch around rubber cap that is attached to the unborn baby’s scalp at one end, while the other end is connected to a small hand-pump.
The first thing obstetricians do under these circumstances is use an obstetrical device known as a “vacuum extractor”. It is somewhat reminiscent of a miniature toilet plunger – a 4-inch around rubber cap that is attached to the unborn baby’s scalp at one end, while the other end is connected to a small hand-pump.
When it is repeatedly pumped, the vacuum extractor creates a strong suction on the top of the baby’s head that allows the obstetrician to pull the unborn baby down farther down, until the doctor can get his or her hands on the baby and extract it from its mother’s body.
I was present at a hospital birth in which the doctor asked the nurse to go get a vacuum extractor, but the mother delivered quickly and it was never used.
Since the package was opened, it was no longer technically “sterile” and would otherwise been thrown in the waste basket. However, I asked one of the nurses if I could keep it to demonstrate to my childbirth classes how a vacuum extractor worked, so she let me take it.
Not long after, I demonstrated how vacuum extraction worked to our childbirth education class. I pressed the round rubber vacuum disk that is usually attached to the top of the unborn baby’s head against the palm of my left hand. I was surprised and pleased that it fit so perfectly. Then I stated pumping the handle that sucked the very small amount of room air between my hand that the rubberized fetal “disk”.
But I was soon horrified to see that the suction being created between the palm of my hand and the suction disk (which usually is attached to the unborn baby’s head) was so very strong that collapsed the bones in my left hand – the ones that ran between my wrist at one end and my fingers at the other. In essence the natural “dome” that would naturally be the back of my hand was sucked inward until it created a depression or a hollow pit, something like a shallow sink hole in lawn.

Suction cup on the unborn baby head while the doctor pulls on the handle in an attempt to deliver the baby’s head
On that occasion, I concluded that it was wrong to believe that vacuum extraction was just a benign device — handy and yet “no big deal” from the standpoint of the baby’s head!
Instead I had another fact-based reason to insist that the “right use of gravity” is Mother Nature’s best gift to childbearing women, the best way to avoid the need to use medical and surgical instruments to ‘remove’ the baby from its mother’s body.
Pitocin, EFMs, and the hospital attorneys’ fear of litigation!
Whenever Pitocin is used to induce or speed up labor, electronic fetal monitoring is required by the hospital’s malpractice attorneys.
 If the baby goes into some kind of fetal distress and does poorly after its birth, lawyers hope the EFM tracing will be normal and therefore able to prove that it wasn’t the hospital or doctor’s fault.
If the baby goes into some kind of fetal distress and does poorly after its birth, lawyers hope the EFM tracing will be normal and therefore able to prove that it wasn’t the hospital or doctor’s fault.
Many of these same issues apply to the use of epidural anesthesia, which also obliterates the ability to make “right use of gravity” so not infrequently it results in additional obstetrical interventions such as Pitocin IV to make the labor more effective.
Unfortunately, when laboring women lie in bed for a protracted period of time, it sometimes triggers fetal distress and this usually means the baby will be delivered by emergency C-section.

Another one of the 85% of laboring women lying in a hospital bed while hooked up to a continuous EFM machinery.
As the “gift that keeps on giving”, a searching “Cesarean” on the Internet brings up pages of published studies that have identified 33 frequent complications and when unusual and rare complications are accounted for, there are more than 100 potential complications triggered by the Cesarean or its complications.
Complications inevitably require the use of more drugs, additional expensive and painful procedures, or surgery that often introduces new complications that so severe that the new mother is in the ICU for a month.
Cesarean Surgery ~ The gift that keeps on giving comes in three flavors
Starting with a genuine gratitude for the “rescue operation” known as “Cesarean section”
I thank Heaven that an effective rescue operation is available in serious emergencies, and am very glad that obstetricians are so good at performing this surgery.
But we all have to acknowledge that Cesareans are major abdominal surgery; they subject one out of every three childbearing women to host of present and future dangers that don’t apply to women who just have a normal vaginal birth.
In addition, Cesarean surgery is one of those quintessential “gifts” that keeps on “giving”, in that they are directly and indirectly associated with a very long list of serious and even fatal complications.
Nonetheless, two-thirds of all Cesarean surgeries done in the United States very likely not to be medically necessary. As a L&D room nurse in the late 1960s and early 1970s (before electronic fetal monitoring was invented), our hospital’s annual C-section rate had a low of only 3% and high of only 5%.
Unfortunately, Cesarean surgery changes the childbearing woman’s life forever. Publication that compared maternal outcomes for Cesarean delivery with vagina birth identified 33 serious complications associated with C-sections compared to only 4 for vaginal birth.
As bad as that is, a Google search of the medical literature has uncovered an even longer and more far-reaching list of complications associated with Cesarean surgery and the most obvious medical issue arising from this long-standing obstetrical policy:
“Once a Cesarean, always a Cesarean”.

The “Cesarean” problem that plagues the United States and many other wealthy industrialized countries is the overuse and inappropriate use of surgical delivery for reasons that are beneficial to doctors and hospitals, but unfortunately introduce unnecessary dangers to the childbearing woman and her baby.
The “wrong use” of Cesarean surgery
Only 5 -to-10% of Cesarean surgeries are medically necessary — that is, done to save the life and wellbeing of the mother or baby or both.
When Cesarean surgery replaces normal spontaneous childbirth, mothers and babies are always exposed to a substantial increase in complications, including emergency hysterectomy, a prolonged stay in the hospital’s Intensive Care Unit for mother or baby (or both) and unexpected death. Exposure to these higher risks begins with the “primary” surgery and continues in all post-Cesarean pregnancies and births.
There is a long list of complications associated with Cesarean surgery. Time-wise, these problems fall in the three categories noted earlier — immediate, delayed and downstream. Some occur immediately, others are delayed by a few days or weeks, while downstream complications don’t occur for many weeks, months, or even years later. These serious but not-lethal complications fall in the category of substantial morbidity.
When the situation is uncommonly dangerous for mother or baby, Cesarean surgery is the only rational choice.
Elective Cesarean surgery is dangerous and therefore an irrational choice
However, the “elective” use of Cesarean based on personal or professional “convenience” for hospitals, doctors and/or childbearing women is irrational. It opens up a “can of worms” with consequences that can reach far into the future and be unbelievably expensive for all the parties involved. If there is an unexpected “bad outcome”, it will quickly turn into the “gift” that keeps on giving, as the mother or baby is hospitalized for a long time, and all the lawyers line up to sue anyone even slightly involved in making decisions and providing care.
Cesarean surgery and its complications
There are three distinct categories of complications that are directly and indirectly associated with Cesarean surgery. (A) Immediate, (B) Delayed and (C) Downstream

Intraoperative and
Immediate post-op dangers include:
Hemorrhage,
Blood transfusions,
Pulmonary embolism,
Accidental cutting of a ureter* {*the biological tube that connects to each kidney to the mother’s bladder}
ICU admission, and up to a month’s stays in the ICU, while her newborn is in the hospital nursery or sent home to be cared for by family members.
Downstream complications include a 6% rate of secondary infertility rate
One of the most worrisome post-operative problems are abdominal adhesions, in which the woman’s abdominal organs quite literally get functionally “glued” together by the “free blood” left in the mother’s abdomen after the surgeon sutured each of the 7 layers of the abdominal wall.
Small amounts of blood leaking from the many small blood vessels cut during the surgery can and often do cause adhesions. Instead of the mother’s abdominal organs (particularly intestines and bladder) being slippery, they will be somewhat glued together and every time she sneezes it causes a painful twinge.
One of the reasons this list is so long is that the majority of unplanned Cesarean are done on first-time mothers who go on to have other pregnancies. This opens Pandors’s box in all post-Cesaean pregnancies and births and repeat Cesaean deliveries”.
This brings us to the very important issue of “VBAC” or Vaginal BIrth After Cesarean. This was and continues to be a big and very controversial topic, with many debates and arguments within and without the obstetrical and midwifery professions. I have already written extensively about the issue of several posts about the social, psychological and obstetrical issues that surround Vaginal BIrth After Cesarean.
This lose-lose situation does NOT have to be the “business as usual” for childbearing families in America. No one wants the first month of their newborn’s life to be in the hospital nursery while their new mother is being treated for unexpected complications in the hospital’s ICU.
This foolish system has never been the “norm” in Japan, European countries and most other parts of the world. This not only wastes lives and destroys families, but obstetrical interventions and their complications often cost society a small fortune.
Part 1-a; link to the part 1B
@@@@@@@@@@@@@@@@@@@@@@@@@@
AI search list for the most
frequent complications
of Cesarean surgery
Google search term used: “risks of elective c-section”
Materal and infant risks of elective C-section:
Maternal Risks:
-
-
Anesthesia: Complications from rapidly administered anesthesia
- Bleeding: Heavy bleeding during or after surgery, sometimes requiring a blood transfusion
- Blood clots: Increased risk of deep vein thrombosis or pulmonary embolism, including formation of a blood clot in the leg or deep vein thrombosis that could be life-threatening
- Cardiac arrest: A risk associated with emergency C-sections
- Injury: Injury to the organs, nerves, or blood vessels near the uterus, as well as damage to nearby organs such as the bladder, ureters, or intestines
- Increased risk of future surgeries, such as hysterectomy
- Infection: Risk of infection at the incision site, in the uterus, or urinary tract
- Placental problems: Increased risk of placenta previa or accreta in future pregnancies.
-
- Prolonged recovery: Longer hospital stay and slower return to daily activities
- Uterine rupture: .A risk associated with emergency C-sections, especially if there have been previous cesarean deliveries. The risks and complications of post-Cesaean vaginal birth includes:
-
- Not being able to deliver vaginally in the future
- Longer hospitalization
- Pain and discomfort for many days after the operation
- The incision can be sore for weeks after the C-section
Other risks to the childbearing woman
- **********************************************************************************
Risks to Newborns: - Respiratory problems ~ Increased risk of respiratory distress syndrome, especially if born prematurely.
- Accidental injury: The baby may be accidentally injured during the C-section
-
-
- Injuries: Rare but possible, such as cuts or bruises during surgery.
-
-
-
- Developmental problems: Studies have shown a slightly increased risk of asthma and allergies in children born by elective cesarean section.
-
Important Take Away
C-sections can save lives when indicated, but they’re riskier than vaginal delivery if they’re not indicated or done for the right reasons.
@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@

