HEADLINE NEWS ~ Planned places-of-birth — hospitals, independent birth centers and planned home births — are all associated with some increased risks of morbidity and mortality in healthy women with normal pregnancies when compared to the outcomes achieved in each of these other settings.
The logical response to these facts is to acknowledge the problem and work together to reduce its incidence in each respective setting.
Only if all childbirth complications were consistently lower than these same problems in the other settings could a particular setting be identified as a clearly superior choice. But this is not true for either hospitals or OOH birth. Nor do these two setting have an equal occurrence of the same types of maternal-infant problems, as what goes wrong is often very different, depending on the setting. The grass is definitely not greener on either side of this fence.
Luckily, the most serious complications associated with childbirth in healthy women are remarkably rare in both hospitals and OOH settings. However, studies show that certain of the more common complications occur more often in one planned place-of-birth, while being significantly lower in the other setting. This goes both ways — certain complication are more frequent in hospitals than OOH, while a different set of complications are more frequent in OOH settings that they are in hospitals.
For planned hospital birth, many site-specific complications are associated with the high rate of obstetrical interventions, which is 2 to 10-fold greater than OOH setting. In far too many instances, the negative side-effects and unintended consequences of a particular intervention is greater than the intended benefit.
One of the setting-specific issues for hospitals is the high rate of Cesarean surgery; the obstetrical profession publicly acknowledges the Cesarean section is an “over-used” intervention but also states that the changing practice habits of obstetricians also is not easy. Nonetheless, medical problems that result from medical decisions or treatments are legally defined as ‘iatrogenic’ (when doctor-related) and/or nosocomial (when hospital-related).
The fundamental problem for Cesarean overuse in hospital labors is that medical schools in the US have not taught the principles or technical skills associated with the physiological management of normal labor since the late 19th century. As members of a surgical discipline, American obstetricians have not personally attended labor throughout the entire 20th century. They generally have little or no experience with the physiologic support of normal childbirth. In addition, most physiological strategies for stimulating a better labor pattern or help the baby’s head to descend during the pushing stage CANNOT be used when women had had an epidural. Under such circumstances, obstetricians see the
Under this situation — obstetricians with no training or experience in the use of physiological support for normal labor and a labor that is not progressing as determined by current obstetrically- defined criteria — Cesarean delivery is generally seen by American obstetricians as the only logical available option, and given such constraints, it often is.
However, the lack of obstetrical training in the physiological management of normal labor and birth in healthy women can be rectified by American medical schools again teaching the principles and practice of curriculums. The incorrect assumption that the ever-increasing medicalization of healthy women makes childbirth safer for them and their babies can be recognized as inaccurate (i.e. not an evidence-based practice) by the American College of Obstetricians and Gynecologists. As the spokesperson for the surgical specialty of obstetrics and gynecology, ACOG could, if it chose, challenge the
As the spokesperson for the surgical specialty of obstetrics and gynecology, ACOG could, if it chose, challenge the very unhelpful legal theory that it would be a form of ‘substandard’ or negligent care for an obstetrically-trained surgeon to provide (or provide for) the physiological management of labor and birth in a healthy woman who was not asking for or need medical interventions.
Statistical Significance in scientific studies & problems
To paraphrase the American Heritage New Dictionary of Cultural Literacy, 3rd Edition, definition of “statistical significance” when used in a statistical anaylsis ,is:
“a number that expresses the probability that the result of a given experiment or study could have occurred purely by chance. This number can be a margin of error [example: “The results of this public opinion poll are accurate to 5%”], or it can indicate a confidence level [example: [“If this experiment were repeated, there is a probability of 95% that our conclusions would be substantiated”].
Scientific studies on the relative safety of childbirth practices or planned places-of-birth often report numbers of ‘bad outcomes’ (adverse events) that are higher in one ‘arm’ (group) of the study than the other. For example, a Canadian study published in 2002 (quoted below) reported there were 3 neonate deaths in the PHB groups while there was only one in the hospital group and yet — crazy as it seems — stated truthfully and accurately that there was no “statistically significant” difference in neonatal mortality between the two groups.
Statistical significance relative to maternity care is the idea that whatever outcome was identified in the study (likelihood of having a vaginal birth, cesarean delivery, serious morbidity or mortality for mother or baby, etc) can be determined to be the result of the specific type of care or treatment provided or the setting of the labor and birth and was NOT just chance or a fluke of some kind. {click here for another post with additional explanation}
While this is an accurate “fact”, more information is needed before readers of these studies can understand this concept and what it means to them personally.
Perinatal mortality is so statistically rare in both settings that it often does not rise to the level of “statistical significance” in population-based studies. This is why the findings of published studies so frequently state that for professionally-attended births no difference (that is, no statistically significant difference) was detected for either hospital or OOH settings.
However, childbearing should have both types of information — the incidence (i.e. actual number) of morbidity and mortality specific to each setting as well as all statistically significant conclusions.
To assist childbearing families to make informed decisions consistent with their goals and values, they should receive this kind of well-balanced and scientific accounting of the risks and benefits for each birth setting — without any fear tactics or intimidation — for hospitals, independent birth centers, and planned home births.
Comparisons between hospital and OOH groups for essentially healthy women with normal pregnancies show significantly different rates for the following:
(a) normal vaginal births
(b) Cesarean deliveries
(c) immediate, delayed and downstream complications subsequent to Cesarean surgery
(d) number and frequency of obstetrical interventions used
(e) maternal postpartum morbidity –> mother requiring blood transfusion due to PP hemorrhage
(f) higher maternal mortality
(g) neonatal morbidity –> baby requiring 24 hours of assisted ventilation
(h) higher perinatal mortality (unexpected/unexplained intrapartum and neonatal deaths)
Planned OOH Birth for healthy women with normal pregnancies
OOH Increased Risks for mothers and babies
The intrapartum hospital transfer rate for laboring women varies from a low of 2% to as high at about 20%.
Compared to planned hospital births, some (but not all) published research on OOH birth shows an increase in perinatal morbidity, (such as assisted ventilation of 24 or more hours {P. Jansen BC 1999}. The OOH setting also has an average increase in perinatal mortality of approximately one per 1,00o births.
The obstetrical profession attributes the slightly lower rate of intrapartum and neonatal deaths in hospitals to electronic fetal monitoring, which is used routinely on 90-plus percent of women for approximately 90% (or more) of the time the mother is in labor.
The great majority of birth attendants who provide care in OOH settings do not routinely use continuous electronic fetal monitoring (EFM). In fact, the largest accrediting organization for free-standing birth centers owned and run by CNMs, do not allow the use of continuous EFM. Lack of continuous may or may not explain the small number of additional deaths when compared to hospital care of the same cohort of healthy women.
New mothers who delivered OOH also have an increased rate of postpartum hemorrhage requiring emergency transport and blood transfusions. The issue here is time. In an OOH setting, access to advanced medical and surgical services requires physical transport (awaiting the arrival of EMS, two-way driving time for the ambulance, etc); this generally delays certain vital emergency measures such as providing blood transfusions or surgical interventions.
Decreased Risks & benefits to mothers and babies in OOH settings
The spontaneous vaginal birth rate for OOH locations varies from a 90% to 98%, with an average of about 93%. (California Licensed Midwives Annual Report – 2007-2015, cohort of approximately 40,000 births).
Most childbearing women who choose an OOH setting (home or birth center) consider that its advantages include continuity of care, birth attendant physically present during all stages of the intrapartum (active labor, birth, immediate postpartum-neonatal period)who is trained, skilled and experienced in the principles of physiologic support and management of common variations of normal. These attributes include patience with nature, the absence of artificial time limitations, and acknowledging the normal need for privacy experienced by many women during labor.
In an OOH settings women laboring are normally encouraged to be active, upright and mobile during all stages of labor. This reduces the likelihood of a stalled labor or that the baby will assume an unfavorable position. In addition, these mothers consistently receive one-on-one care and encouragement from familiar caregivers and family members.
Support for normal labor normally includes use , non-drug methods of pain relief such as therapeutic touch, hot showers, and immersion in deep-water tubs during 1st stage. During 2nd stage, OOH birth attendants make right-use-of-gravity by encouraging maternal mobility, upright postures, squatting and/or use of a birth stool.
In OOH setting, the rate of medical interventions that is 2 to 10-times less than hospitals, with a C-section rate is under 10 % compared to over 30% for hospitals.
The MMR is also lower for OOH than hospitals with a similarly healthy low-risk cohort of women.
Planned Hospital Birth for healthy women with normal pregnancies
Increased Risk for mothers and babies in hospital births
Management of labor and birth in hospitals is provided by two different professions. A professional nursing staff manages the labor while staying in contact with the doctor by phone for updates and whenever the mother has a question or the nurse notices a problem. When the baby is about to be born the physician-obstetricians is called in to conduct the surgical procedure of “vaginal delivery”, or in many cases, to perform Cesarean surgery or other types of operative delivery (forceps or vacuum).
Compared to independent birth centers and planned home births, hospitals are associated with 2- to 10-times higher rate of obstetrical interventions (used in 99% of all hospitalized labor patients), increase serious morbidity that includes Cesarean-related complications and a small number of deaths in subsequent pregnancies.
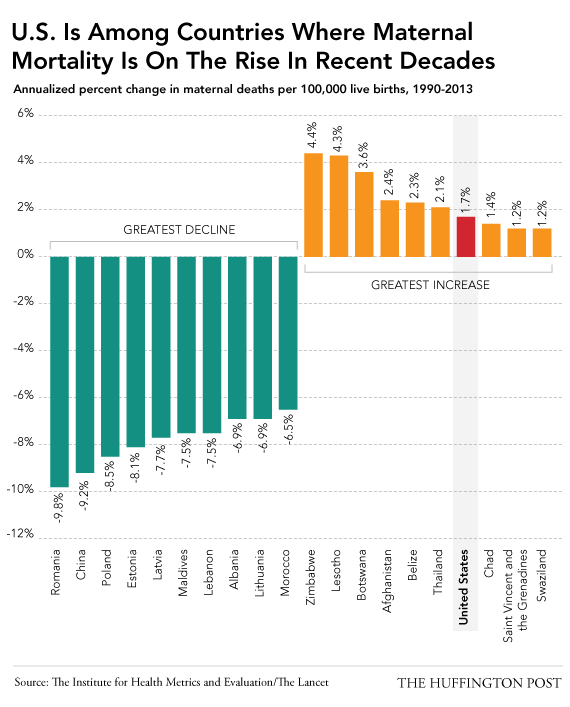
Hospitals have a generally increased rate of maternal deaths in healthy women as contrasted with OOH birth services and with other developed countries (MMR in the US currently ranks 60th worldwide).
However, hospitals do enjoy a reduced rate of (1) perinatal mortality and (2) severe postpartum hemorrhage compared to OOH settings.
Decreases Risks and benefits to mothers and babies having a hospital birth
On the up-side, reduced perinatal morbidity and mortality in hospitals appears to be associated with the routine use of continuous electronic fetal monitoring and a very liberal policy of performing Cesarean surgeries for abnormal EFM tracing. The obstetrical profession frequently refers to this customary practice as “when in doubt, cut it out”. At least one study (Jansen, 1999) found that the number of babies born spontaneously to healthy women that subsequently required assisted ventilation for 24-hours or longer was less frequent in hospital births.
The other improved outcome associated with hospitals as the planned place-of-birth is a reduced number of several PP hemorrhages after a spontaneous vaginal birth. A study of 2,177 healthy women that compared matched outcomes for both home and hospital births noted that 3 of the 4 women in the study that required a blood transfusion were in the PHB arm.
However, these two specific categories of improved outcomes for the hospital management of normal birth in healthy women also had a decided downside. Compared to OOH settings, the rate of medical interventions used in hospitals on healthy women are 2 to 10-times greater with a C-section rate over 30%, compared to under 10% to for OOH.
A significant level of increase in hospital interventions and Cesarean surgeries is seen ever when the labor and birth is attended by a hospital midwife. It appears that many of these troubling issues are location-specific (found in hospital birth but not OOH settings) which is to say, they not based on the category of birth attendant (physician vs. midwife).
Double-edged sword: Continuous Electronic Fetal Monitoring (EFM)
The most central and most controversial obstetrical intervention in American hospitals is continuous EFM. Continuous electronic monitoring is nearly universal in spite of 40 years of studies that found the only statistically significant outcomes of EFM was a consistent rise in the rate of Cesareans in laboring women who were electronically monitored.
Click here to read NEJM paper on EFM that provides a brief history and explanation of EFM, the problematic fact that is was universally implemented before any research was published, and that 20 or more studies concluded that universal use of EFM has not lowered the cerebral palsy rate at all, that EFM is NOT more effective than intermittent auscultation (listening with a fetoscope or doppler) and that the use of EFM during labor is associated with a consistent and considerable increase in the rate of Cesareans.
The other consequential obstetrical intervention use in over 50% of hospital labors is induction or augmentation of labor with the drug Pitocin. This requires starting maintaining an IV on the mother, which make mobility a problem. The use of Pitocin during labor is strongly associated with fetal distress. Due to this high level of risk associated with its use, obstetrical protocols worldwide mandate continuous electronic monitors as long as a Pitocin IV is running.
As recorded in the operative notes, the second most frequently reason for performing a C-section is an abnormal EFM tracing (23%). However only 3.1% of babies born by Cesarean are determined to be suffering from fetal distress at birth based on low Apgars and other criteria. [Consensus on Obstetrical Care series — Safe Prevention of the Primary Cesarean Delivery — ACOG, 2014]
As mentioned already, the MMR in the US ranks 60th (i.e. women in 59 other countries are safer). In fact, the US is one of only 8 countries, and the ONLY developed country, that currently has a rising MMR.
But that is not the only problem with a C-section rate that is 2 or 3 times more CS than seems reasonable. For every maternal death, 50 mothers experience serious morbidity requiring prolonged hospitalization, admission to an ICU and other medical treatment that make it impossible to nurse one’s newborn. The rate of re-readmission to the hospital after discharge is much higher. Other post-Cesarean problems are sometimes permanent. For example, an emergency hysterectomy is 13-times more frequent after a Cesarean section.
This conversation continues in the next post, which had links to 2 additional documents.
This posts address the issue of “statistical significance”, informed consent, and changes in the curriculum of American medical schools (teaching the principles of physiological management) and also changing the legal definition of an obstetrician’s ‘standard of care’ to include the use of physiological management techniques and timelines relative to ‘normal progress’.
This would help to close the gap btw hospital-based obstetrics and OOH midwifery care, which in turn would make care available to healthy childbearing women seeking normal childbirth services that are both safer and more satisfactory for all involved (including care providers and hospitals)
