How I became a time-traveler, a storyteller and “idiot savant” on the unnecessary often dangerous medicalization of normal birth by the obstetrical profession in the United States over the course of the 20th century and why this story still matters today to every American
Easy Shortcut to share –> https://tinyurl.com/y8pgewkg
The information in this 8-part series on Dr. Williams (original author of Williams’ Obstetrics) is a crucial element in an even bigger historical tale that I describe as:
“The Last and Most UNTOLD Story of the 20th Century: How Healthy Pregnant Women were turned into the patients of a surgical speciality and normal childbirth into a surgical procedure ‘performed’ by obstetrically-trained surgeons“
A Brief Introduction
I have been a professional maternity care provider my entire adult life as a labor and delivery room nurse and childbirth educator, and later on as a professional midwife, preceptor of midwifery students, and legislative activist. My fascination with childbearing began at the tender age of 18, as a nursing school student.
My first job after graduation was working as a labor and delivery room nurse during the “knock’em-out-drag’em-out” era of American obstetrics. The routine use of twilight sleep drugs — narcotics and scopolamine (an amnesic and hallucinogenic drug) was the standard policy of hospitals everywhere from the early 19o0 until the late 1970s.
Whenever our L&D wasn’t busy, I passed the time by reading old obstetrical textbooks brought in by older doctors and kept on a shelf behind the nurses’ station. This informal library was a time-capsule of obstetrical practices from 1900 to the late 1960s.
My study of American obstetrics as a surgical speciality and its opposite — the non-interventive or ‘physiological’ management of normal childbirth as provided by midwives and old-fashions country doctors — became the driving force in my own personal and professional story and gave energy and direction to my life’s calling.
I was fascinated by the childbirth practices of 20, 50 or 100 years ago, and how things changed or didn’t change, which was the case for Twilight Sleep drugs given to laboring women, the routine use of general anesthesia, episiotomies and forceps to pull the baby out.
 {Link to an “Journal BIRTH A Time-Traveler’s Perspective 0n Normal Childbirth_Sept-11-2011′ published in the journal BIRTH September 2011 about my experience and insights as an L&D nurse during this period}
{Link to an “Journal BIRTH A Time-Traveler’s Perspective 0n Normal Childbirth_Sept-11-2011′ published in the journal BIRTH September 2011 about my experience and insights as an L&D nurse during this period}
After 15 years of trying unsuccessfully to have a positive impact on this dangerous and inhumane system (and often being referred to by our OBs as that “witch” and fired more than once for “meddling” in their business), I finally called it quits and cross-trained into midwifery.
I have been practicing as a California Licensed Midwife since 1996. In 2007, I was appointed to the Medical Board’s Midwifery Advisory Council and served as the Council’s first Chair for three years. In 2013 I resigned to work on legislation amending the California Licensed Midwives Practice Act.
Over the last four decades, I have devoted nearly all of my spare time to researching the deep history of obstetrics in America, which is dramatically different than childbirth practices used around the world.
Luckily, I live within biking distance of the Stanford University campus and had access to the medical school’s library (Lane Library) and its collection of very old obstetrical textbooks. The author of a historical textbook published in 1837 (“Midwifery and Churgery” {old spelling of ‘surgery’}) was particularly interesting.
It’s author was extremely critical of the growing trend in the medical profession of his day to misuse of emergency interventions, in particular, the manual removal of the placenta, as a way to quickly end the 3rd and final stage of labor. Instead of waiting the normal 10 to 20 (occasionally 30-60) minutes for the placenta to be expelled normally by the mother, many doctors routinely did a manual removals of placenta so they could leave immediately after the baby’s birth.
In the relatively rare cases of maternal hemorrhage, this drastic intervention can be a life saving, but manual removal of a placenta is a dangerously invasive intervention that dramatically increases the likelihood of a fatal infection and/or a delayed but fatal postpartum hemorrhage. To remove the placenta from the mother’s uterus, the doctor must insert his hand and lower forearm thru the mother’s vagina and up into her uterus. Then he use the tips of his fingers in an effort to pry the still adherent placenta off the uterine wall.
We must remember that this 1837 textbook was published nearly half a century before medical science discovered that microscopic organisms unseen by the naked eye — bacteria and other forms of pathogens — were the cause of infection and were highly contagious.
Doctors did not understand that invisible bacteria on their ungloved hands was the direct cause of the deadly “childbed fever”, a fatal infection that frequently killed new mothers. This also was happening long before the invention of rubberized surgeon’s exam gloves, before doctors knew to wash and disinfect their hands both before and after every patient encounter and any invasive or surgical procedure, and more than 150 years antibiotics became available to civilians in the United States, when penicillin first became made available to the general public on March 15, 1945.
The author of this 1837 medical textbook was high critical and outspoken about the harm being caused by doctors who routinely doctors to procedures developed as emergency interventions to make the birth go faster. This is an obvious example of “the more things change, the more they stay the same“, since the exact same comment applies to today to the use of Pitocin to speed up first stage labor, operative deliveries to truncate the normal second stage and routinely removing the placenta manually.
All these previous emergency intervention had become the standard of care which was till in use when i worked in the L&D units of 4 different hospitals in central Florida after graduating from nursing school in the 1960s and 70s.

Laboring woman given Twilight Sleep drugs. Protocol called for blocking all “stimulations” which meant putting a hood or mask over the mother’s face to block light and sound
Brief Aside on the historical origin of our modern-day “cascade of obstetrical interventions”
From the old obstetrical textbooks in the stacks of Stanford’s medical Lane Library, I was able to discovered the origin of the chain of events that we now call the “cascade of interventions” that starts in the early 19th century with routinely intervening in the 3rd stage (expulsion of the placenta) to hurry things along so the doctor would leave.
In the early 20th century, doctors began to routinely intervene in 2nd stage of labor using episiotomy and forceps. Later in the 20th century Cesarean replaced forceps as the preferred way to truncate 2nd stage labor.
By the mid-20th century, the first stage of labor came under attack when the drug Pitocin — a uterine stimulant — was marketed in 1953. At first Pitocin was used sparingly and mainly to treat excessive bleeding and postpartum hemorrhage. By the early 1970s obstetrician started ordering nurses to give subcutaneous injections of very small amount of Pitocin (0.5 to 2.0 miniums in a TB syringe) every 20 minutes to speed up a slow labor or occasionally to induce labor.
By the 21st century, the only possible childbirth-related interventions left were elective Cesareans done for the convenience of either doctor or mother and the routine elective induction of labor as the new ‘standard of care’. Based on the dubious idea that it is ‘safer’ for the baby to be born before its due date, obstetrical practices are electively hospitalizing healthy pregnant women during the 39th week of pregnancy (normal pregnancy is 40 weeks) and routinely inducing labor. They claim this does not increase the CS rate but very good data says otherwise.
Here is how this happened and its consequences for the childbearing woman.
Beginning in the late 1700s, very first obstetrical intervention on this list was turning the emergency procedure of manually removing the placenta during the 3rd stage of labor into an intervention used routinely by doctors .
To remove the placenta from the new delivered mother’s uterus requires the doctor to stick his hand and lower part of his forearm up through her vagina and into her uterus and use his fingers to peel the placenta off the wall of the uterus. This way the doctor no longer required to wait the usual 20-30 minutes of waiting for the placenta to be spontaneously expelled by the mother.
Manual removal of the placenta also introduces dangerous bacteria, but unfortunately, this was 75 years before the Germ Theory of Infectious Disease (1881) became public. At this time doctors did not realize that putting their hands in the mother’s vagina often introduced deadly bacteria; when the physician’s ungloved hand and lower arm are thrust into the uterus, any bacteria or other pathogens have direct access to the mother’s blood stream. This childbirth-related infection was called “childbed fever” (i.e., septicemia) and resulting in the death of newly-delivered women.
The obstetrician-author of that 1837 textbook noted with great disdain that:
For every one mother such a doctor saves from the danger of a postpartum hemorrhage by manually removing the placenta, this invasive obstetrical procedure is responsible for dangerous complications and even death for a hundred other women who did not need or benefit from the shortcut taken by the doctor.
The next stage in this re-branding of an obstetrical emergency intervention to routine procedures was the use forceps to shorten the 2nd stage in first-time mothers. Typically, these women pushed for 30 minutes to 3 hours, while a forceps delivery might only take 5 or 10 minutes, thus saving doctors a couple hours of his time for each and every forceps delivery.
For women who had given birth before, episiotomy was routinely used to hasten the birth, so the doctor didn’t have to spend his valuable time watching while the mother pushed and pushed.
Last but not least, the new medical science of the early 20th century finally provided doctors with ways to shorten the first stage of labor by giving injections of the drug pituitrin, which makes the uterus contract more frequently and more strongly, which substantially increases the speed at which the cervix is dilated.
Then in 1953, the pharmaceutical company Park Daviss developed a synthetic oxytocin (the Rx drug “Pitocin”), which could not only speed up labors, but could be used routinely for labor induction. Now doctors could induce their patients with Pitocin whenever they were planning to go out of town or on vacation. This model of obstetrics is remarkable for its ever-increasing rate, timing and invasiveness of obstetric interventions.
Learning how and why medical and surgical interventions were turned into a routine part of ‘normal’ childbirth helped me understand the obstetrical profession’s historical relationship with normal childbirth and midwifery and specifically how it combined to produce our 20th and 21st system of highly medicalized, interventive and our unproductively expensive “American Way of Birth“.
When you add up the routine (i.e. preemptive) use of previously emergency-related interventions from 3rd state, then to 2nd , then to 1st stage labor and now inducing labor and performing elective Cesarean surgeries), you can clearly understand why the US has the worst maternal mortality rates in the developed world.
The cumulative effect of a dozen or more risky procedures used routinely in early labor and birth often creates iatrogenic (medical provider-related) and nosocomial (hospital-related) complications — that is, preventable morbidity (disability) and mortality (death of mother or baby). The numbers don’t lie — we are the only wealth country that a high and continue to climb maternal mortality rate. Shame on us!
The Shocker — It’s ever so much worse than I imagined
 Nothing in my study of old obstetrical textbooks prepared me for the stunning information in discovered in a book written by Dr. J. Whitridge Williams for the lay public and published in 1914. Twilight Sleep: Simple Discoveries in Painless Childbirth.
Nothing in my study of old obstetrical textbooks prepared me for the stunning information in discovered in a book written by Dr. J. Whitridge Williams for the lay public and published in 1914. Twilight Sleep: Simple Discoveries in Painless Childbirth.
This out-of-print book only became available in modern times after being scanned and posted online in 2008 by the Google Library project. Because the two Google founders (Sergey Brin and Larry Page) were Stanford graduates, they chose Stanford medical library as first collection to be scanned and posted on the Internet.
Twilight Sleep contains a wealth of compelling and previously unknown facts about the obstetrical profession in America during the early decades of the 20th-century. This particular historical period was marked by an acrimonious turf war between gynecology, which was a surgical specialty, and obstetrics, which has always been a medical discipline.
My paradigm-shifting breakthrough was the result of the Google Library Project.

For “delivery”, women were strapped into metal stirrups
Dr. Williams’ book also reveal why obstetrical medicine in the US became a surgical speciality and how it subsequently interfaced with healthy childbearing women and the profession of midwifery by re-branding childbirth – even in the healthiest of women — a dangerous biological event that could only be made safe by turning into a surgical procedure and trying to eliminate the lawful practice of midwifery.
Dr. William’s amazing book was the most important source of information on WHY obstetricians in the early 20th century turned healthy childbearing women into “patients” of their surgical speciality and re-named and re-configured the spontaneous act of giving birth as a conscious act of the mother into a surgical procedures “performed” by the obstetrician on women rendered unconscious under general anesthesia.
The Medical Practice of Obstetrics marries the Surgical Speciality of Gynecology
At that time, there was two types of licensing for MDs — ‘physician’ and ‘surgeon’. In contemporary language, we would describe a physician as an “internist”, while doctors licensed as “surgeons” were only trained in surgery, and knew nothing about the general practice of medicine.
 As a non-surgical medical practice, the services provided by these doctors was much closer to midwifery. Since the care provided by midwives was denigrated on as mere “woman’s work“, the professionalism of doctor who attended normal births was likewise derided by gynecologists.
As a non-surgical medical practice, the services provided by these doctors was much closer to midwifery. Since the care provided by midwives was denigrated on as mere “woman’s work“, the professionalism of doctor who attended normal births was likewise derided by gynecologists.
In particular, gynecological surgeons could perform a cesarean section, while medical doctors could do nothing more in an emergency than the lowly midwife.
This tension between the two professional discipline lead to frequent disputes over the legal right of medical doctors to do forceps deliveries. Gynecological surgeon also argued with doctors who called them to perform a Cesarean, claiming they didn’t contacted was soon enough to assure a good outcome.
Frequent arguments between the doctors and surgeons were both frequent and extremely acrimonious, with name-calling, insults, and plenty of hard feelings. When tempers reached the boiling point, an occasion punch was thrown and the resulting black-eye an embarrassment to both professions.
To stop this unproductive hostility, influential leaders of both professions decided to combine the non-medical discipline of obstetrics with gynecological surgery to form the new American hybrid surgical specialty of obstetrics and gynecology.
Dr. J. Whitridge Williams’ Dream
Although Dr. J. W. Williams was trained as a gynecological surgeon in the late 1800s, served as chief of obstetrics for more than a decade, and authored “Williams Obstetrics” (the most famous obstetrical textbook in America), the practice of ob-gyn was no longer his all-consuming passion. In his new role as Dean of Johns Hopkins’ School of Medicine, he dreamed of a modern nationwide system of full-service general hospitals in the US like ones used for the last 200 years in Western European countries.
The European hospital systems provided medical and surgical care to patients of all ages and types of problems or disease. These big general hospitals were sponsored by the national government, supported by public taxes, and had large, state-run bureaucracies that managed institutions in each geographical area and population center.
In addition, public hospitals in Western Europe have played a central role in medical education for several centuries. Poor and homeless patients received free medical care in exchange for became ‘teaching cases’. This pool of the ill and injured provided opportunities for clinical training to hundreds of medical students each year.

Johns Hopkins University Hospital in the very early 1900s, where Dr. Williams was Chief of Obstetrics and later Dean of the JH’ medical school
The insurmountable problem for Dr. Williams was how to create the same kind of general hospital system in the US without involving or depending in any way on the federal government or any ‘nationalized’ bureaucracy. The American medical profession pejoratively defined all types of nationally-supported system as ‘socialized medicine’ because it reduced the role of doctors to ‘mere’ employees of the system.
The AMA thoroughly despised and vilified any form of government funding (and its bureaucratic control over doctors), so that kind of funding would never be accepted by the American medical profession. Dr. Williams had to really “think outside the box”.
But Dr. Williams’ was undaunted, determined, and filled with an entrepreneurial zeal. One day he became inspired and figure out an effective “workaround” that, as the saying goes, killed two birds with one stone. He did this by inventing a brand new category of hospital patient — the electively hospitalized healthy childbearing woman of ‘means’ (middle or upper-class) as a paying customer.
This turned out to be a double whammy that was even more satisfying he could imagine at first. Without ever involving state or federal governments (and its suffocating bureaucracies), his plan created a dependably profitable revenue stream which handsomely paid for the actual cost of care (which was very low) and the remaining profit available to build a nationwide general hospital system.
But even more exciting, the idea of ‘elective hospitalization’ allowed general hospitals to exchange the money-losing model they were historically stuck with (i.e. sick and injured people die or become disabled and can’t work, thus can’t pay) for a dependably profitable, market-based economic model on a par with any other business.
Fatal Fly in the Ointment
But Dr. JWW’s little book also provided irrefutable evidence that his profound enthusiasm and emotional investment in his big “Plan” dramatically interfered with his ethical judgment. As a result, he drastically misrepresented important facts (“alternative facts” in today’s lingo) at a level that would be considered unethical, if not actually criminal. Unfortunately for all of us, this propaganda campaign of mis- and dis-information became the raison d’etre for the new surgical specialty of hospital obstetrics as the “modern” American standard for all childbearing women.
For the entire 20th century, these new hospital policies and obstetrical protocols consistently caused enormous harm to healthy laboring women who lost ground every time their normal biology was disrupted by a hospital protocol or medical or surgical intervention and at same time, these interventions exposed them and their unborn baby to the risks and side-effects of unnecessary medical and surgical procedures.
A potentially deadly roll of the dice

Midwife providing postnatal care in early 1900s
In 1931, Testimony on the efficacy of midwifery care was presented to the White House Conference on Child Health and Protection by the Committee on Prenatal and Maternal Care: Dr. Reed concluded:
~”…that untrained midwives approach and trained midwives surpass the record of physicians in normal deliveries has been ascribed to several factors. Chief among these is the fact that the circumstances of modern practice induce many physicians to employ procedures which are calculated to hasten delivery, but which sometimes result in harm to mother and child. On her part, the midwife is not permitted to and does not employ such procedures. She waits patiently and lets nature take its course.” (original emphasis)
In 1932, an American physician and statistician for the Metropolitan Life Insurance Company calculated that 70,000 maternal-infant deaths could be prevented each year — 10,000 mothers, 30,000 stillbirths, and 30,000 newborns — if the quality of professional midwifery care provided by the Kentucky Frontier Nurse-midwifery program was made available to all healthy childbearing women in the United States.
“In 1933, the New York Academy of Medicine published a shocking study of 2,041 maternal deaths in childbirth. ”
“At least two-thirds, the investigators found, were preventable. There had been no improvement in death rates for mothers in the preceding two decades; newborn deaths from birth injuries had actually increased. Hospital care brought no advantages; mothers were better off delivering at home with a professionally trained midwives.
Investigators were appalled to find that many physicians simply didn’t know what they were doing: they missed clear signs of hemorrhagic shock and other treatable conditions, violated basic antiseptic standards, tore and infected women with misapplied forceps. The White House followed with a similar national report. Doctors may have had the right tools, but midwives without them did better.”
{{ Annals of Medicine The Score: How childbirth went industrial” By Atul Gawande }}
 But the obstetrical profession’s stubbornly ignored this advice. Their refusal to provide physiologically-based childbirth services to healthy women (or allow professional midwives to do so) resulted in thousands of unnecessary maternal deaths from the routine use general anesthesia (3rd leading cause of maternal mortality in 1960), postpartum hemorrhage and infection.
But the obstetrical profession’s stubbornly ignored this advice. Their refusal to provide physiologically-based childbirth services to healthy women (or allow professional midwives to do so) resulted in thousands of unnecessary maternal deaths from the routine use general anesthesia (3rd leading cause of maternal mortality in 1960), postpartum hemorrhage and infection.
Hundreds of thousands of newborn babies suffered permanent brain damage as a result of the narcotics and other drugs given repeatedly to their mothers during labor (and causing respiratory depression at birth), and the routine use of forceps during delivery.
Childbirth-related deaths and permanent injuries in essentially healthy women and babies occurred year after year, from the early 1900s until the mid-1940s. That is when several scientific breakthroughs in medicine made it possible to treat previously fatal iatrogenic complications caused by unwise and unnecessary obstetrical interference in normal childbirth. These life-saving developments included the antibiotic drug penicillin to treat hospital-acquired infections in new mothers, better anesthesia to prevent anesthetic-related deaths, safer blood transfusions to treat hemorrhages following routine manual removal of placentas and generally improved surgical techniques developed on the battlefield during WWII.
The profession of obstetrics continues to reject and vilify normal childbirth practices (physiologically-based care) in 2018
Sadly, Dr. J. Whitridge Williams’ original ideas still form the bedrock of 21st-century American obstetrics. While our contemporary problems are not so grim or drastic as those in the 1920s or 30s (before the discovery of antibiotics), routine obstetrical interventions are still associated with preventable mortality and morbidity in previously healthy mothers and their newborn babies. But this is a well-kept secret, as it’s rare for the public to find out that these childbirth-related deaths were preventable. Instead, they are blamed on the women themselves for being older or fatter, or having some mysterious or undiagnosed medical problem.

Dr. Williams’ book reveals the basic economic motive behind the new profession’s troubling relationship with normal childbirth. It was during this historical period that healthy pregnant women were identified as the patients of a surgical specialty and normal childbirth became a surgical procedure to be ‘performed’ by doctors trained in obstetrical surgery.
For this reason, I refer to this situation as the last and most important UNTOLD story of the 20th century.
The danger associated with using obstetrical intervention routinely during the care of healthy women with normal pregnancies must become common knowledge. Then so we can build on the actual strengths of modern obstetrical medicine, which are substantial and life-saving when disengaged from their inappropriate use on healthy women, while we work to eliminate the profession’s historical errors.
A Truth and Reconciliation Commission to heal the hurt and hostility between the obstetrical profession, consumer groups of healthy childbearing women, and physiological management by non-obstetrician birth attendants
To bring about the level of change that is needed will require some version of a “Truth and Reconciliation Commission” in which the earlier errors are acknowledged and a structure put in place to keep them from being repeated.
 The eventual goal is a maternity care system for healthy women with normal pregnancies that is based on physiological principles and practices. Normal childbirth services for healthy women will be provided by professional midwives and family practice physicians in the setting chosen by the parents; obstetrical intervention will be reserved for women who develop a complication or if an informed mother-to-be requests medical treatments or surgical procedures.
The eventual goal is a maternity care system for healthy women with normal pregnancies that is based on physiological principles and practices. Normal childbirth services for healthy women will be provided by professional midwives and family practice physicians in the setting chosen by the parents; obstetrical intervention will be reserved for women who develop a complication or if an informed mother-to-be requests medical treatments or surgical procedures.
End of Intro, Continue to Part !
Part 1: The Dream, the Motives, the Methods & Enduring Impact of 1914 book
“Twilight Sleep ~ Simple Discoveries in Painless Childbirth ~
by famous American obstetrician: Part 1-a ~ Overview
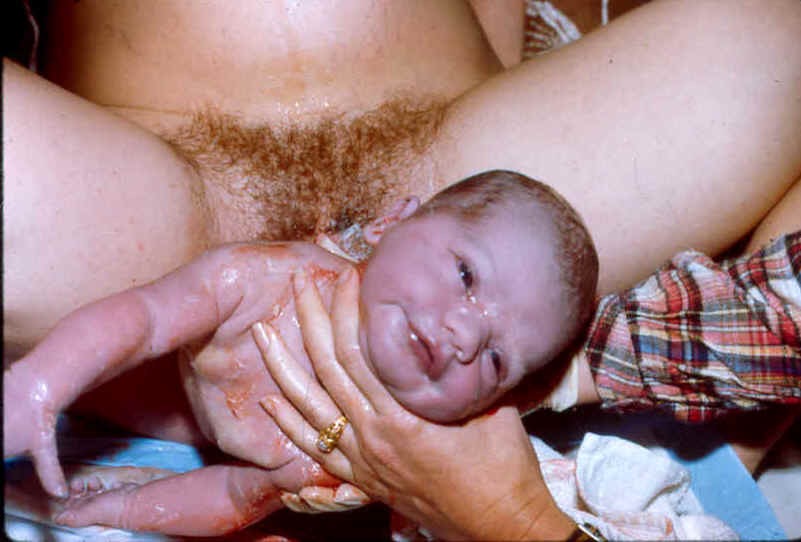
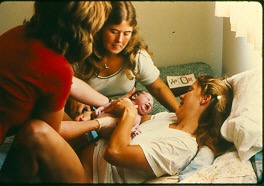
Photographs of Healthy Mothers, Normal Childbirth:
Mothers pushing their babies under their own power,
babies as a conscious being at the time of its birth